Abstract
-
Background
- Optic nerve sheath diameter (ONSD) is an emerging non-invasive, easily accessible, and possibly useful measurement for evaluating changes in intracranial pressure (ICP). The utilization of bedside ultrasonography (USG) to measure ONSD has garnered increased attention due to its portability, real-time capability, and lack of ionizing radiation. The primary aim of the study was to assess whether bedside USG-guided ONSD measurement can reliably predict increased ICP in traumatic brain injury (TBI) patients.
-
Methods
- A total of 95 patients admitted to the trauma intensive care unit was included in this cross sectional study. Patient brain computed tomography (CT) scans and Glasgow Coma Scale (GCS) scores were assessed at the time of admission. Bedside USG-guided binocular ONSD was measured and the mean ONSD was noted. Microsoft Excel was used for statistical analysis.
-
Results
- Patients with low GCS had higher mean ONSD values (6.4±1.0 mm). A highly significant association was found among the GCS, CT results, and ONSD measurements (P<0.001). Compared to CT scans, the bedside USG ONSD had 86.42% sensitivity and 64.29% specificity for detecting elevated ICP. The positive predictive value of ONSD to identify elevated ICP was 93.33%, and its negative predictive value was 45.00%. ONSD measurement accuracy was 83.16%.
-
Conclusions
- Increased ICP can be accurately predicted by bedside USG measurement of ONSD and can be a valuable adjunctive tool in the management of TBI patients.
-
Keywords: intracranial pressure monitoring; optic nerve sheath diameter; traumatic brain injury
INTRODUCTION
Traumatic brain injury (TBI) is a formidable global health concern, contributing significantly to mortality, morbidity, and long-term disability rates. The ability to assess intracranial pressure (ICP) swiftly and accurately in TBI patients is pivotal in guiding timely interventions to prevent secondary brain injury and to optimize patient outcomes. In this context, measurement of the optic nerve sheath diameter (ONSD) is an emerging non-invasive, easily accessible, and possibly useful measurement for evaluating changes in ICP. The utilization of bedside ultrasonography (USG) to measure ONSD has garnered increased attention due to its portability, real-time capability, and absence of ionizing radiation [1-7].
The optic nerve, extending from the retina to the optic chiasma, is encompassed by cerebrospinal fluid within the subarachnoid space. The optic nerve sheath becomes distended as a result of increased ICP, a defining feature of TBI, which increases the pressure conveyed to the subarachnoid region. This distension is reflected in an enlarged ONSD, indicating it as a potential indicator of ICP changes. Non-invasive imaging and measurement of the optic nerve sheath using high-frequency ultrasound probes are important components of bedside USG examination of ONSD. The simplicity, safety, and ability to perform repeated measurements render this technique particularly attractive for real-time monitoring of ICP trends.
In the present study, we aimed to assess the clinical utility, accuracy, and limitations of ONSD measurements as a surrogate marker for ICP changes. Also, we assessed the potential of ONSD measurements to serve as an early indicator of elevated ICP, facilitating prompt clinical decision-making and optimizing patient care strategies.
MATERIALS AND METHODS
Aims and Objectives
The primary aim of the study was to assess whether USG-guided ONSD can reliably predict increased ICP in TBI patients. The secondary objective was to assess the relationship between USG-guided ONSD with the Glasgow Coma Scale (GCS).
Study Design
This cross-sectional study included a total of 95 patients hospitalized in an intensive care unit (ICU). This study was approved by the Institutional Ethics Committee of B. J. Government Medical College and Sassoon General Hospital, Pune, India (BJGMC/IEC/Pharmac/ND-Dept. 0822108-108 dated 8-08-2022), and written informed consent was obtained from all patients for use and publication of data. The study was registered with the Clinical Trials Registry-India registry (CTRI trial no. CTRI/2022/08/044907 dated 25/08/2022).
Inclusion and Exclusion Criteria
Patients aged between the ages of 18 and 65 years with TBI admitted to the trauma ICU were included in the study. Patients with major eye injuries, glaucoma history, or optic nerve abnormalities were excluded from the study (Figure 1).
Sample Size Calculation
The sample size was calculated by assuming the mean ONSD in increased ICP patients as 5.6±0.3 mm, at a statistical power of 0.90 (alpha=0.05) [8], leading to an estimated sample size of 95 subjects.
Methodology
After Institutional Ethics Committee approval, 95 patients admitted with head injury to the trauma ICU were selected for study. Patients were evaluated, computed tomography (CT) brain scans were conducted immediately after presentation, and casualty was noted. GCS (Table 1) was assessed at the time of admission and daily. When the patient was admitted, an ultrasonic probe with a linear frequency range of 6–13 MHz was used to measure the ONSD. All examinations were conducted in the supine position. The upper eyelid was closed and covered with conductive ultrasonic gel without applying any pressure. The probe was positioned on the lateral and superior sides of the orbit in accordance with a specified procedure [9]. The optic nerve was perceived as an elongated, hypoechoic structure with definite boundaries posterior to the globe. Three millimeters beyond the retina, the transverse ONSD was measured and reported. According to earlier research, a binocular ONSD greater than 5.0 mm was regarded as elevated [1-7]. To reduce intraobserver variability, the investigator performed three ONSD measurements in both the left and right eyes, and the mean of these measurements was calculated. Age, sex, clinical diagnosis, GCS, hemodynamic parameters, mechanical breathing, and comorbidities were other noted factors. Data were analyzed to determine the associations between variables and ONSD. Duration of the study was three months from August 2022 to October 2022.
Statistical Analysis
Microsoft Excel (ver. MSO Professional Plus 2016) was used for analysis. When appropriate, data are expressed as the mean SD or as a count and percentage (%). To determine the significance of differences between groups, the unpaired Student t-test, chi-square test, or Fisher's exact test was used. Significant results were those with a two-sided P-value ≤0.05. For all statistical studies, IBM SPSS software (ver. 20, IBM Corp.) was utilized.
RESULTS
Ninety-five individuals admitted to the trauma ICU with TBI were assessed. The mean age distribution was 43±11 years (Table 2). The minimum and maximum ages were 22 and 65 years, respectively. The majority of patients (31 total) was between the ages of 40 and 50 years. Of the 95 patients, 65 (68%) were male and 30 (31%) were female. The mean ONSD in males was 6.2±1.1 mm and 6.1±1.2 mm in females. The differences in ONSD based on age and gender were not significant (Table 3). Increased ONSD was seen in 75 patients (79%). The mean ONSD in increased ONSD patients was 6.5±0.7 mm and was 4.6±0.2 mm in patients with normal ONSD. The maximum ONSD value was 8.4 mm, and the lowest ONSD was 4 mm.
All patients included in the study had TBI and were evaluated by CT scan. Many patients (n=88, 92%) had multiple brain injuries in the form of extradural hemorrhage, subdural hemorrhage, subarachnoid hemorrhage, hemorrhagic contusion, and/or skull bone fractures. Isolated extradural hemorrhage or subdural hemorrhage was seen in only seven patients (7%).
In the present study, patients with a low GCS (2–8) (n=82, 86%) had higher mean ONSD (6.4±1.0 mm), and patients with moderate GCS (9–12) (n=13,13%) had lower mean ONSD (4.7±0.4 mm). Table 3 shows a highly significant correlation between GCS and ONSD measurements (<0.001). In the present study, 83 patients (87%) were on ventilator support and 12 (12%) were on spontaneous ventilation during examination of ONSD. The difference was not significant (Table 3).
On radiological CT examination, 81 patients (85%) had increased ICP and 14 (14%) had normal ICP as assessed by radiologists. Of 81 patients, 70 (86%) had ONSD values of greater than 5.0 mm and 11 (13%) had ONSD values of less than 5.0 mm. Of 14 patients with normal ICP, five (35%) had ONSD values of greater than 5.0 mm and nine (64%) had ONSD values of less than 5.0 mm, showing statistical significance (P<0.001) (Table 3).
The area under the curve (AUC) for the mean ONSD was 0.754, indicating good discrimination between true and false positives. This receiver operating characteristic (ROC) curve exhibited a notable capacity to differentiate effectively between normal and elevated ICP (Table 4, Figure 2). Sensitivity of the bedside USG measurement ONSD to detect increase ICP was 86.42% and specificity was 64.29% compared with results from CT scans. The positive predictive value of ONSD measurement to detect increased ICP was 93.33% and the negative predictive value was 45.00%. Accuracy of ONSD measurement was calculated as 83.16%.
DISCUSSION
Recent years have witnessed a surge in research exploring the association between ONSD and ICP, with a focus on its potential role in predicting intracranial hypertension. Several studies have suggested a correlation between ONSD measurements and elevated ICP level, supporting the notion that changes in ONSD may reflect changes in ICP [10,11]. However, discrepancies and methodological variations across studies necessitate a critical analysis of the current evidence base. The association between ONSD and ICP in TBI patients is evaluated in the current study. The impact of factors of age, gender, GCS, and the accuracy of USG measurements on the reliability of ONSD as an ICP surrogate is also assessed. Additionally, we discuss the potential integration of ONSD measurements into existing clinical algorithms for TBI management.
In the present study, we found no significant correlation between age and gender, similar to other studies [8,12]. Other studies have shown that GCS has significant correlation with ONSD, where they found that low GCS significantly correlates with higher ONSD [8]. Similar results are seen in our study as patients with low GCS had a mean ONSD of 6.4±1.0 mm, and patients with moderate GCS had an ONSD of 4.7±0.4 mm. The low GCS of individuals with severe TBI, which are associated with elevated ICPs, can be used to explain this finding.
We selected CT as our reference standard for assessing the outcomes of ONSD since head CT scans are often utilized in clinical practice to identify elevated ICP. In the present study, CT scans showed increased ICP in 81 patients and increased ONSD in 70 patients. This shows that ONSD and CT scan findings had a significant correlation. Similar findings were seen in other studies [8].
Here, we observed that ONSD assessment with ultrasound has good sensitivity and specificity (86.42% and 64.29%, respectively), with a 93.33% positive predictive value to identify increased ICP at an accuracy of 83.16%. Compared to CT scans, Kaur et al. [8] found a correlation between ONSD and ICP using ONSD assessment to detect elevated ICP in neurological trauma patients, with a sensitivity and specificity of 93.2% and 91.1%, respectively. The ONSD test had an accuracy of 92% and a positive predictive value to detect elevated ICP of 89.1% and a negative predictive value of 94.4%. Other studies have found a range of sensitivity for ONSD from 88% to 100% with a specificity range between 63% to 95% [7,13,14]. These investigations further showed the strong correlation between an ONSD of 5.0 mm and an ICP greater than 20 mm Hg. [7,13].
Systematic reviews and meta-analyses of the literature have demonstrated that ONSD greater than 5.0 to 5.7 mm is associated with ICP greater than 20 mm Hg [4,15]. According to Rajajee et al. [16], the ideal ONSD for detection of ICP of 20 mm Hg was 0.48 cm, with a sensitivity and specificity of 96% and 94%, respectively. Kaur et al. [8] found an ONSD of 0.46 cm to have a sensitivity of 95% and an ONSD of 0.52 cm to have a specificity of 98% for the detection of increased ICP. Binocular ONSD >5.0 mm served as our reference standard, and ONSD >5.0 mm was considered abnormal. With an AUC value of 0.754, the ROC for the ONSD values demonstrated good separation between true and false positives.
Although invasive methods are thought to be the best for measuring ICP, they come with a high risk of infection and bleeding, are difficult to use, and are extremely expensive, especially affecting low- and middle-income countries [17]. Transporting critically ill ICU patients to radiology facilities is frequently challenging and may even be life-threatening. There have been reports of adverse event rates as high as 68% and fatality rates as high as 2% for critically ill patients who are transported between hospitals [18]. According to several studies, only around half of patient treatment plans are changed as a result of CT scans (39% to 68%) [19,20]. ONSD assessment as a bedside procedure is non-invasive, portable, quick, affordable, repeatable, effective, radiation-free, and does not require a lot of training [17,21]. In a clinical situation when there is uncertainty, ONSD enables quick triage and less invasive examination of intracranial hypertension. Additionally, it provides helpful details for planning definitive neurosurgical treatment and for managing intracranial hypertension early. ONSD responds to ICP instantly. The optic nerve sheath has very little risk of plastic deformation or over-distention within the effective range [22,23] and is a very helpful adjunct to other common diagnostic techniques [24]. Future work is needed to establish consistent techniques and a range of normal ONSD values [17].
High interobserver variability in assessments is a principal drawback of this method but can be minimized with practice and training. Only CT scans were used to assess ICP and no other invasive method was employed for comparison. Bedside USG measurement of the ONSD shows potential as a valuable additional tool in predicting increased ICP to aid in the treatment of patients with TBI. As ongoing research continues to refine our understanding of the relationship between ONSD and ICP, it is essential to establish standardized protocols and methodologies for ONSD measurement. Here, we offer a comprehensive synthesis of the existing evidence, highlighting both the potential and the challenges in utilizing ONSD as a surrogate marker for ICP in the context of TBI.
KEY MESSAGES
▪ Bedside ultrasonographic measurement of the optic nerve sheath diameter (ONSD) holds promise as an additional valuable tool for managing traumatic brain injury (TBI) patients.
▪ The establishment of standardized protocols and methodologies for ONSD measurement is crucial as ongoing research seeks to better understand the relationship between ONSD and intracranial pressure (ICP).
▪ This review provides a comprehensive analysis of existing evidence, emphasizing the potential benefits and challenges associated with using ONSD as a surrogate marker for ICP in the context of TBI, contributing to the ongoing discourse in this field.
NOTES
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: SJK, SVN. Methodology: SJK, AHP, SVN, AY, RMS. Software: SJK, SMS, AN, PD. Validation: Sall authors. Formal analysis: all authors. Investigation: all authors. Resources: SJK, AY, RMS, SMS, AN, PD. Data curation: SJK, SMS, AN, PD. Supervision: AHP, SVN. Writing–original draft: SJK, AHP, SVN, AY, RMS. Writing–review & editing: SJK, AHP, SVN, AY, RMS.
Acknowledgments
None.
Figure 1.Flowchart of the study.
Figure 2.Receiver operating characteristic (ROC) curve analysis of optic nerve sheath diameter.
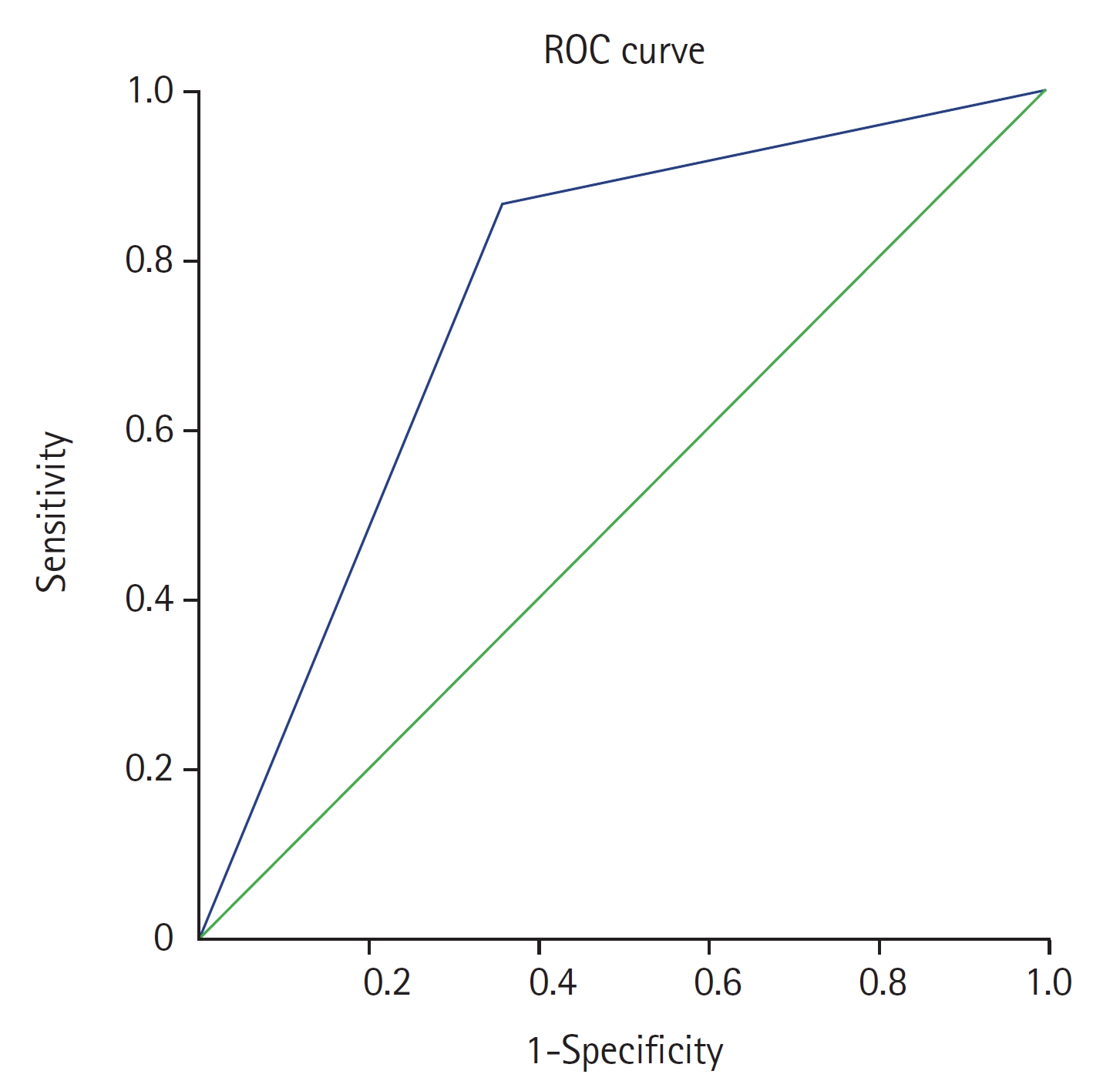
Table 1.Glasgow Coma Scale
|
Component assessed |
Score |
|
Eye response |
Spontaneous eye opening |
4 |
|
Opens eyes to verbal command |
3 |
|
Opens eyes to pain stimulus |
2 |
|
No eye opening |
1 |
|
Motor response |
Obeys commands |
6 |
|
Localizes pain |
5 |
|
Withdraws from pain |
4 |
|
Flexor response to pain |
3 |
|
Extensor response to pain |
2 |
|
No motor response |
1 |
|
Verbal response |
Oriented |
5 |
|
Confused |
4 |
|
Inappropriate words |
3 |
|
Incomprehensible sounds |
2 |
|
No verbal response |
1 |
|
Total score |
15 |
Table 2.Patient age distribution with mean ONSD values
|
Age (yr) |
ONSD ≥5.0 mm
|
Eye
|
ONSD of both eyes (mm) |
P-value |
|
Yes |
No |
Right (mm) |
Left (mm) |
|
20–30 (n=13) |
12 |
1 |
6.7±1.4 |
5.9±0.7 |
6.3±1.2 |
0.842 |
|
30–40 (n=25) |
22 |
3 |
6.4±1.2 |
6.0±0.9 |
6.2±1.1 |
|
40–50 (n=31) |
25 |
6 |
6.5±1.3 |
5.8±0.8 |
6.2±1.1 |
|
50–60 (n=18) |
16 |
2 |
6.3±1.3 |
5.9±1.0 |
6.1±1.1 |
|
>60 (n=8) |
7 |
1 |
5.6±0.8 |
5.4±0.6 |
5.5±0.7 |
Table 3.Patient characteristics including sex distribution, GCS, CT scan findings, and ventilator support requirement
|
Parameter |
ONSD
|
P-value |
|
>5.0 mm |
<5.0 mm |
Mean±SD |
|
Sex |
|
|
|
0.072 |
|
Male (n=65) |
48 (73) |
17 (26) |
6.2±1.1 |
|
|
Female (n=30) |
27 (90) |
3 (10) |
6.1±1.2 |
|
GCS |
|
|
|
<0.001 |
|
Severe (2–8, n=82) |
71(86) |
11 (13) |
6.4±1.0 |
|
|
Moderate (9–12, n=13) |
4 (30) |
9 (69) |
4.7±0.4 |
|
CT scan |
|
|
|
<0.001 |
|
Positive (raised ICP, n=81) |
70 (86) |
11 (13) |
- |
|
|
Normal (normal ICP, n=14) |
5 (35) |
9 (64) |
- |
|
Ventilatory support |
|
|
|
<0.001 |
|
Yes (n=83) |
72 (86) |
11 (13) |
- |
|
|
No (n=12) |
3 (25) |
9 (75) |
- |
Table 4.Area under the curve
|
Area under the curve |
Standard error |
Asymptotic significance |
Asymptotic 95% confidence interval
|
|
Lower bound |
Upper bound |
|
0.754 |
0.080 |
0.003 |
0.597 |
0.910 |
References
- 1. Soldatos T, Karakitsos D, Chatzimichail K, Papathanasiou M, Gouliamos A, Karabinis A. Optic nerve sonography in the diagnostic evaluation of adult brain injury. Crit Care 2008;12:R67. ArticlePubMedPMC
- 2. Moretti R, Pizzi B, Cassini F, Vivaldi N. Reliability of optic nerve ultrasound for the evaluation of patients with spontaneous intracranial hemorrhage. Neurocrit Care 2009;11:406-10.ArticlePubMedPDF
- 3. Moretti R, Pizzi B. Optic nerve ultrasound for detection of intracranial hypertension in intracranial hemorrhage patients: confirmation of previous findings in a different patient population. J Neurosurg Anesthesiol 2009;21:16-20.PubMed
- 4. Dubourg J, Javouhey E, Geeraerts T, Messerer M, Kassai B. Ultrasonography of optic nerve sheath diameter for detection of raised intracranial pressure: a systematic review and meta-analysis. Intensive Care Med 2011;37:1059-68.ArticlePubMedPDF
- 5. Geeraerts T, Launey Y, Martin L, Pottecher J, Vigué B, Duranteau J, et al. Ultrasonography of the optic nerve sheath may be useful for detecting raised intracranial pressure after severe brain injury. Intensive Care Med 2007;33:1704-11.ArticlePubMedPDF
- 6. Geeraerts T, Merceron S, Benhamou D, Vigué B, Duranteau J. Non-invasive assessment of intracranial pressure using ocular sonography in neurocritical care patients. Intensive Care Med 2008;34:2062-7.ArticlePubMedPDF
- 7. Kimberly HH, Shah S, Marill K, Noble V. Correlation of optic nerve sheath diameter with direct measurement of intracranial pressure. Acad Emerg Med 2008;15:201-4.ArticlePubMed
- 8. Kaur A, Gautam PL, Sharma S, Singh VP, Sharma S. Bedside ultrasonographic assessment of optic nerve sheath diameter as a means of detecting raised intracranial pressure in neuro-trauma patients: a cross-sectional study. Ann Indian Acad Neurol 2021;24:63-8.ArticlePubMed
- 9. Raffiz M, Abdullah JM. Optic nerve sheath diameter measurement: a means of detecting raised ICP in adult traumatic and non-traumatic neurosurgical patients. Am J Emerg Med 2017;35:150-3.ArticlePubMed
- 10. Zhu S, Cheng C, Zhao D, Zhao Y, Liu X, Zhang J. The clinical and prognostic values of optic nerve sheath diameter and optic nerve sheath diameter/eyeball transverse diameter ratio in comatose patients with supratentorial lesions. BMC Neurol 2021;21:259. ArticlePubMedPMCPDF
- 11. Helmke K, Hansen HC. Fundamentals of transorbital sonographic evaluation of optic nerve sheath expansion under intracranial hypertension : II. patient study. Pediatr Radiol 1996;26:706-10.ArticlePubMedPDF
- 12. Yanamandra U, Gupta A, Yanamandra S, Das SK, Patyal S, Nair V. Bedside ultrasonography as an alternative to computed tomography scan for the measurement of optic nerve sheath diameter. J Neurosci Rural Pract 2018;9:252-5.ArticlePubMedPMC
- 13. Tayal VS, Neulander M, Norton HJ, Foster T, Saunders T, Blaivas M. Emergency department sonographic measurement of optic nerve sheath diameter to detect findings of increased intracranial pressure in adult head injury patients. Ann Emerg Med 2007;49:508-14.ArticlePubMed
- 14. Blaivas M, Theodoro D, Sierzenski PR. Elevated intracranial pressure detected by bedside emergency ultrasonography of the optic nerve sheath. Acad Emerg Med 2003;10:376-81.ArticlePubMed
- 15. Gauthey M, Tessaro MO, Breitbart S, Kulkarni AV, Davis AL. Reliability and feasibility of optic nerve point-of-care ultrasound in pediatric patients with ventricular shunts. Childs Nerv Syst 2022;38:1289-95.ArticlePubMedPDF
- 16. Rajajee V, Vanaman M, Fletcher JJ, Jacobs TL. Optic nerve ultrasound for the detection of raised intracranial pressure. Neurocrit Care 2011;15:506-15.ArticlePubMedPDF
- 17. Bittencourt Rynkowski C, Caldas J. Ten good reasons to practice neuroultrasound in critical care setting. Front Neurol 2022;12:799421. ArticlePubMedPMC
- 18. Beckmann U, Gillies DM, Berenholtz SM, Wu AW, Pronovost P. Incidents relating to the intra-hospital transfer of critically ill patients: an analysis of the reports submitted to the Australian Incident Monitoring Study in Intensive Care. Intensive Care Med 2004;30:1579-85.ArticlePubMedPDF
- 19. Aliaga M, Forel JM, De Bourmont S, Jung B, Thomas G, Mahul M, et al. Diagnostic yield and safety of CT scans in ICU. Intensive Care Med 2015;41:436-43.ArticlePubMedPDF
- 20. Caruana M, Culp K. Intrahospital transport of the critically ill adult: a research review and implications. Dimens Crit Care Nurs 1998;17:146-56.PubMed
- 21. Dinsmore M, Venkatraghavan L. Clinical applications of point-of-care ultrasound in brain injury: a narrative review. Anaesthesia 2022;77 Suppl 1:69-77.ArticlePubMedPDF
- 22. Wang LJ, Chen LM, Chen Y, Bao LY, Zheng NN, Wang YZ, et al. Ultrasonography assessments of optic nerve sheath diameter as a noninvasive and dynamic method of detecting changes in intracranial pressure. JAMA Ophthalmol 2018;136:250-6.ArticlePubMedPMC
- 23. Hirzallah MI, Lochner P, Hafeez MU, Lee AG, Krogias C, Dongarwar D, et al. Quality assessment of optic nerve sheath diameter ultrasonography: scoping literature review and Delphi protocol. J Neuroimaging 2022;32:808-24.ArticlePubMedPDF
- 24. Montorfano L, Yu Q, Bordes SJ, Sivanushanthan S, Rosenthal RJ, Montorfano M. Mean value of B-mode optic nerve sheath diameter as an indicator of increased intracranial pressure: a systematic review and meta-analysis. Ultrasound J 2021;13:35. ArticlePubMedPMCPDF
Citations
Citations to this article as recorded by

- Measurement of Optic Nerve Sheath Diameter by Bedside Ultrasound in Patients With Traumatic Brain Injury Presenting to Emergency Department: A Review
Preethy Koshy, Charuta Gadkari
Cureus.2024;[Epub] CrossRef

 , Anandkumar H. Pande
, Anandkumar H. Pande

 PubReader
PubReader ePub Link
ePub Link Cite
Cite


