Articles
- Page Path
- HOME > Acute Crit Care > Volume 38(3); 2023 > Article
-
Review Article
Trauma Mobilization phases in traumatic brain injury -
Tommy Alfandy Nazwar1
 , Ivan Triangto2, Gutama Arya Pringga2, Farhad Bal’afif1, Donny Wisnu Wardana1
, Ivan Triangto2, Gutama Arya Pringga2, Farhad Bal’afif1, Donny Wisnu Wardana1 -
Acute and Critical Care 2023;38(3):261-270.
DOI: https://doi.org/10.4266/acc.2023.00640
Published online: August 18, 2023
1Division of Neurosurgery, Department of Surgery, Brawijaya University/Saiful Anwar Hospital Malang, East Java, Indonesia
2Department of Physical Medicine and Rehabilitation, Brawijaya University/Saiful Anwar Hospital Malang, East Java, Indonesia
- Corresponding author: Tommy Alfandy Nazwar Division of Neurosurgery, Department of Surgery, Brawijaya University/Saiful Anwar Hospital Malang, Brawijaya, RSUD Dr Saiful Anwar SMF Bedah Saraf Gedung GPT II 2nd floor, Malang, East Java 65112, Indonesia Tel: +62-83-1375-2620, Fax: +62-33-3100, E-mail: tommy@ub.ac.id
Copyright © 2023 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- Abstract
- INTRODUCTION
- PHYSIOLOGICAL EFFECTS OF MOBILIZATION
- MOBILIZATION GUIDELINE IN TBI
- MOBILIZATION PRECAUTIONS IN TBI
- MOBILIZATION PRECAUTION IN PATIENTS WITH TBI TREATED WITH EXTRA VENTRICULAR DRAINS
- MOBILIZATION TECHNIQUE
- COGNITION IN TBI AND REHABILITATIVE ASPECT
- NUTRITIONAL ISSUES IN TBI PATIENTS
- CONCLUSIONS
- KEY MESSAGES
- NOTES
- Acknowledgments
- References
Abstract
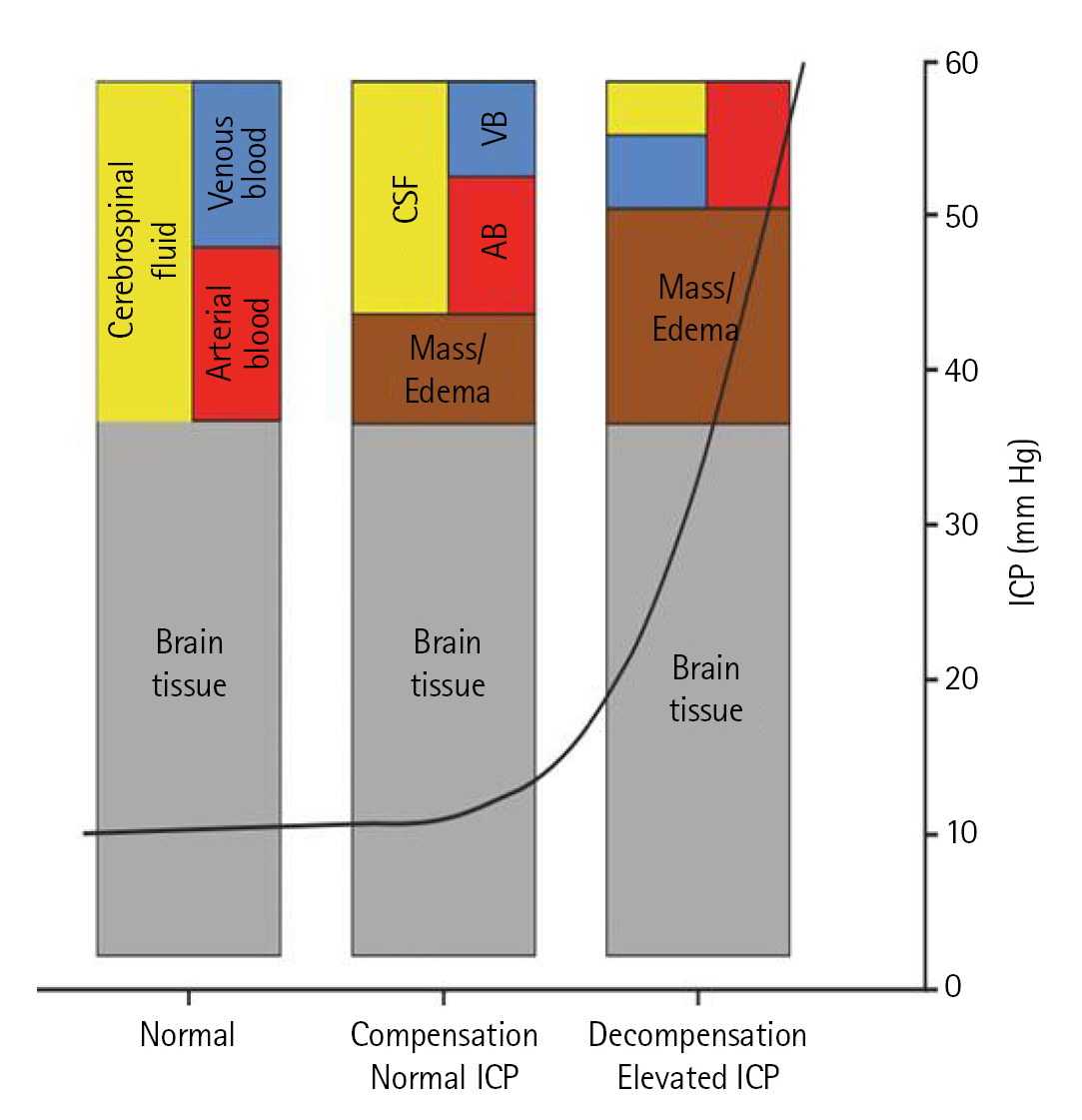
- Mobilization in traumatic brain injury (TBI) have shown the improvement of length of stay, infection, long term weakness, and disability. Primary damage as a result of trauma’s direct effect (skull fracture, hematoma, contusion, laceration, and nerve damage) and secondary damage caused by trauma’s indirect effect (microvasculature damage and pro-inflammatory cytokine) result in reduced tissue perfusion and edema. These can be facilitated through mobilization, but several precautions must be recognized as mobilization itself may further deteriorate patient’s condition. Very few studies have discussed in detail regarding mobilizing patients in TBI cases. Therefore, the scope of this review covers the detail of physiological effects, guideline, precautions, and technique of mobilization in patients with TBI.
INTRODUCTION
PHYSIOLOGICAL EFFECTS OF MOBILIZATION
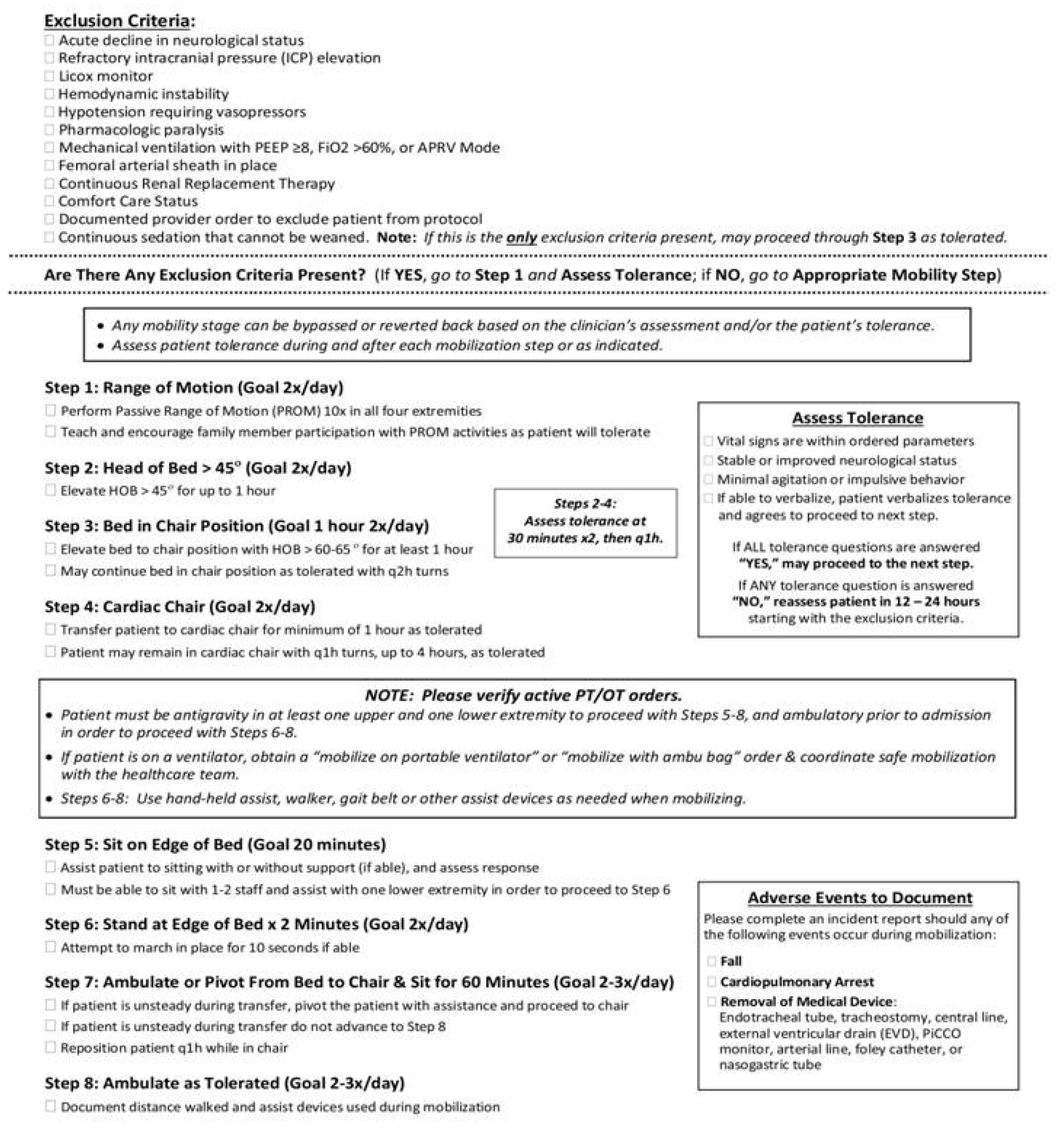
MOBILIZATION GUIDELINE IN TBI
MOBILIZATION PRECAUTIONS IN TBI
MOBILIZATION PRECAUTION IN PATIENTS WITH TBI TREATED WITH EXTRA VENTRICULAR DRAINS
MOBILIZATION TECHNIQUE
COGNITION IN TBI AND REHABILITATIVE ASPECT
NUTRITIONAL ISSUES IN TBI PATIENTS
CONCLUSIONS
KEY MESSAGES
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: TAN, GAP, FB, DWW. Formal analysis: TAN, IT. Data curation: IT. Visualization: IT. Writing–original draft: IT, GAP. Writing–review & editing: TAN, FB, DWW.
NOTES
Acknowledgments

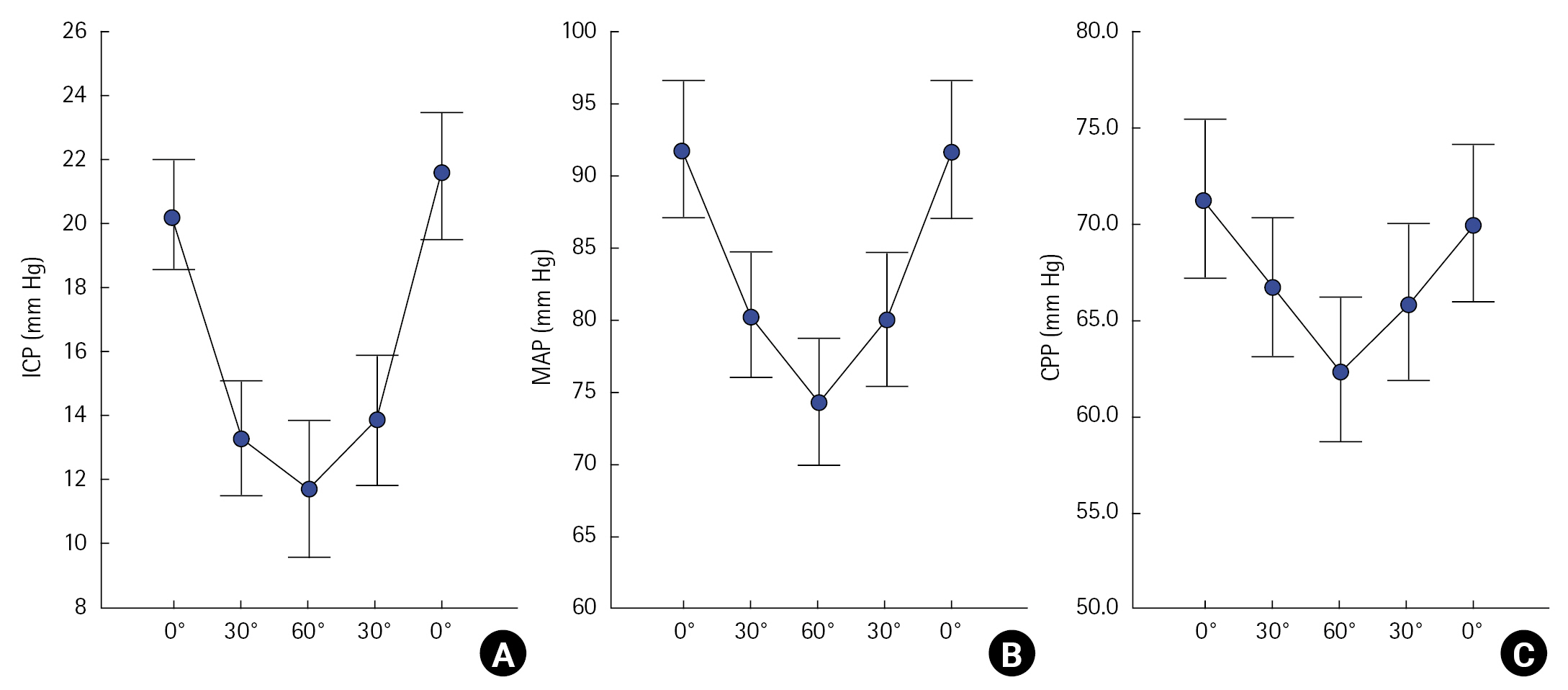
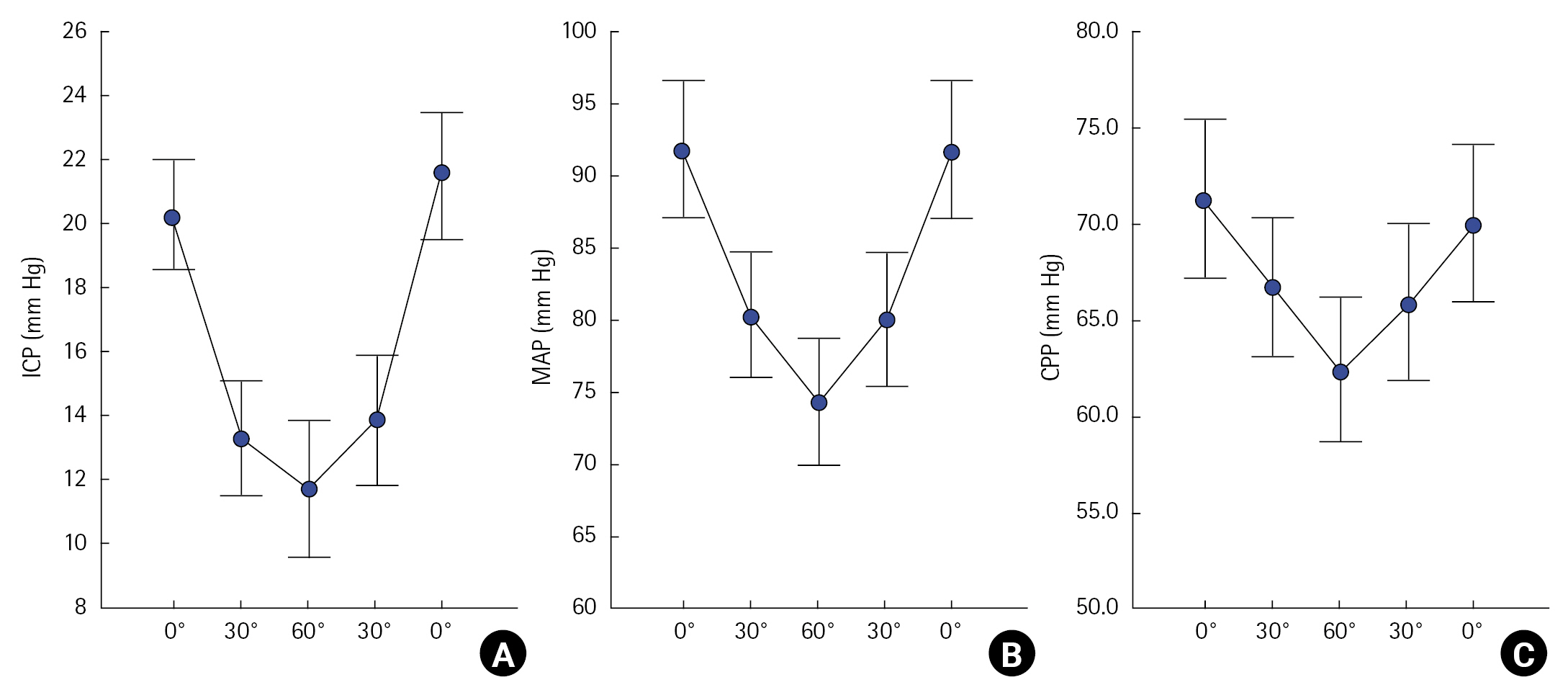
| Variable | 0° | 30° | 60° | 30° | 0° |
|---|---|---|---|---|---|
| ICP | 20.3±0.9 | 13.4±0.9 | 11.8±1.1 | 13.8±1.1 | 21.6±1.0 |
| CPP | 72.8±2.2 | 67.5±2.0 | 62.6±2.2 | 66.8±2.2 | 70.8±2.2 |
| MAP | 93.0±2.4 | 80.1±2.2 | 74.4±2.3 | 80.6±2.4 | 92.4±2.5 |
- 1. Ai W, Venkatachalam L, Molawi SA, Kuwari FA. Traumatic brain injury rehabilitation: an overview. In: Farid Sadaka. In: Traumatic brain injury. InTech. 2014.
- 2. Brissie MA, Zomorodi M, Soares-Sardinha S, Jordan JD. Development of a neuroearly mobilisation protocol for use in a neuroscience intensive care unit. Intensive Crit Care Nurs 2017;42:30-5.ArticlePubMed
- 3. Altun Uğraş G, Yüksel S, Temiz Z, Eroğlu S, Şirin K, Turan Y. Effects of different head-of-bed elevations and body positions on intracranial pressure and cerebral perfusion pressure in neurosurgical patients. J Neurosci Nurs 2018;50:247-51.ArticlePubMed
- 4. Gaspari CH, Lafayette S, Jaccoud AC, Kurtz P, Lavradas LA Jr, Cavalcanti DD. Safety and feasibility of out-of-bed mobilization for patients with external ventricular drains in a neurosurgical intensive care unit. J Acute Care Phys Ther 2018;9:171-8.Article
- 5. Kawoos U, McCarron RM, Auker CR, Chavko M. Advances in intracranial pressuremonitoring and its significance in managing traumatic brain injury. Int J Mol Sci 2015;16:28979-97.ArticlePubMedPMC
- 6. Thal SC. Intensive care management of head-injured patient. In: Prabhakar H, , Ali Z. In: Textbook of neuroanesthesia and neurocritical care. Springer Singapore. 2019, pp 157-65.
- 7. Petersen LG, Petersen JC, Andresen M, Secher NH, Juhler M. Posturalinfluence on intracranial and cerebral perfusion pressure in ambulatoryneurosurgical patients. Am J Physiol Regul Integr Comp Physiol 2016;310:R100-4.ArticlePubMed
- 8. Chitteti P, George AS, Nair S, Karuppasamy R, Joseph M. Adherence to head-of-bed elevation in traumatic brain injury: an audit. J Neuroanaesthesiol Crit Care 2022;9:177-82.Article
- 9. Sattur MG, Patel SJ, Helke KL, Donohoe M, Spiotta AM. Head elevation, cerebral venous system, and intracranial pressure: review and hypothesis. Stroke Vasc Interv Neurol 2022;3:e000522.Article
- 10. Mahfoud F, Beck J, Raabe A. Intracranial pressure pulse amplitude duringchanges in head elevation: a new parameter for determining optimum cerebralperfusion pressure? Acta Neurochir (Wien) 2010;152:443-50.ArticlePubMedPDF
- 11. Mitchell PH, Kirkness C, Blissitt PA. Chapter 5 cerebral perfusion pressureand intracranial pressure in traumatic brain injury. Annu Rev Nurs Res 2015;33:111-83.ArticlePubMed
- 12. Sands E, Wong L, Lam MY, Panerai RB, Robinson TG, Minhas JS. The effects ofgradual change in head positioning on the relationship between systemic andcerebral haemodynamic parameters in healthy controls and acute ischaemic strokepatients. Brain Sci 2020;10:582. ArticlePubMedPMC
- 13. Nagarathinam V, Muthusamy R, Ramachandran S. Effectiveness of mobilization to sitting in improving arousal at various durations in traumatic brain injury patients. Indian J Public Health Res Dev 2019;10:399-404.Article
- 14. Young B, Moyer M, Pino W, Kung D, Zager E, Kumar MA. Safety and feasibilityof early mobilization in patients with subarachnoid hemorrhage and externalventricular drain. Neurocrit Care 2019;31:88-96.ArticlePubMedPDF
- 15. Borges LF, Fraga Righetti R, de Souza Francisco D, Pereira Yamaguti W. Hemodynamic impact of early mobilization in critical patients receivingvasoactive drugs: a prospective cohort study. PLoS One 2022;17:e0279269.ArticlePubMedPMC
- 16. Tipping CJ, Bailey MJ, Bellomo R, Berney S, Buhr H, Denehy L, et al. The ICU Mobility Scale has constructand predictive validity and is responsive: a multicenter observational study. Ann Am Thorac Soc 2016;13:887-93.ArticlePubMed
- 17. Sommers J, Engelbert RH, Dettling-Ihnenfeldt D, Gosselink R, Spronk PE, Nollet F, et al. Physiotherapy in the intensive care unit: anevidence-based, expert driven, practical statement and rehabilitationrecommendations. Clin Rehabil 2015;29:1051-63.ArticlePubMedPMCPDF
- 18. Kisner C, Colby LA, Borstad J. Therapeutic exercise: foundations and techniques. 7th ed. F. A. Davis Company. 2018.
- 19. Seo B, Shin WS. Effects of functional training on strength, function level, and quality of life of persons in intensive care units. Phys Ther Rehabil Sci 2019;8:134-40.Article
- 20. Kocan MJ, Lietz H. Special considerations for mobilizing patients in the neurointensive care unit. Crit Care Nurs Q 2013;36:50-5.ArticlePubMed
- 21. Monaghan HM, McWilliams D, Cook S, Klein LM, Kumble KS, Friedman M, et al. Early mobility. Int J Safe Patient Handl Mov 2022;special issue:SI-35.
- 22. Kubota S, Endo Y, Kubota M, Ishizuka Y, Furudate T. Effects of trunk posturein Fowler’s position on hemodynamics. Auton Neurosci 2015;189:56-9.ArticlePubMed
- 23. Vatwani A. Caregiver guide and instructions for safe bed mobility. Arch PhysMed Rehabil 2017;98:1907-10.Article
- 24. Cifu DX, Johns JS. Braddom’s physical medicine and rehabilitation. 6th ed. Elsevier. 2021.
- 25. Sharma B, Allison D, Tucker P, Mabbott D, Timmons BW. Cognitive and neuraleffects of exercise following traumatic brain injury: a systematic review ofrandomized and controlled clinical trials. Brain Inj 2020;34:149-59.ArticlePubMed
- 26. Dresen E, Weißbrich C, Fimmers R, Putensen C, Stehle P. Medical high-proteinnutrition therapy and loss of muscle mass in adult ICU patients: a randomizedcontrolled trial. Clin Nutr 2021;40:1562-70.ArticlePubMed
- 27. Bear DE, Puthucheary Z. Potential nutritional strategies to reduce muscle wasting in early critical illnes. ICU Manag Pract 2016;16:109-11.
- 28. Zhou W, Yu L, Fan Y, Shi B, Wang X, Chen T, et al. Effect of early mobilization combined with early nutrition on acquired weakness in critically ill patients (EMAS): a dual-center, randomized controlled trial. PLoS One 2022;17:e0268599.ArticlePubMedPMC
- 29. Chapple LS, Parry SM, Schaller SJ. Attenuating muscle mass loss in criticalillness: the role of nutrition and exercise. Curr Osteoporos Rep 2022;20:290-308.ArticlePubMedPMCPDF
References
Figure & Data
References
Citations
- Acute orthostatic responses during early mobilisation of patients with acquired brain injury - Innowalk pro versus standing frame
Matthijs F Wouda, Espen I Bengtson, Ellen Høyer, Alhed P Wesche, Vivien Jørgensen
Journal of Rehabilitation and Assistive Technologies Engineering.2024;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite