
Articles
- Page Path
- HOME > Acute Crit Care > Volume 39(1); 2024 > Article
-
Original Article
Pediatrics Outcomes of extracorporeal membrane oxygenation support in pediatric hemato-oncology patients -
Hong Yul An1,2
 , Hyoung Jin Kang1,2, June Dong Park1
, Hyoung Jin Kang1,2, June Dong Park1 -
Acute and Critical Care 2024;39(1):108-116.
DOI: https://doi.org/10.4266/acc.2023.01088
Published online: January 24, 2024
1Department of Pediatrics, Seoul National University College of Medicine, Seoul, Korea
2Cancer Research Institute, Seoul National University College of Medicine, Seoul, Korea
- Corresponding author: June Dong Park Department of Pediatrics, Seoul National University College Of Medicine, 103 Daehak-ro, Jongno-gu, Seoul 03080, Korea Tel: +82-2-2072-3359 Fax: +82-2-743-3455 E-mail: jdparkmd@snu.ac.kr
© 2024 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,129 Views
- 91 Download
Abstract
-
Background
- In this study, we reviewed the outcomes of pediatric patients with malignancies who underwent hematopoietic stem cell transplantation (HSCT) and extracorporeal membrane oxygenation (ECMO).
-
Methods
- We retrospectively analyzed the records of pediatric hemato-oncology patients treated with chemotherapy or HSCT and who received ECMO in the pediatric intensive care unit (PICU) at Seoul National University Children’s Hospital from January 2012 to December 2020.
-
Results
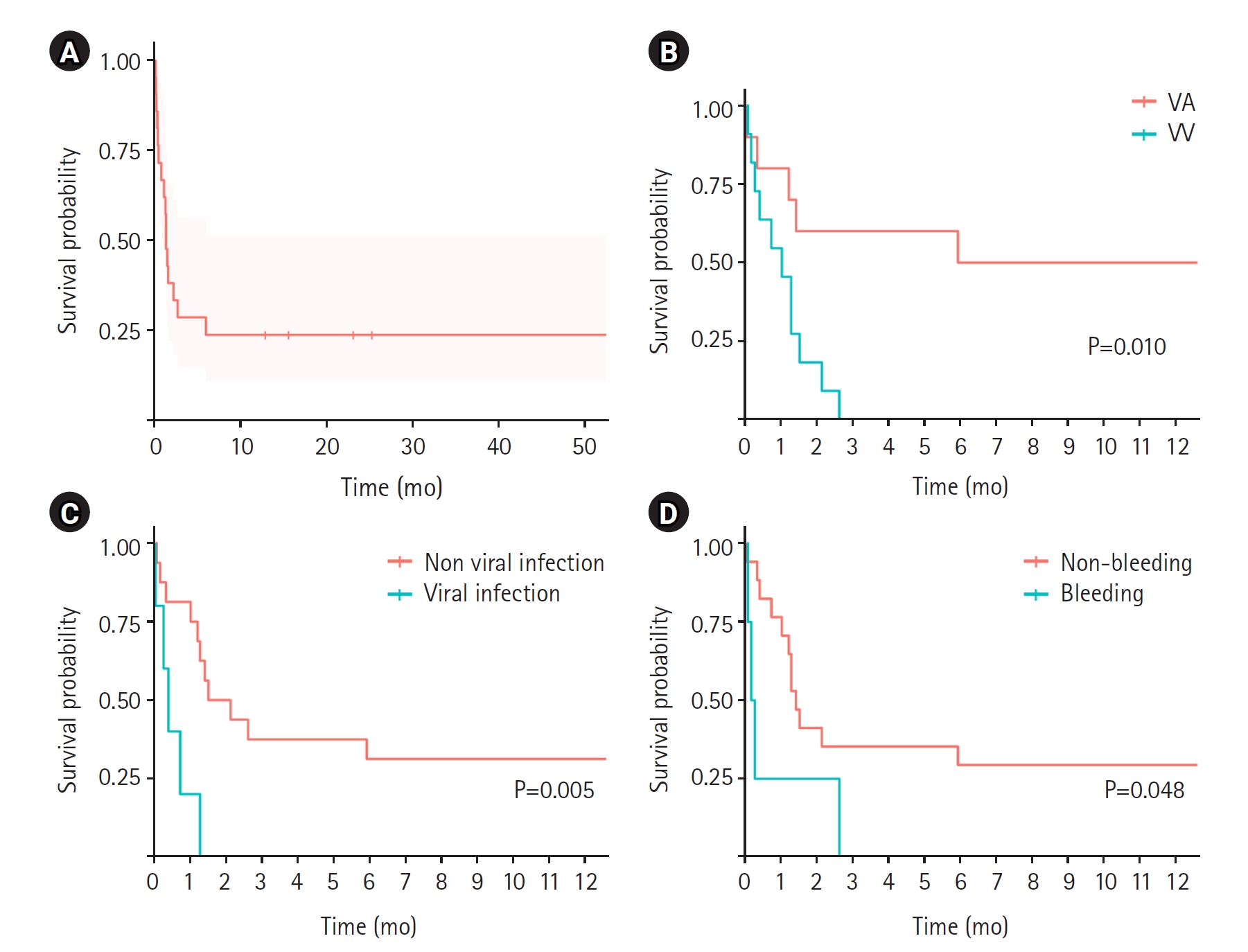
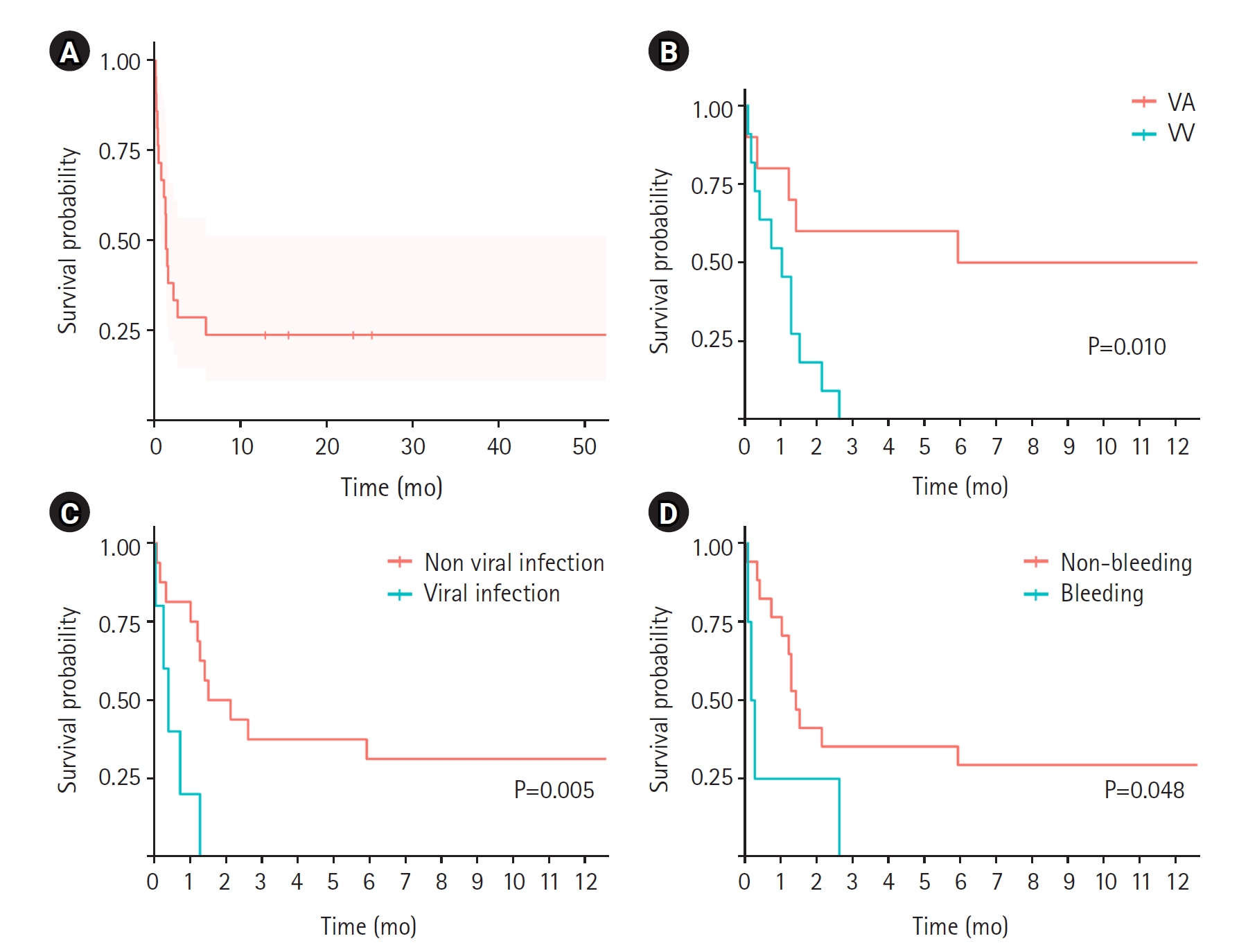
- Over a 9-year period, 21 patients (14 males and 7 females) received ECMO at a single pediatric institute; 10 patients (48%) received veno-arterial (VA) ECMO for septic shock (n=5), acute respiratory distress syndrome (ARDS) (n=3), stress-induced myopathy (n=1), or hepatopulmonary syndrome (n=1); and 11 patients (52%) received veno-venous (VV) ECMO for ARDS due to pneumocystis pneumonia (n=1), air leak (n=3), influenza (n=1), pulmonary hemorrhage (n=1), or unknown etiology (n=5). All patients received chemotherapy; 9 received anthracycline drugs and 14 (67%) underwent HSCT. Thirteen patients (62%) were diagnosed with malignancies and 8 (38%) were diagnosed with non-malignant disease. Among the 21 patients, 6 (29%) survived ECMO in the PICU and 5 (24%) survived to hospital discharge. Among patients treated for septic shock, 3 of 5 patients (60%) who underwent ECMO and 5 of 10 patients (50%) who underwent VA ECMO survived. However, all the patients who underwent VA ECMO or VV ECMO for ARDS died.
-
Conclusions
- ECMO is a feasible treatment option for respiratory or heart failure in pediatric patients receiving chemotherapy or undergoing HSCT.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
KEY MESSAGES
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: all authors. Data curation: HYA. Formal analysis: HYA. Methodology: HYA. Project administration: all authors. Visualization: HYA. Writing–original draft: HYA. Writing–review & editing: all authors. All authors read and agreed to the published version of the manuscript.
NOTES
Acknowledgments
SUPPLEMENTARY MATERIALS
Supplementary Figure 1.
HSCT: hematopoietic stem cell transplantation; ECMO: extracorporeal membrane oxygenation; RRT: renal replacement therapy; CPR: cardiopulmonary resuscitation; ICU: intensive care unit; NA: not available; ARDS: acute respiration distress syndrome; PCP: pneumocystis carinii jirovecii; VA: veno-arterial; Y: yes; N: no; rBMT: related bone marrow transplantation; uCBT: unrelated cord blood transplantation; CMV: cytomegalovirus; VV: veno-venous; uPBSCT: unrelated peripheral blood stem cell transplantation; aPBSCT: autologous peripheral blood stem cell transplantation; IRAB: imipenem resistant Acinetobacter baumannii; hPBSCT: haploidentical peripheral blood stem cell transplantation; AML: acute myeloid leukemia.
- 1. Zabrocki LA, Brogan TV, Statler KD, Poss WB, Rollins MD, Bratton SL. Extracorporeal membrane oxygenation for pediatric respiratory failure: survival and predictors of mortality. Crit Care Med 2011;39:364-70.ArticlePubMed
- 2. von Bahr V, Hultman J, Eksborg S, Gerleman R, Enstad Ø, Frenckner B, et al. Long-term survival and causes of late death in children treated with extracorporeal membrane oxygenation. Pediatr Crit Care Med 2017;18:272-80.ArticlePubMed
- 3. Jenks CL, Raman L, Dalton HJ. Pediatric extracorporeal membrane oxygenation. Crit Care Clin 2017;33:825-41.ArticlePubMed
- 4. Coleman RD, Goldman J, Moffett B, Guffey D, Loftis L, Thomas J, et al. Extracorporeal membrane oxygenation mortality in high-risk populations: an analysis of the pediatric health information system database. ASAIO J 2020;66:327-31.ArticlePubMed
- 5. Slooff V, Hoogendoorn R, Nielsen JS, Pappachan J, Amigoni A, Caramelli F, et al. Role of extracorporeal membrane oxygenation in pediatric cancer patients: a systematic review and meta-analysis of observational studies. Ann Intensive Care 2022;12:8. ArticlePubMedPMCPDF
- 6. Gupta M, Shanley TP, Moler FW. Extracorporeal life support for severe respiratory failure in children with immune compromised conditions. Pediatr Crit Care Med 2008;9:380-5.ArticlePubMed
- 7. Gow KW, Heiss KF, Wulkan ML, Katzenstein HM, Rosenberg ES, Heard ML, et al. Extracorporeal life support for support of children with malignancy and respiratory or cardiac failure: the extracorporeal life support experience. Crit Care Med 2009;37:1308-16.ArticlePubMed
- 8. Leahey AM, Bunin NJ, Schears GJ, Smith CA, Flake AW, Sullivan KE. Successful use of extracorporeal membrane oxygenation (ECMO) during BMT for SCID. Bone Marrow Transplant 1998;21:839-40.ArticlePubMedPDF
- 9. Fan K, Hurley C, McNeil MJ, Agulnik A, Federico S, Qudeimat A, et al. Case report: management approach and use of extracorporeal membrane oxygenation for diffuse alveolar hemorrhage after pediatric hematopoietic cell transplant. Front Pediatr 2020;8:587601. ArticlePubMedPMC
- 10. Kebudi R, Oflaz Sozmen B, Bahar M, Paker T, Hacı I, Ekinci A, et al. Prolonged extracorporeal membrane oxygenation in pediatric leukemia with severe acute respiratory distress syndrome and persistent fungemia. Pediatr Blood Cancer 2021;68:e28966.ArticlePubMedPDF
- 11. Prabhu AD, Mos K, Karl TR, Anderson B. Extracorporeal life support in the acute management of tumour lysis syndrome. Interact Cardiovasc Thorac Surg 2012;15:568-9.ArticlePubMedPMC
- 12. Olson TL, O'Neil ER, Kurtz KJ, MacLaren G, Anders MM. Improving outcomes for children requiring extracorporeal membrane oxygenation therapy following hematopoietic stem cell transplantation. Crit Care Med 2021;49:e381-93.ArticlePubMed
- 13. Suzuki Y, Kugelmann A, Cass S, Radhakrishnan R. Extracorporeal membrane oxygenation for pediatric patients with malignancy: outcomes and trends in the last decade. J Am Coll Surg 2021;233:S293-4.ArticlePMC
- 14. Potratz JC, Guddorf S, Ahlmann M, Tekaat M, Rossig C, Omran H, et al. Extracorporeal membrane oxygenation in children with cancer or hematopoietic cell transplantation: single-center experience in 20 consecutive patients. Front Oncol 2021;11:664928. ArticlePubMedPMC
- 15. Ranta S, Kalzén H, Nilsson A, von Schewelov K, Broman LM, Berner J, et al. Extracorporeal membrane oxygenation support in children with hematologic malignancies in Sweden. J Pediatr Hematol Oncol 2021;43:e272-5.ArticlePubMed
- 16. Cortina G, Neu N, Kropshofer G, Meister B, Klingkowski U, Crazzolara R. Extracorporeal membrane oxygenation offers long-term survival in childhood leukemia and acute respiratory failure. Crit Care 2018;22:222. ArticlePubMedPMCPDF
- 17. Steppan DA, Coleman RD, Viamonte HK, Hanson SJ, Carroll MK, Klein OR, et al. Outcomes of pediatric patients with oncologic disease or following hematopoietic stem cell transplant supported on extracorporeal membrane oxygenation: the PEDECOR experience. Pediatr Blood Cancer 2020;67:e28403.ArticlePubMedPDF
- 18. Kang HS, Rhee CK, Lee HY, Kim YK, Kwon SS, Kim SC, et al. Clinical outcomes of extracorporeal membrane oxygenation support in patients with hematologic malignancies. Korean J Intern Med 2015;30:478-88.ArticlePubMedPMCPDF
- 19. Di Nardo M, Ahmad AH, Merli P, Zinter MS, Lehman LE, Rowan CM, et al. Extracorporeal membrane oxygenation in children receiving haematopoietic cell transplantation and immune effector cell therapy: an international and multidisciplinary consensus statement. Lancet Child Adolesc Health 2022;6:116-28.ArticlePubMed
- 20. Di Nardo M, MacLaren G, Schellongowski P, Azoulay E, DeZern AE, Gutierrez C, et al. Extracorporeal membrane oxygenation in adults receiving haematopoietic cell transplantation: an international expert statement. Lancet Respir Med 2023;11:477-92.ArticlePubMed
- 21. Smith S, Butt W, Best D, MacLaren G. Long-term survival after extracorporeal life support in children with neutropenic sepsis. Intensive Care Med 2016;42:942-3.ArticlePubMedPDF
- 22. Di Nardo M, Locatelli F, Palmer K, Amodeo A, Lorusso R, Belliato M, et al. Extracorporeal membrane oxygenation in pediatric recipients of hematopoietic stem cell transplantation: an updated analysis of the Extracorporeal Life Support Organization experience. Intensive Care Med 2014;40:754-6.PubMed
- 23. Gow KW, Wulkan ML, Heiss KF, Haight AE, Heard ML, Rycus P, et al. Extracorporeal membrane oxygenation for support of children after hematopoietic stem cell transplantation: the Extracorporeal Life Support Organization experience. J Pediatr Surg 2006;41:662-7.ArticlePubMed
References
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-
- Related articles
-
- Plasma biomarkers for brain injury in extracorporeal membrane oxygenation
- Risk factors for cannula-associated arterial thrombosis following extracorporeal membrane oxygenation support: a retrospective study
- Outcomes of patients with COVID-19 requiring extracorporeal membrane oxygenation and continuous renal replacement therapy in the United States
- Awakening in extracorporeal membrane oxygenation as a bridge to lung transplantation

