
Articles
- Page Path
- HOME > Acute Crit Care > Volume 36(3); 2021 > Article
-
Review Article
Meta-analysis The efficacy of vitamin C, thiamine, and corticosteroid therapy in adult sepsis patients: a systematic review and meta-analysis -
Manoj Kumar Reddy Somagutta1
 , Maria Kezia Lourdes Pormento1, Muhammad Adnan Khan1, Alaa Hamdan1, Namrata Hange1, Manish KC1, Sukrut Pagad1, Molly Sanjay Jain2, Sivasthikka Lingarajah3, Vishal Sharma3, Jaspreet Kaur4, Bernard Emuze2, Erkan Batti5, Obumneme Jude Iloeje6
, Maria Kezia Lourdes Pormento1, Muhammad Adnan Khan1, Alaa Hamdan1, Namrata Hange1, Manish KC1, Sukrut Pagad1, Molly Sanjay Jain2, Sivasthikka Lingarajah3, Vishal Sharma3, Jaspreet Kaur4, Bernard Emuze2, Erkan Batti5, Obumneme Jude Iloeje6 -
Acute and Critical Care 2021;36(3):185-200.
DOI: https://doi.org/10.4266/acc.2021.00108
Published online: June 30, 2021
1Department of Clinical and Translational Research, Larkin Community Hospital, South Miami, FL, USA
2Department of Medicine, Saint James School of Medicine, Park Ridge, IL, USA
3Department of Medicine, Windsor University School of Medicine, Cayon, St. Kitts and Nevis, USA
4Department of Medicine, Medical University of Silesia, Katowice, Poland
5Department of Medicine, Washington University of Health and Science, San Pedro, Belize
6Department of Medicine, University of Health Sciences, Antigua, Antigua and Barbuda
- Corresponding author Manoj Kumar Reddy Somagutta Department of Clinical and Translational Research, Larkin Community Hospital, 7031 SW 62nd Ave, South Miami, FL 33143, USA Tel: +1-773-289-2848 Fax: +1-773-289-2848 E-mail: manojleo.go@gmail.com
Copyright © 2021 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
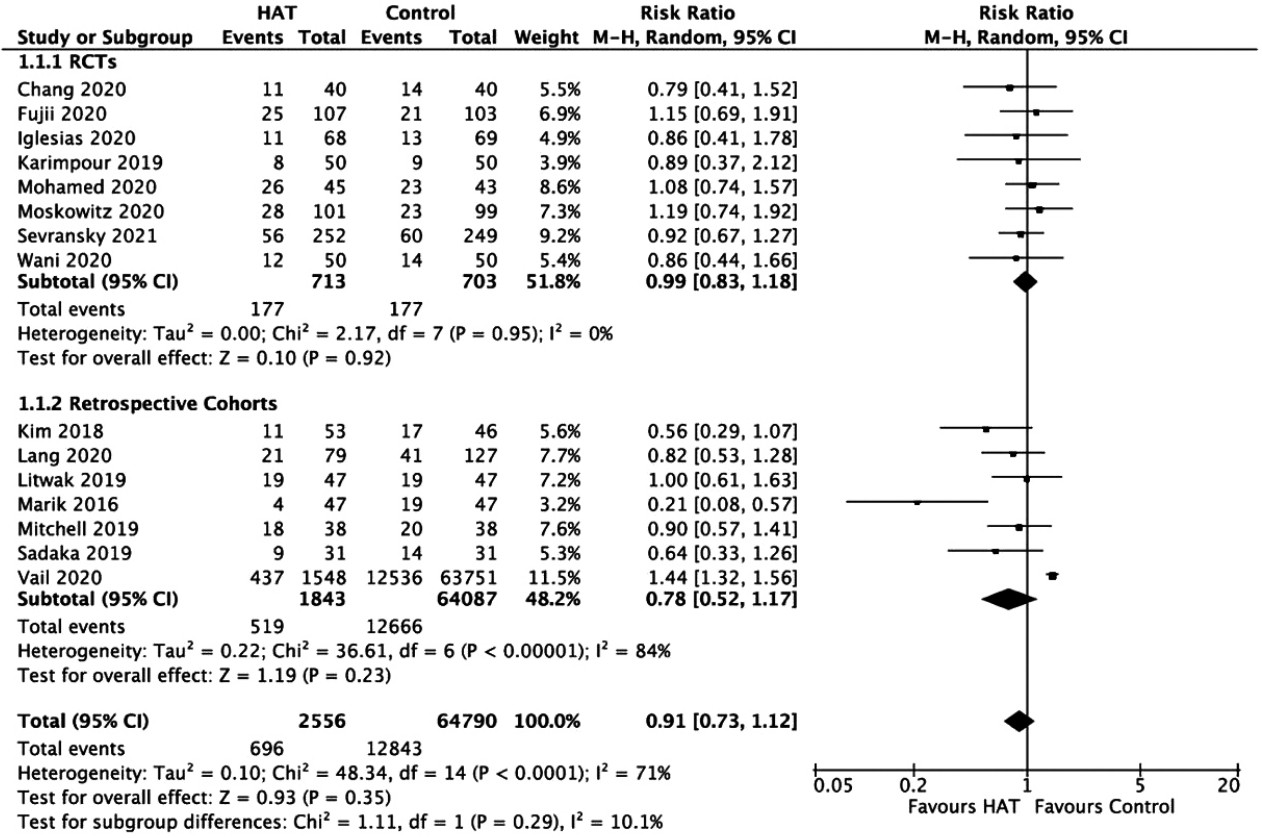
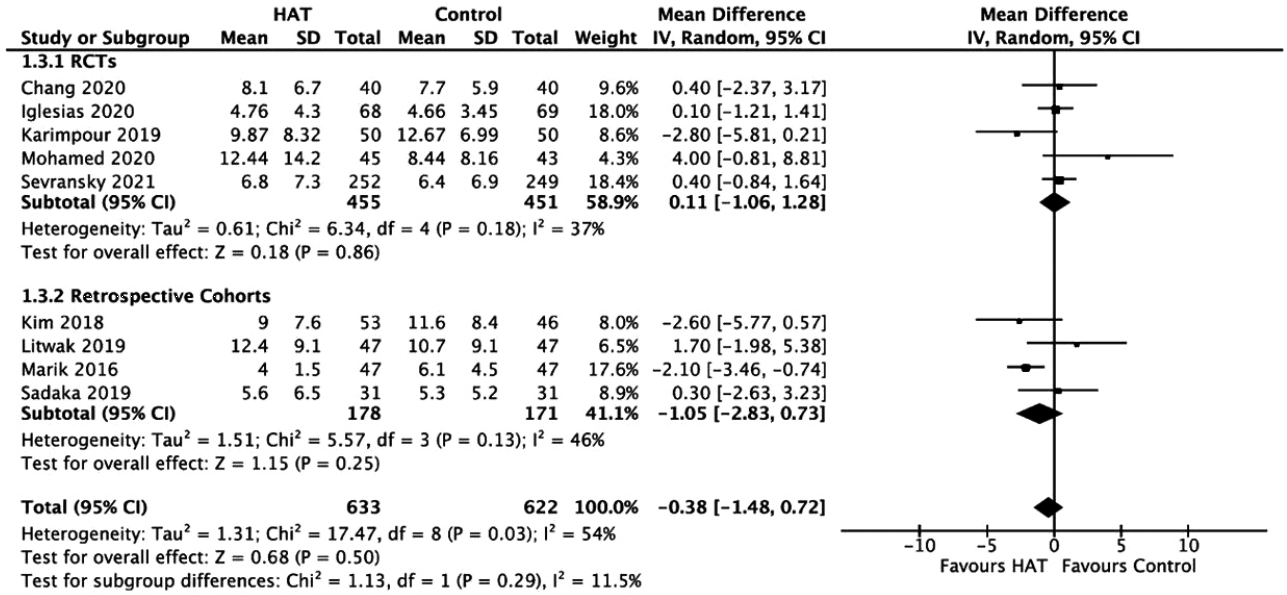
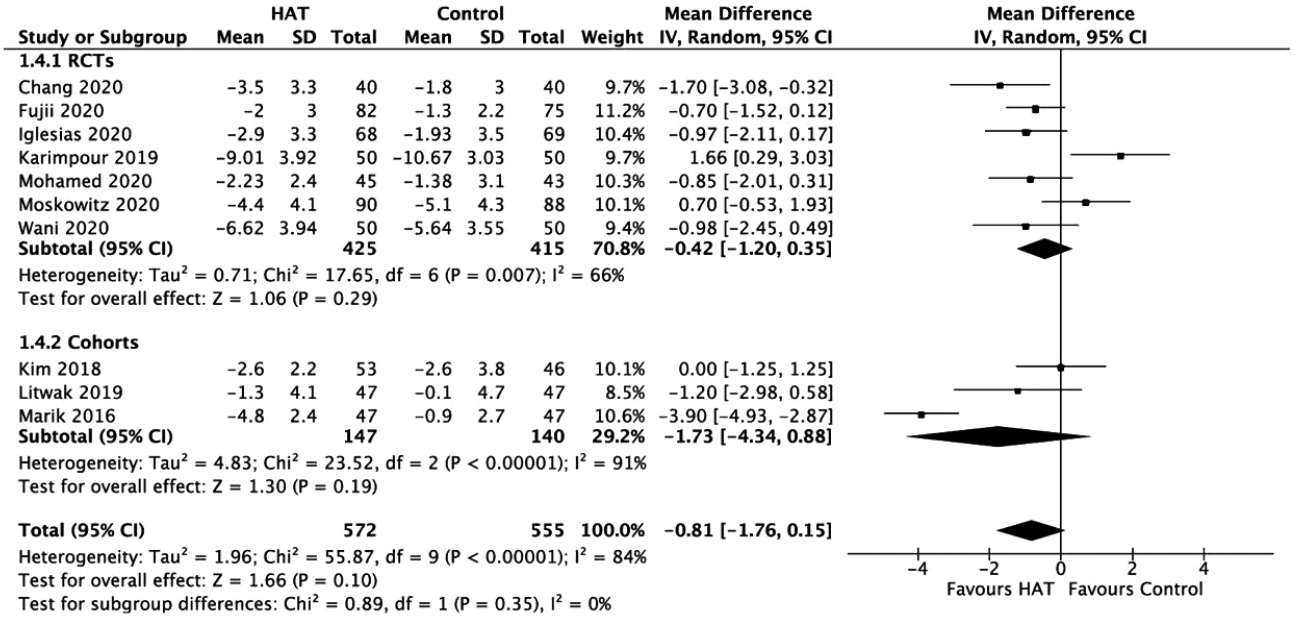
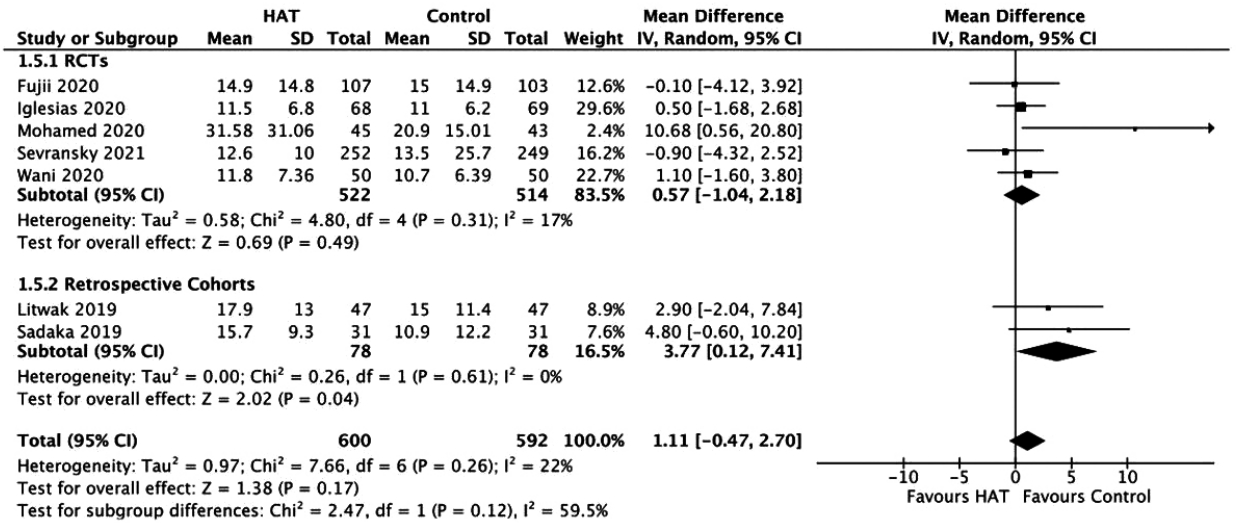
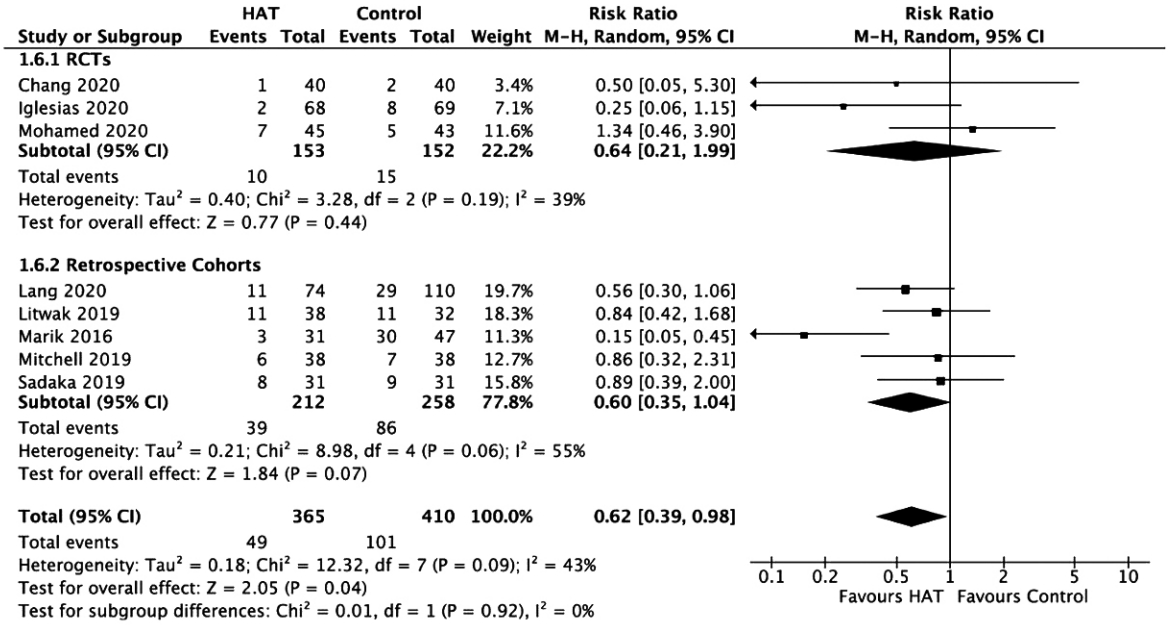
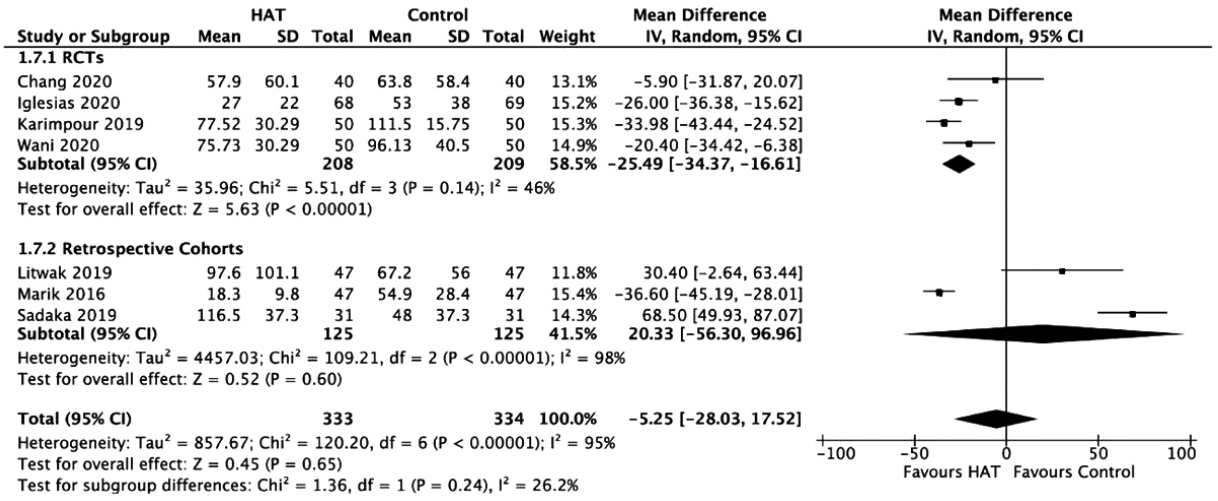
- Previous studies have suggested favorable outcomes of hydrocortisone, ascorbic acid (vitamin C), and thiamine (HAT) therapy in patients with sepsis. However, similar results have not been duplicated in sequential studies. This meta-analysis aimed to reevaluate the value of HAT treatment in patients with sepsis. Electronic databases were searched up until October 2020 for any studies that compared the effect of HAT versus non-HAT use in patients with sepsis. Data from 15 studies (eight randomized controlled trials [RCTs] and seven cohort studies) involving 67,349 patients were included. The results from the RCTs show no significant benefit of triple therapy on hospital mortality (risk ratio [RR], 0.99; P=0.92; I2=0%); intensive care unit (ICU) mortality (RR, 0.77; P=0.20; I2=58%); ICU length of stay (weighted mean difference [WMD], 0.11; P=0.86; I2 =37%) or hospital length of stay (WMD: 0.57; P=0.49; I2=17%), and renal replacement therapy (RR, 0.64; P=0.44; I2=39%). The delta Sequential Organ Failure Assessment (SOFA) score favored treatment after a sensitivity analysis (WMD, –0.72; P=0.01; I2=32%). However, a significant effect was noted for the duration of vasopressor use (WMD, –25.49; P<0.001; I2=46%). The results from cohort studies have also shown no significant benefit of HAT therapy on hospital mortality, ICU mortality, ICU length of stay, length of hospital stay, the delta SOFA score, the use of renal replacement therapy, or vasopressor duration. HAT therapy significantly reduced the duration of vasopressor use and improved the SOFA score but appeared not to have significant benefits in other outcomes for patients with sepsis. Further RCTs can help understand its benefit exclusively.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
KEY MESSAGES
-
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: MKRS, MKLP, MAK, AH, NH, MKC, SP. Data curation: MKRS, MKLP, MAK, AH, NH, MKC, SP, MSJ, SL, VS, JK, BE, EB. Formal analysis: MKRS, MKLP, MAK, AH, NH, MKC, SP. Methodology: MAK, MKRS, AH, NH, MKC, SP. Project administration: MKRS, MKLP, MSJ, OJI. Visualization: MKRS, MSJ, SL, VS, JK, BE, EB. Writing–original draft: MKRS, MKLP, MAK, AH, NH, MKC, SP, MSJ, SL, VS, JK, BE, EB. Writing–review & editing: all authors.
NOTES
SUPPLEMENTARY MATERIALS
Supplementary Figure 1.
Supplementary Figure 2.



| Study | Country | Study design | Total sample |
Sample |
Age (yr) |
Male |
Control group treatment | Intervention and dosage/route | Outcome in the intervention group | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention group | Control group | Intervention group | Control group | Intervention group | Control group | |||||||
| Sadaka (2019) [38] | USA | Retrospective | 62 | 31 | 31 | 67±16 | 70±12 | 16 (52) | 16 (52) | Managed according to current sepsis guidelines | Ascorbic acid 1.5 g IV every 6 hours for 4 days; hydrocortisone 50 mg IV every 6 hours for 7 days; thiamine 200 mg IV every 12 hours for 4 days IV | ICU mortality, 3 (9.6) |
| Hospital mortality, 9 (29) | ||||||||||||
| Hospital LOS, 15 days (10–22) | ||||||||||||
| RRT for AKI, 8 (26) | ||||||||||||
| Duration of VP, 4.5 days (4–6) | ||||||||||||
| MV-free day, 10.2 (5–15) | ||||||||||||
| Marik (2016) [39] | USA | Retrospective | 94 | 27 | 47 | 58.3±14.1 | 62.2±14.3 | 27 (100) | 23 (49) | Broad spectrum antibiotics, fluids, vasopressors, enteral nutrition, thrombosis prophylaxis, allow permissive hyperglycemia | Ascorbic acid 1.5 g IV every 6 hours for 4 days or until ICU discharge; hydrocortisone 50 mg IV every 6 hours for 7 days or until ICU discharge; thiamine 200 mg IV every 12 hours for 4 days or until ICU discharge | Hospital mortality, 4 (8.5) |
| ICU LOS, 4 days (3–5) | ||||||||||||
| Duration of VP, 18.3±9.8 hours | ||||||||||||
| RRT for AKI, 3/31 (10) | ||||||||||||
| Procalcitonin clearance (72 hours), 86.4% (80.1%–90.8%) | ||||||||||||
| Mitchell (2019) [40] | USA | Retrospective | 76 | 38 | 38 | 68±10 | 68±10 | 36 (95) | 37 (97) | IV hydrocortisone alone | Ascorbic acid 1.5 g IV every 6 hours for 4 days; hydrocortisone 50 mg IV every 6 hours or 100 mg IV every 8 hours or continuous IV infusion of 10 mg per hour for 7 days then tapered over approximately 3–5 days; thiamine 200 mg IV every 12 hours for 4 days | Hospital mortality, 18 (47) |
| ICU mortality, 12 (32) | ||||||||||||
| 28-Day mortality, 22 (58) | ||||||||||||
| 60-Day mortality, 22 (58) | ||||||||||||
| Litwak (2019) [41] | USA | Retrospective | 94 | 47 | 47 | 58.3±17 | 60.1±14 | 28 (59.6) | 29 (61.7) | Fluid resuscitation with 30 mL/kg of crystalloid, broad spectrum antibiotics, vasopressor therapy | At least one dosage of each of the following medications; ascorbic acid 1.5 g IV every 6 hours; hydrocortisone 50 mg IV every 6 hours or 100 mg IV every 8 hours; thiamine 200 mg IV every 12 hours | Hospital mortality, 19 (40.4) |
| ICU mortality, 17 (36.2) | ||||||||||||
| RRT for AKI, 11/38 (28.9) | ||||||||||||
| ICU LOS, 11.0 days (7.0–19.0) | ||||||||||||
| Hospital LOS, 19.0 days (9.0–26.) | ||||||||||||
| Duration of VP, 84.2 hours (37.0–169.3) | ||||||||||||
| Delta procalcitonin (72 hours), 0.1 ng/mL (–55.0 to 9.1) | ||||||||||||
| Fujii (2020) [42] | Australia, New Zealand and Brazil | RCT | 211a | 107 | 104 | 61.9±15.9 | 61.6±13.9 | 68 (63.6) | 65 (62.5) | IV hydrocortisone 50 mg every 6 hours and thiamine 200 mg every 12 hours | Ascorbic acid 1.5 g IV every 6 hours; hydrocortisone 50 mg IV every 6 hours; thiamine 200 mg every 12 hours | 28-Day mortality, 24/106 (22.6) |
| 90-Day mortality, 30/105 (28.6) | ||||||||||||
| ICU mortality, 21 (19.6) | ||||||||||||
| Hospital mortality, 25 (23.4) | ||||||||||||
| 28-Day cumulative vasopressorfree days, 25.6 (17.8–26.8) | ||||||||||||
| 28-Day cumulative mechanical ventilation-free days, 25.3 (5.2–28.0) | ||||||||||||
| 28-Day RRT–free days, 28.0 (23.5–28.0) | ||||||||||||
| 28-Day ICU-free days, 21.9 (0–25.8) | ||||||||||||
| Hospital LOS, 12.3 days (6.2–26.0) | ||||||||||||
| Karimpour (2019) [43] | Iran | RCT | 100 | 50 | 50 | 56.2±13.6 | 61.1±16.9 | 23 (46) | 20 (40) | Normal saline, norepinephrine, hydrocortisone | Ascorbic acid 50 mg/kg IV every 6 hours up to 6 g/day for 4 days; all included patients received hydrocortisone 200 mg daily for 4 days then tapers over 4 days; thiamine 200 mg IV | Delta SOFA score, 9.01±3.92 |
| 28-Day mortality, 8 (15) | ||||||||||||
| Duration of vasopressors, 77.52±21.5 hours | ||||||||||||
| ICU LOS, 9.87±8.32 | ||||||||||||
| Mechanical ventilation, 6.67±7.84 days | ||||||||||||
| Procalcitonin level, 1.25±1.61 ng/mL | ||||||||||||
| Wani (2020) [44] | India | RCT | 100 | 50 | 50 | 51.5±35.6 | 50.7±35.5 | 31 (62) | 28 (56) | Broad spectrum antibiotics, intravenous fluids, vasopressors, and mechanical ventilation as indicated | Ascorbic acid 1.5 g IV every 6 hours for 4 days or until hospital discharge; hydrocortisone 50 mg IV every 6 hours for 7 days or until ICU discharge then tapered over 3 days; thiamine 200 mg IV every 12 hours for 4 days or until hospital discharge | Hospital mortality, 24% |
| Duration of vasopressor use, 75.72±30.29 | ||||||||||||
| Hospital LOS, 11.82±7.36 days | ||||||||||||
| 30-Day mortality, 20 (40) | ||||||||||||
| Kim (2018) [45] | Korea | Retrospective | 99 | 53 | 46 | 73 (62–79) | 74 (68–79) | 41 (77) | 29 (63) | Managed according to therapeutic recommendations in Surviving Sepsis Campaign Guidelines and lungprotective ventilation strategy | Ascorbic acid 6 g IV divided into 4 equal doses; hydrocortisone 50 mg IV every 6 hours for 7 days then tapered over 3 days; thiamine 200 mg IV every 12 hours for 4 days | Hospital mortality, 6 (17) |
| ICU LOS, 9 days (5–14) | ||||||||||||
| No. ventilator-free days at day 28, 12.3±11.0 | ||||||||||||
| No. vasopressor-free days at day 28, 19.8±10.8 | ||||||||||||
| Iglesias (2020) [46] | USA | RCT | 137 | 68 | 69 | 70±12 | 67±14 | 32 (47) | 27 (39) | Saline placebo | Ascorbic acid 1.5 g every 6 hours; hydrocortisone 50 mg every 6 hours; thiamine 200 mg every 12 hours | Delta SOFA score at 72 hours, 2.9±3.3 |
| Duration of vasopressors, 27±22 hours | ||||||||||||
| Hospital mortality, 11 (16) | ||||||||||||
| ICU mortality, 6 (9) | ||||||||||||
| Hospital LOS, 11.5±6.8 days | ||||||||||||
| ICU LOS, 4.76±4.3 days | ||||||||||||
| Procalcitonin clearance, 63 (170) | ||||||||||||
| Ventilator-free days, 22 (6.2) | ||||||||||||
| AKI, 54 (79) | ||||||||||||
| Moskowitz (2020) [47] | USA | RCT | 200 | 101 | 99 | 68.9±15 | 67.6±13.9 | 57 (56.4) | 54 (54.6) | Local sepsis guidelines including antibiotics, volume resuscitation and vasopressors | Ascorbic acid 1.5 g every 6 hours for 4 days or until ICU discharge; hydrocortisone 50 mg every 6 hours for 4 days or until ICU discharge; thiamine 100 mg every 6 hours for 4 days or until ICU discharge | All-cause mortality over 30 days, 35 (34.7) |
| Kidney failure, 32 (31.7) | ||||||||||||
| Ventilator-free days, 6 (2–7) | ||||||||||||
| Shock-free days, 5 (3–5) | ||||||||||||
| Incidence of delirium, 31/83 (37.4) | ||||||||||||
| ICU-free days, 22 (3–25) | ||||||||||||
| All-cause mortality to ICU discharge, 23 (22.7) | ||||||||||||
| All-cause mortality to hospital discharge, 28 (277) | ||||||||||||
| Survivors discharged home, 34/73 (46.6) | ||||||||||||
| Vail (2020) [48] | USA | Retrospective | 65,299 | 1,548 | 63,751 | 64.6±14.8 | 66.1±14.7 | 1,903 (53.2) | 168,833 (51.3) | Not mentioned | At least one charge for high-dose IV ascorbic acid along with at least one charge for both IV hydrocortisone and IV thiamine at any dose | Mortality for hospital, 437 (28.2) |
| Mohamed (2020) [49] | India | RCT | 85 | 45 | 43 | 58.7±14.9 | 59.4±15 | 31 (69) | 32 (74) | Standard of care for septic shock with hydrocortisone and vitamin supplements according to the treating physician’s discretion | Ascorbic acid 1.5 g IV every 6 hours for 4 days; hydrocortisone 50 mg IV every 6 hours for 4 days; thiamine 200 mg IV every 12 hours for 4 days | Mortality, 23/43 (53) |
| Time to shock reversal, 34.58±22.63 hours | ||||||||||||
| Hospital LOS, 20.9±15.01 days | ||||||||||||
| Long (2020) [50] | USA | Retrospective | 206 | 79 | 127 | 64.4±13.9 | 61.1±16.2 | 43 (54.4) | 70 (55.9) | 2012 Sepsis Guidelines including 30 mL/kg of crystalloid, broad spectrum antibiotics, and vasopressor therapy; steroids at the discretion of the physician | Ascorbic acid 1.5 g IV every 6 hours; hydrocortisone 50 mg IV every 6 hours; thiamine 200 mg IV every 12 hours | Hospital mortality, 21 (26.6) |
| ICU mortality, 9 (11.4) | ||||||||||||
| Vasopressor duration (median), 13.9 hours | ||||||||||||
| RRT initiation, 11/74 (14.9) | ||||||||||||
| Ventilator duration, 3.4 days | ||||||||||||
| ICU LOS (median), 2.0 days | ||||||||||||
| Hospital LOS (median), 9.5 days | ||||||||||||
| Chang (2020) [51] | China | RCT | 80 | 40 | 40 | 59.5±15 | 63.7±12.8 | 22 (57.5) | 21 (52.5) | 2016 International management of sepsis guidelines including resuscitation, antimicrobial therapy, vasopressor strategy, mechanical ventilation, and RRT | Ascorbic acid 1.5 g IV every 6 hours for 4 days or until ICU discharge; hydrocortisone 50 mg every 6 hours for 7 days or until ICU discharge; thiamine 200 mg IV every 12 hours for 4 days or until ICU discharge | 28-Day mortality, 11 (27.5) |
| ICU LOS, 7.5 days (4–12.8) | ||||||||||||
| Duration of vasopressors, 46 hours (23.8–102.5) | ||||||||||||
| New AKI, 1 (2.5) | ||||||||||||
| Delta SOFA score (72 hours), 3.5±3.3 | ||||||||||||
| Procalcitonin clearance (72 hours), 75.8 (62.2–86.4) | ||||||||||||
| Duration of mechanical ventilation, 126.5 hours (63.5–239.3) | ||||||||||||
| Lactate clearance (72 hours), 21.3% (–49.7% to 44.2%) | ||||||||||||
| Sevransky (2021) [52] | USA | RCT | 501 | 252 | 249 | 60.6±13.4 | 61±16.4 | 139 (55.2) | 134 (53.8) | Matching placebo | Ascorbic acid 1.5 g, thiamine 100 mg, hydrocortisone 50 mg every 6 hours; patients can be given corticosteroids. | Ventilator- and vasopressor-free days, 25 (0–29) |
| Mortality at 30 days, 56 (22.2) | ||||||||||||
| ICU mortality, 52 (20.6) | ||||||||||||
| Mortality at 180 days, 102 (40.5) | ||||||||||||
| Length of ICU stay, 6.7 (7.3) | ||||||||||||
| Length of hospital stay, 12.6 (10) | ||||||||||||
Values are presented as mean±standard deviation, number (%), or median (interquartile range) unless otherwise indicated.
IV: intravenous; ICU: intensive care unit; LOS: length of stay; RRT: renal replacement therapy; AKI: acute kidney injury; VP: vasopressors; MV: mechanical ventilation; RCT: randomized controlled trial; SOFA: Sequential Organ Failure Assessment.
a Five patients (2.3%; 2 in the intervention group and 3 in the control group) either withdrew or refused consent to continue participation and withdrew all data, leaving 211 patients.
- 1. Abraham E. New definitions for sepsis and septic shock: continuing evolution but with much still to be done. JAMA 2016;315:757-9.ArticlePubMed
- 2. Angus DC, van der Poll T. Severe sepsis and septic shock. N Engl J Med 2013;369:840-51.ArticlePubMed
- 3. Beesley SJ, Lanspa MJ. Why we need a new definition of sepsis. Ann Transl Med 2015;3:296. PubMedPMC
- 4. Allegranzi B, Bagheri Nejad S, Chraiti MN, Castillejos GG, Kilpatrick C, Kelley E. Report on the burden of endemic health care-associated infection worldwide. Geneva, World Health Organization. 2011.
- 5. Rudd KE, Johnson SC, Agesa KM, Shackelford KA, Tsoi D, Kievlan DR, et al. Global, regional, and national sepsis incidence and mortality, 1990-2017: analysis for the Global Burden of Disease Study. Lancet 2020;395:200-11.ArticlePubMedPMC
- 6. Marik PE, Farkas JD. The changing paradigm of sepsis: early diagnosis, early antibiotics, early pressors, and early adjuvant treatment. Crit Care Med 2018;46:1690-2.ArticlePubMed
- 7. Galley HF, Howdle PD, Walker BE, Webster NR. The effects of intravenous antioxidants in patients with septic shock. Free Radic Biol Med 1997;23:768-74.ArticlePubMed
- 8. Wilson JX. Mechanism of action of vitamin C in sepsis: ascorbate modulates redox signaling in endothelium. Biofactors 2009;35:5-13.ArticlePubMedPMC
- 9. Kuhn SO, Meissner K, Mayes LM, Bartels K. Vitamin C in sepsis. Curr Opin Anaesthesiol 2018;31:55-60.ArticlePubMedPMC
- 10. Mandl J, Szarka A, Bánhegyi G. Vitamin C: update on physiology and pharmacology. Br J Pharmacol 2009;157:1097-110.ArticlePubMedPMC
- 11. Heo HJ, Lee CY. Protective effects of quercetin and vitamin C against oxidative stress-induced neurodegeneration. J Agric Food Chem 2004;52:7514-7.ArticlePubMed
- 12. May JM, Harrison FE. Role of vitamin C in the function of the vascular endothelium. Antioxid Redox Signal 2013;19:2068-83.ArticlePubMedPMC
- 13. Zhou G, Kamenos G, Pendem S, Wilson JX, Wu F. Ascorbate protects against vascular leakage in cecal ligation and puncture-induced septic peritonitis. Am J Physiol Regul Integr Comp Physiol 2012;302:R409-16.ArticlePubMed
- 14. Costa NA, Azevedo PS, Polegato BF, Zornoff LA, Paiva SA, Minicucci MF. Thiamine as a metabolic resuscitator in septic shock: one size does not fit all. J Thorac Dis 2016;8:E471-2.ArticlePubMedPMC
- 15. Moskowitz A, Donnino MW. Thiamine (vitamin B1) in septic shock: a targeted therapy. J Thorac Dis 2020;12(Suppl 1):S78-83.ArticlePubMedPMC
- 16. Donnino MW, Andersen LW, Chase M, Berg KM, Tidswell M, Giberson T, et al. Randomized, double-blind, placebo-controlled trial of thiamine as a metabolic resuscitator in septic shock: a pilot study. Crit Care Med 2016;44:360-7.PubMedPMC
- 17. Costa NA, Gut AL, de Souza Dorna M, Pimentel JA, Cozzolino SM, Azevedo PS, et al. Serum thiamine concentration and oxidative stress as predictors of mortality in patients with septic shock. J Crit Care 2014;29:249-52.ArticlePubMed
- 18. Woolum JA, Abner EL, Kelly A, Thompson Bastin ML, Morris PE, Flannery AH. Effect of thiamine administration on lactate clearance and mortality in patients with septic shock. Crit Care Med 2018;46:1747-52.ArticlePubMed
- 19. Artigas A, Carlet J, Garnacho J, Niederman M, Torres A. 24th international symposium on infections in the critically ill patient. Med Sci 2019;7:23. Article
- 20. Erstad BL, Brophy GM, Martin SJ, Haas CE, Devlin JW, Welage LS, et al. Key articles and guidelines relative to intensive care unit pharmacotherapy: 2009 update. Pharmacotherapy 2009;29:1228-69.ArticlePubMed
- 21. Annane D. The role of ACTH and corticosteroids for sepsis and septic shock: an update. Front Endocrinol (Lausanne) 2016;7:70. ArticlePubMedPMC
- 22. Schumer W. Steroids in the treatment of clinical septic shock. Ann Surg 1976;184:333-41.ArticlePubMedPMC
- 23. Keh D, Trips E, Marx G, Wirtz SP, Abduljawwad E, Bercker S, et al. Effect of hydrocortisone on development of shock among patients with severe sepsis: the HYPRESS randomized clinical trial. JAMA 2016;316:1775-85.ArticlePubMed
- 24. Marik PE, Pastores SM, Annane D, Meduri GU, Sprung CL, Arlt W, et al. Recommendations for the diagnosis and management of corticosteroid insufficiency in critically ill adult patients: consensus statements from an international task force by the American College of Critical Care Medicine. Crit Care Med 2008;36:1937-49.ArticlePubMed
- 25. Annane D, Sébille V, Charpentier C, Bollaert PE, François B, Korach JM, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA 2002;288:862-71.ArticlePubMed
- 26. Sprung CL, Annane D, Keh D, Moreno R, Singer M, Freivogel K, et al. Hydrocortisone therapy for patients with septic shock. N Engl J Med 2008;358:111-24.ArticlePubMed
- 27. Keh D, Boehnke T, Weber-Cartens S, Schulz C, Ahlers O, Bercker S, et al. Immunologic and hemodynamic effects of “lowdose” hydrocortisone in septic shock: a double-blind, randomized, placebo-controlled, crossover study. Am J Respir Crit Care Med 2003;167:512-20.ArticlePubMed
- 28. Moskowitz A, Andersen LW, Huang DT, Berg KM, Grossestreuer AV, Marik PE, et al. Ascorbic acid, corticosteroids, and thiamine in sepsis: a review of the biologic rationale and the present state of clinical evaluation. Crit Care 2018;22:283. ArticlePubMedPMC
- 29. Marik PE. Hydrocortisone, ascorbic acid and thiamine (HAT therapy) for the treatment of sepsis: focus on ascorbic acid. Nutrients 2018;10:1762. ArticlePubMedPMC
- 30. Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016;315:801-10.ArticlePubMedPMC
- 31. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 2010;25:603-5.ArticlePubMed
- 32. Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa, Ottawa Hospital Research Institute. 2000.
- 33. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or midquartile range. Stat Methods Med Res 2018;27:1785-805.ArticlePubMed
- 34. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 2014;14:135. ArticlePubMedPMC
- 35. Patsopoulos NA, Evangelou E, Ioannidis JP. Sensitivity of between-study heterogeneity in meta-analysis: proposed metrics and empirical evaluation. Int J Epidemiol 2008;37:1148-57.ArticlePubMedPMC
- 36. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177-88.ArticlePubMed
- 37. Mathes T, Kuss O. A comparison of methods for meta-analysis of a small number of studies with binary outcomes. Res Synth Methods 2018;9:366-81.ArticlePubMed
- 38. Sadaka F, Grady J, Organti N, Donepudi B, Korobey M, Tannehill D, et al. Ascorbic acid, thiamine, and steroids in septic shock: propensity matched analysis. J Intensive Care Med 2020;35:1302-6.ArticlePubMed
- 39. Marik PE, Khangoora V, Rivera R, Hooper MH, Catravas J. Hydrocortisone, vitamin C, and thiamine for the treatment of severe sepsis and septic shock: a retrospective before-after study. Chest 2017;151:1229-38.ArticlePubMed
- 40. Mitchell AB, Ryan TE, Gillion AR, Wells LD, Muthiah MP. Vitamin C and thiamine for sepsis and septic shock. Am J Med 2020;133:635-8.ArticlePubMed
- 41. Litwak JJ, Cho N, Nguyen HB, Moussavi K, Bushell T. Vitamin C, hydrocortisone, and thiamine for the treatment of severe sepsis and septic shock: a retrospective analysis of real-world application. J Clin Med 2019;8:478. ArticlePubMedPMC
- 42. Fujii T, Luethi N, Young PJ, Frei DR, Eastwood GM, French CJ, et al. Effect of vitamin C, hydrocortisone, and thiamine vs hydrocortisone alone on time alive and free of vasopressor support among patients with septic shock: the VITAMINS randomized clinical trial. JAMA 2020;323:423-31.PubMedPMC
- 43. Karimpour H, Bahrami A, Amini S, Rezaei M, Amini-Saman J, Shahbazi F. Effects of a high dose of vitamin C along with thiamine in critically-ill patients with septic shock: a preliminary study. J Pharm Res Int 2019;29:1-7.ArticlePDF
- 44. Wani SJ, Mufti SA, Jan RA, Shah SU, Qadri SM, Khan UH, et al. Combination of vitamin C, thiamine and hydrocortisone added to standard treatment in the management of sepsis: results from an open label randomized controlled clinical trial and a review of the literature. Infect Dis (Lond) 2020;52:271-8.PubMed
- 45. Kim WY, Jo EJ, Eom JS, Mok J, Kim MH, Kim KU, et al. Combined vitamin C, hydrocortisone, and thiamine therapy for patients with severe pneumonia who were admitted to the intensive care unit: propensity score-based analysis of a before-after cohort study. J Crit Care 2018;47:211-18.ArticlePubMed
- 46. Iglesias J, Vassallo AV, Patel VV, Sullivan JB, Cavanaugh J, Elbaga Y. Outcomes of metabolic resuscitation using ascorbic acid, thiamine, and glucocorticoids in the early treatment of sepsis: the ORANGES trial. Chest 2020;158:164-73.ArticlePubMed
- 47. Moskowitz A, Huang DT, Hou PC, Gong J, Doshi PB, Grossestreuer AV, et al. Effect of ascorbic acid, corticosteroids, and thiamine on organ injury in septic shock: the ACTS randomized clinical trial. JAMA 2020;324:642-50.ArticlePubMedPMC
- 48. Vail EA, Wunsch H, Pinto R, Bosch NA, Walkey AJ, Lindenauer PK, et al. Use of hydrocortisone, ascorbic acid, and thiamine in adults with septic shock. Am J Respir Crit Care Med 2020;202:1531-9.ArticlePubMed
- 49. Mohamed ZU, Prasannan P, Moni M, Edathadathil F, Prasanna P, Menon A, et al. Vitamin C therapy for routine care in septic shock (ViCTOR) trial: effect of intravenous vitamin C, thiamine, and hydrocortisone administration on inpatient mortality among patients with septic shock. Indian J Crit Care Med 2020;24:653-61.ArticlePubMedPMC
- 50. Long MT, Frommelt MA, Ries MP, Murray M, Osman F, Krause BM, et al. Early hydrocortisone, ascorbate and thiamine therapy for severe septic shock. Crit Care Shock 2020;23:23-34.
- 51. Chang P, Liao Y, Guan J, Guo Y, Zhao M, Hu J, et al. Combined treatment with hydrocortisone, vitamin C, and thiamine for sepsis and septic shock: a randomized controlled trial. Chest 2020;158:174-82.ArticlePubMed
- 52. Sevransky JE, Rothman RE, Hager DN, Bernard GR, Brown SM, Buchman TG, et al. Effect of vitamin C, thiamine, and hydrocortisone on ventilator- and vasopressor-free days in patients with sepsis: the VICTAS randomized clinical trial. JAMA 2021;325:742-50.ArticlePubMedPMC
- 53. Barabutis N, Khangoora V, Marik PE, Catravas JD. Hydrocortisone and ascorbic acid synergistically prevent and repair lipopolysaccharide-induced pulmonary endothelial barrier dysfunction. Chest 2017;152:954-62.ArticlePubMedPMC
- 54. Berger MM. Do micronutrient deficiencies contribute to mitochondrial failure in critical illness? Curr Opin Clin Nutr Metab Care 2020;23:102-10.ArticlePubMed
- 55. Hwang SY, Ryoo SM, Park JE, Jo YH, Jang DH, Suh GJ, et al. Combination therapy of vitamin C and thiamine for septic shock: a multi-centre, double-blinded randomized, controlled study. Intensive Care Med 2020;46:2015-25.ArticlePubMedPMC
- 56. Shi R, Tie H. Benefit of hydrocortisone, thiamine, and vitamin C for patients with sepsis or septic shock? Too early to draw conclusions. Crit Care 2020;24:431. ArticlePubMedPMC
- 57. Rowe TA, McKoy JM. Sepsis in older adults. Infect Dis Clin North Am 2017;31:731-42.ArticlePubMed
- 58. Kim J, Arnaout L, Remick D. Hydrocortisone, ascorbic acid, and thiamine (HAT) therapy decreases oxidative stress, improves cardiovascular function, and improves survival in murine sepsis. Shock 2020;53:460-7.ArticlePubMed
- 59. Petsakul S, Morakul S, Tangsujaritvijit V, Kunawut P, Singhatas P, Sanguanwit P. Effects of thiamine on vasopressor requirements in patients with septic shock: a prospective randomized controlled trial. BMC Anesthesiol 2020;20:280. ArticlePubMedPMC
- 60. Martin GS, Mannino DM, Moss M. The effect of age on the development and outcome of adult sepsis. Crit Care Med 2006;34:15-21.ArticlePubMed
- 61. Starr ME, Saito H. Sepsis in old age: review of human and animal studies. Aging Dis 2014;5:126-36.ArticlePubMedPMC
References
Figure & Data
References
Citations
- Effect of intravenous vitamin C on adult septic patients: a systematic review and meta-analysis
Huoyan Liang, Qingqing Mu, Wenju Sun, Liming Liu, Simin Qiu, Zili Xu, Yuqing Cui, Yan Yan, Tongwen Sun
Frontiers in Nutrition.2023;[Epub] CrossRef - Insights Into Thiamine Supplementation in Patients With Septic Shock
Nara Aline Costa, Amanda Gomes Pereira, Clara Sandra Araujo Sugizaki, Nayane Maria Vieira, Leonardo Rufino Garcia, Sérgio Alberto Rupp de Paiva, Leonardo Antonio Mamede Zornoff, Paula Schmidt Azevedo, Bertha Furlan Polegato, Marcos Ferreira Minicucci
Frontiers in Medicine.2022;[Epub] CrossRef - Vitamin C-induced Hemolysis: Meta-summary and Review of Literature
Deven Juneja, Ravi Jain
Indian Journal of Critical Care Medicine.2022; 26(2): 224. CrossRef - Is it time to reconsider the administration of thiamine alone or in combination with vitamin C in critically ill patients? A meta-analysis of clinical trial studies
Nafiseh Shokri-mashhadi, Ali Aliyari, Zahra Hajhashemy, Saeed Saadat, Mohammad Hossein Rouhani
Journal of Intensive Care.2022;[Epub] CrossRef - Parenteral Vitamin C in Patients with Severe Infection: A Systematic Review
Arnav Agarwal, John Basmaji, Shannon M. Fernando, Fang Zhou Ge, Yingqi Xiao, Haseeb Faisal, Kimia Honarmand, Mathieu Hylands, Vincent Lau, Kimberley Lewis, Rachel Couban, François Lamontagne, Neill K. J. Adhikari
NEJM Evidence.2022;[Epub] CrossRef - Unanswered questions on the use of hydrocortisone, ascorbic acid, and thiamine therapy in sepsis and septic shock
David Ragoonanan, Nicolas Tran, Veeshal Modi, Paige Morgan Nickelsen
American Journal of Health-System Pharmacy.2022; 79(19): 1626. CrossRef - Impacts of Corticosteroid Therapy at Acute Stage of Hospital-Onset Clostridioides difficile Infections
Ching-Chi Lee, Jen-Chieh Lee, Chun-Wei Chiu, Pei-Jane Tsai, Wen-Chien Ko, Yuan-Pin Hung
Infection and Drug Resistance.2022; Volume 15: 5387. CrossRef - The impact of vitamin C-containing treatment on the mortality of patients with sepsis: A systematic review and meta-analysis of randomized controlled trials
Ching-Yi Chen, Chien-Tung Chiu, Ho-Sheng Lee, Chih-Cheng Lai
Journal of Infection and Public Health.2022; 15(12): 1514. CrossRef - Role of high dose vitamin C in management of hospitalised COVID-19 patients: A minireview
Deven Juneja, Anish Gupta, Sahil Kataria, Omender Singh
World Journal of Virology.2022; 11(5): 300. CrossRef - Current role of high dose vitamin C in sepsis management: A concise review
Deven Juneja, Prashant Nasa, Ravi Jain
World Journal of Critical Care Medicine.2022; 11(6): 349. CrossRef - HYDROCORTISONE, ASCORBIC ACID, AND THIAMINE THERAPY DECREASE RENAL OXIDATIVE STRESS AND ACUTE KIDNEY INJURY IN MURINE SEPSIS
John Kim, Allan Stolarski, Qiuyang Zhang, Katherine Wee, Daniel Remick
Shock.2022; 58(5): 426. CrossRef - Early administration of Vitamin C in patients with sepsis or septic shock in emergency departments: A multicenter, double blinded, randomized controlled trial: The C-EASIE trial protocol
Stefanie Vandervelden, Lina Wauters, Jan Breuls, Steffen Fieuws, Philippe Vanhove, Ives Hubloue, Magali Bartiaux, Jacques Creteur, François Stifkens, Koen Monsieurs, Didier Desruelles, Elisa Panada
PLOS ONE.2021; 16(11): e0259699. CrossRef - Hydrocortisone, ascorbic acid, and thiamine (HAT) for sepsis and septic shock: a meta-analysis with sequential trial analysis
Weilan Na, Huili Shen, Yichu Li, Dong Qu
Journal of Intensive Care.2021;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-









- Related articles
-
- The efficacy of therapeutic hypothermia in patients with poor-grade aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis
- The impact of ketamine on outcomes in critically ill patients: a systematic review with meta-analysis and trial sequential analysis of randomized controlled trials
- Comparison of high-flow nasal oxygen therapy and noninvasive ventilation in COVID-19 patients: a systematic review and meta-analysis

