
Articles
- Page Path
- HOME > Acute Crit Care > Volume 39(1); 2024 > Article
-
Image in Critical Care
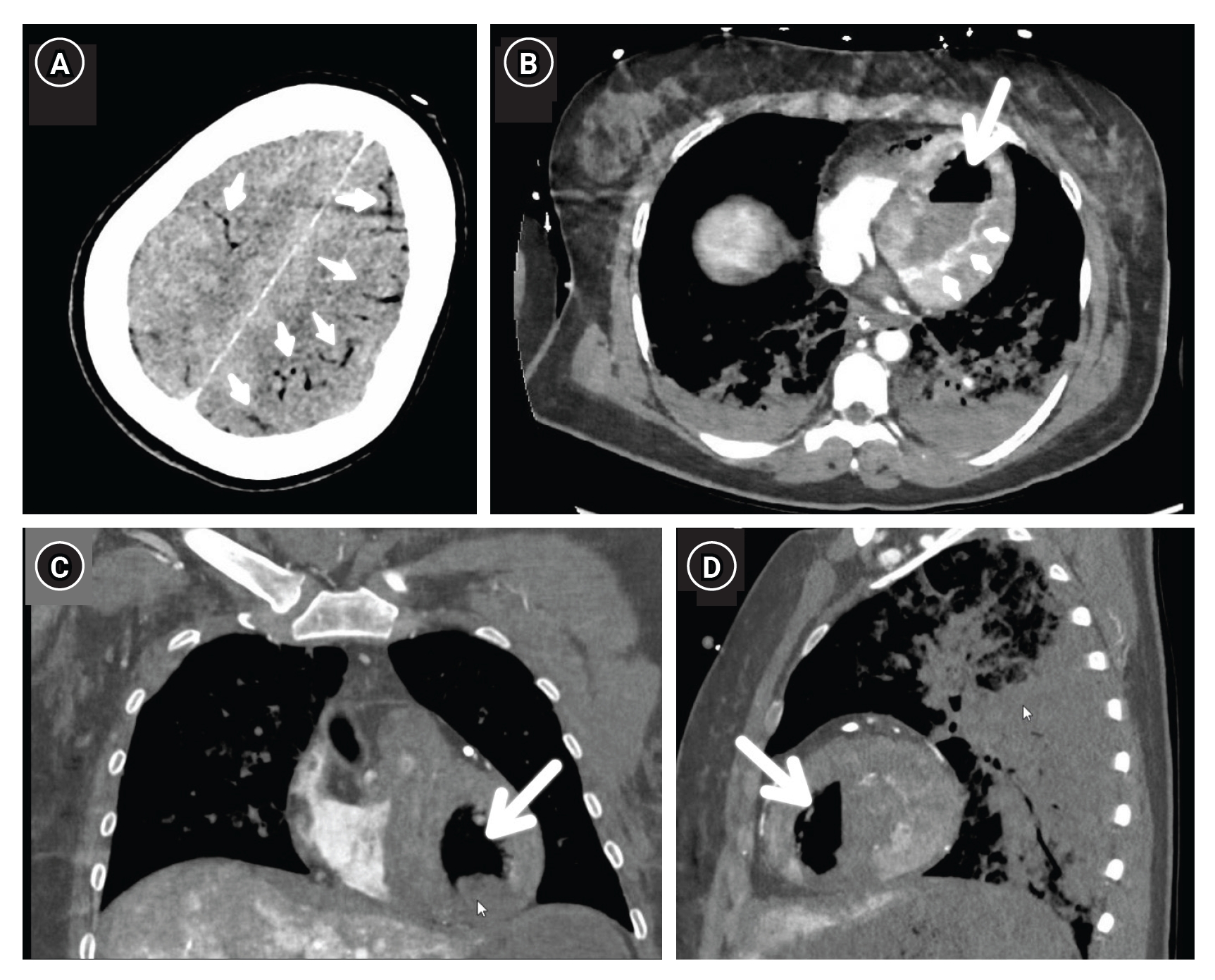
CPR/Resuscitation An unusual case of relapsing arrhythmia during veno-arterial extracorporeal membrane oxygenation cannulation -
Ruth Van Lancker1
 , Tim Balthazar1,2, Stijn Lochy1,2, Michaël Mekeirele1
, Tim Balthazar1,2, Stijn Lochy1,2, Michaël Mekeirele1 -
Acute and Critical Care 2024;39(1):201-202.
DOI: https://doi.org/10.4266/acc.2023.01032
Published online: February 15, 2024
1Intensive Care Department, Universitair Ziekenhuis Brussel, Vrije Universiteit Brussel, Jette, Belgium
2Department of Cardiology, Universitair Ziekenhuis Brussel, Vrije Universiteit Brussel, Jette, Belgium
- Corresponding author: Ruth Van Lancker Intensive Care Department, Universitair Ziekenhuis Brussel, Laarbeeklaan 101, 1090 Jette, Belgium Tel: +32-2801-2721 Fax: +32-2477-7780 E-mail: ruth.vanlancker@uzbrussel.be
© 2024 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 712 Views
- 58 Download
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: RVL, TB, MM. Methodology: RVL, TB, MM. Formal analysis: RVL, TB. Data curation: RVL, TB, SL. Visualization: RVL. Project administration: RVL. Writing–original draft: RVL. Writing–review & editing: all authors.
-
ACKNOWLEDGMENTS
The Institutional Review Board has approved this study with exempt for informed consent.
NOTES
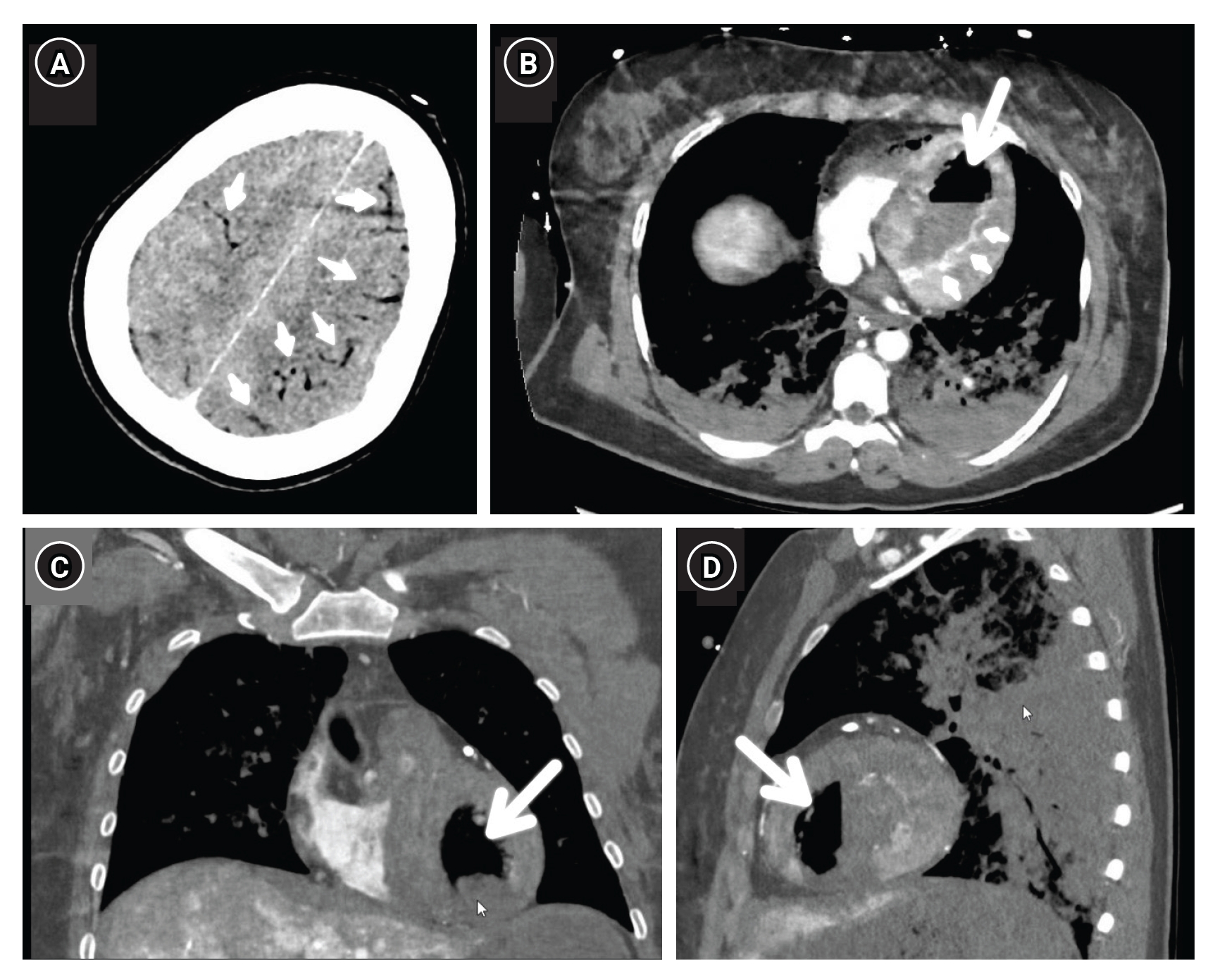
- 1. Malik N, Claus PL, Illman JE, Kligerman SJ, Moynagh MR, Levin DL, et al. Air embolism: diagnosis and management. Future Cardiol 2017;13:365-78.ArticlePubMed
- 2. Kandori K, Ishii W, Iiduka R. Massive systemic arterial air embolism caused by an air shunt after blunt chest trauma: a case report. Int J Surg Case Rep 2018;51:368-71.ArticlePubMedPMC
- 3. Ryu SM, Park SM. Unexpected complication during extracorporeal membrane oxygenation support: ventilator associated systemic air embolism. World J Clin Cases 2018;6:274-8.ArticlePubMedPMC
- 4. Shiina G, Shimosegawa Y, Kameyama M, Onuma T. Massive cerebral air embolism following cardiopulmonary resuscitation. Report of two cases. Acta Neurochir (Wien) 1993;125:181-3.ArticlePubMedPDF
References
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-
- Related articles
-
- Transjugular central venous catheter guidewire embolism to venoarterial extracorporeal membrane oxygenation cannula
- Dangers in using beta-blockers in patients with venovenous extracorporeal membrane oxygenation
- The role of nafamostat mesilate as a regional anticoagulant during extracorporeal membrane oxygenation
- Awakening in extracorporeal membrane oxygenation as a bridge to lung transplantation

