Abstract
-
Background
- Coronavirus disease 2019 (COVID-19) patients with acute respiratory failure who experience delayed initiation of invasive mechanical ventilation have poor outcomes. The lack of objective measures to define the timing of intubation is an area of concern. We investigated the effect of timing of intubation based on respiratory rate-oxygenation (ROX) index on the outcomes of COVID-19 pneumonia.
-
Methods
- This was a retrospective cross-sectional study performed in a tertiary care teaching hospital in Kerala, India. Patients with COVID-19 pneumonia who were intubated were grouped into early intubation (within 12 hours of ROX index <4.88) or delayed intubation (12 hours or more hours after ROX <4.88).
-
Results
- A total of 58 patients was included in the study after exclusions. Among them, 20 patients were intubated early, and 38 patients were intubated 12 hours after ROX index <4.88. The mean age of the study population was 57±14 years, and 55.0% of the patients were male; diabetes mellitus (48.3%) and hypertension (50.0%) were the most common comorbidities. The early intubation group had 88.2% successful extubation, while only 11.8% of the delayed group had successful extubation (P<0.001). Survival was also significantly more frequent in the early intubation group.
-
Conclusions
- Early intubation within 12 hours of ROX index <4.88 was associated with improved extubation and survival in patients with COVID-19 pneumonia.
-
Keywords: airway extubation; artificial respiration; COVID-19; cross-sectional study; intratracheal intubation; survival analysis
INTRODUCTION
The clinical presentation of coronavirus disease 2019 (COVID-19) ranges from asymptomatic illness to severe acute respiratory distress syndrome (ARDS). Approximately 20%–25% of patients with COVID-19 admitted to the hospital require critical care management [1]. Management of hypoxemia and respiratory failure in these patients has presented new challenges. The oxygen therapy has included nasal prongs with low-flow oxygen, non-rebreathing mask, bilevel positive airway pressure (BiPAP), high-flow nasal oxygen (HFNO), and mechanical ventilation. An important concern faced by the intensivist was how to predict the need for invasive mechanical ventilation (IMV) and when to initiate ventilation in these patients. During the first wave of the pandemic, there was a drive for early intubation based on data from China due to fears of rapidly progressing hypoxemia, concerns about patient self-inflicted lung injury (P-SILI), and risk of aerosolization when using non-invasive techniques [2]. Reports from various centers regarding the increased morbidity and mortality of the ventilated patients led to scepticism regarding the early intubation protocol. The argument was that the perils of mechanical ventilation such as ventilator-induced lung injury and ventilator-associated pneumonia can lead to poor outcomes [3]. This led to increased use of alternate techniques of oxygenation such as HFNO, which could avoid intubation in some patients. However, the mortality and morbidity are worse in patients who fail the HFNO trial and require intubation [4]. The criteria for definition of early and delayed intubation differ by study. An objective method to identify subjects who are likely to fail to respond to non-invasive oxygen therapy is needed.
Roca and colleagues first published the respiratory rate-oxygenation (ROX) index, which can predict whether a pneumonia patient will fail treatment using high-flow nasal cannula. The authors reported that ROX >4.88 predicted the success of HFNO to prevent intubation [5]. A retrospective cohort study by Patel et al. [6] involved serial measurements of ROX index and showed that any decrease in the index from baseline over a 24-hour period of initiation of HFNO was a strong predictor of intubation .The ROX index has been used as a non-invasive tool in coronavirus disease patients to predict failure of HFNO and need for intubation [7,8]. However, there are no data as to whether the outcomes of mechanical ventilation are affected by timing of intubation based on ROX index in COVID-19.
This retrospective cross-sectional study was designed to observe the appropriate timing of intubation based on ROX index in patients with coronavirus pneumonia admitted to the intensive care unit (ICU). Our primary hypothesis was that early intubation in less than 12 hours of measurement of ROX index less than 4.88 is associated with successful extubation and improved survival.
MATERIALS AND METHODS
This single-center retrospective cross-sectional study was performed in a 16-bed COVID-19 ICU of a rural tertiary care hospital in Kerala, India. The study sample included all patient 18 years or older with laboratory confirmed COVID-19 who underwent mechanical ventilation in this ICU from April1, 2021 to July 31, 2021, during the second wave of the pandemic in Kerala. After Institutional Review Board approval (No. MOSC/IEC/566/2021), we obtained a waiver for informed consent due to the retrospective nature of the analysis from medical records. The details were evaluated using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist [9].
Positive infection status was confirmed either by rapid antigen testing or reverse transcriptase polymerase chain reaction of nasal or oropharyngeal swab. Patients referred to our center after intubation from another center and patients who opted for palliative care were excluded from the study. The variables collected were demographic characteristics, comorbidities, ratio of SpO2 to fraction of inspired oxygen (SpO2/FiO2) with respiratory rate (ROX index) every 6 hours from admission until intubation, Acute Physiology and Chronic Health Evaluation (APACHE) II score at admission, Sequential Organ Failure Assessment (SOFA) score at admission and at intubation, duration from proven COVID-19 diagnosis to intubation, day of extubation, duration of ICU and hospital stay, incidence of acute kidney injury, pneumothorax, and survival. The primary objective was successful extubation and survival pattern based on time of intubation.
After collection of demographic and clinical data, the intubated patients were categorized into two groups; the early intubation group was patients intubated within 12 hours of ROX index <4.88 and the delayed intubation group comprised patients intubated more than 12 hours after ROX index <4.88. Demographics, comorbidities, and outcomes of the two groups were compared. Patients were followed until hospital discharge or death.
Treatment Protocol in the ICU
Patients who were unable to maintain SpO2>90% on non-rebreather mask with 15 L/min of oxygen or non-invasive BiPAP were put on HFNO, which was initiated with a flow rate of 40–60 L/min and fraction of inspired oxygen (FiO2) titrated to maintain >90% SpO2. The intubation criteria were: (1) hypoxemic respiratory failure with SpO2 <90 % despite receiving the maximal fraction of inspired oxygen by HFNO; (2) hypercapnic respiratory failure accompanied by pH <7.3; (3) uncontrolled metabolic acidosis with hypotension (systolic blood pressure <90 mm Hg or mean blood pressure <65 mm Hg) despite fluid resuscitation; (4) need for airway protection because of altered mental state or aspiration or cardiopulmonary arrest.
The ROX index was measured every 6 hours in all patients on HFNO. Intubation was conducted according to the general guidelines and discretion of the treating physician. The intubated patients were sedated and paralyzed; prone ventilation was started for 12–16 hours each day until there was improvement in oxygenation. Remdesivir was the preferred antiviral agent. All patients admitted to the ICU received parenteral corticosteroids with either dexamethasone or methylprednisolone. Other drugs were anticoagulation with low-molecular weight heparin, prophylactic/therapeutic antibiotics, stress ulcer prophylaxis, nutritional support, vitamins/antioxidant supplements, and drugs according to underlying comorbidities.
Statistical Analysis
Continuous variables are presented as median and interquartile range (IQR) when data did not follow a normal distribution and as mean and standard deviation if data were normal. Qualitative variables are presented as frequencies and percentages. Fisher’s exact test and Pearson chi-square test were used to compare categorical variables. Variables that were clinically important or statistically significant in the univariate logistic regression were selected for multivariate analysis to isolate the contribution of intubation based on ROX index on successful extubation; the odds ratio was reported as effect estimate. Kaplan-Meier survival analysis was conducted to assess survival pattern based on time of intubation. Statistical significance was defined as P<0.05. Analyses were performed using R software (EZR software) and IBM SPSS ver.19 (IBM Corp.).
RESULTS
The second wave of COVID19 in Kerala, India was from April 2021 to July 2021. A total of 814 COVID19-positive patients was admitted to our hospital during this period, and 216 patients were admitted to the ICU. Among the critically ill, 70 patients were mechanically ventilated, 10 patients were intubated outside the ICU, one patient was transferred to another hospital, and palliative treatment was chosen for one patient. These patients were excluded from analysis (Figure 1). The final group included 58 patients; 20 patients were intubated within 12 hours of ROX index <4.88 (early intubation group) and 38 patients were intubated 12 hours after ROX index <4.88 (delayed intubation group).
The baseline characteristics of the 58 patients who were intubated in our ICU are listed in Table 1. The mean age of the study population was 56.8±13.7 years and 55.0% were males. Type II diabetes mellitus was present in 48.3% of the patients and 50.0% were hypertensive. One patient had a history of chronic liver disease and one patient had a history of treatment for breast carcinoma. The Charlson comorbidity index (CCI), APACHE II score at admission, median SOFA score at admission and intubation, and day of intubation after confirmed coronavirus disease were similar in the two groups. The mean ROX index at initiation of HFNO was 5.41±1.92 (Table 1).
The main outcome was successful extubation. In the group of patients intubated within 12 hours of ROX index <4.88, 88.2 % were extubated compared with only 11.8% of the late group (P<0.001). In the early intubation group, 91.7% of the patients survived until discharge from the hospital, which was significantly higher than the percentage of the delayed intubation group. Incidence of acute kidney injury was higher in the delayed intubation group, although without statistical significance. The median duration of ICU stay was 9 days (IQR, 5–13 days). The total numbers of days in the ICU and hospital were higher in the early intubation group (Table 2).
Other complications in the patients were shock requiring vasopressors (17.2%), arrhythmias, and myocardial ischemia/infarction (5%), but there was no difference between the two groups. Pneumothorax occurred in two patients in the delayed intubation group and in one patient in the early intubation group. Tracheostomy was performed in one patient in the delayed intubation group. Variables of clinical importance were selected for the logistic regression model and comprised age, sex, comorbidities, day of intubation after confirmed COVID-19 infection, and SOFA and APACHE scores. The analysis showed that early intubation within 12 hours of ROX index <4.88 was the only factor associated with successful extubation (P<0.001) (Table 3). Kaplan-Meier survival analysis showed that the median survival time was 14.8 days (95% confidence interval [CI], 12.2–17.4 days) for patients who had early intubation and 9.9 days (95% CI, 6.8–13.1 days) in the delayed intubation group (P=0.001) (Figure 2).
DISCUSSION
Deciding if and when to intubate and mechanically ventilate a patient with COVID-19 pneumonia is a difficult decision and is be based on both disease severity and provider judgment. The clinical presentation of COVID-19 varies from asymptomatic infection to severe respiratory distress, and the timing of initiation of IMV may have significant implications for patient outcomes [10]. This retrospective analysis of mechanically ventilated coronavirus disease patients showed that the timing of intubation based on ROX index may improve rates of successful extubation and survival.
The rate of IMV requirement varied in the first and second waves of the COVID-19 pandemic [11]. The proportion of COVID-19 patients who required mechanical ventilation in our study (32%) is similar to those in reports from a large tertiary care center in India [10]. Of the 23.5% patients with COVID-19 who required intensive care management, 30.8% required IMV. In a study from China, of 344 patients in the ICU, 100 (29.1%) required intubation [12]. The mean age (56.8±13.7 years) and sex (males 55.0%) of the patients requiring mechanical ventilation in our study population were similar to those of these previous studies. The most common comorbidities associated with severe COVID-19 disease in this study were hypertension and diabetes mellitus type II, similar to globally reported trends in severe COVID-19 patients [13,14]. The CCI was 2.16±1.47 in our study population. There was no statistically significant difference in CCI between early and delayed intubation groups in our study. A CCI index less than 5 was associated with higher survival rates in patients in the ICU in previously reported critically ill patients [15] but was not the case in our patient group.
In the present study, the median SOFA score at admission was 3 and SOFA at intubation was 4. Serial evaluation of SOFA scores during ICU admission is a good indicator of prognosis, and an increase in score during the first 48 hours predicts a 50% mortality rate [16,17]. However, in COVID-19 pneumonia, the discriminatory accuracy of SOFA for predicting mortality was poor and significantly inferior to using only age. The median SOFA score was only 6 (IQR, 4–8) in a previous study involving nearly 1,000 intubated COVID-19 patients with 59.3% mortality [18]. Thus, this clinical scoring system might be less accurate in COVID-19 pneumonia patients as such patients have severe single organ dysfunction (hypoxemia) and less variation in SOFA score. APACHE II seems to perform better in predicting severity of COVID-19 [10]. However, in this study, there was no statistically significant difference between the two groups for APACHE II score at admission to an ICU.
The ROX index is a simple scoring system devised to predict the failure of HFNO in acute hypoxemic respiratory failure [5]; it has shown utility in not just predicting intubation in COVID-19, but also the need for hospital admission [19]. Patel et al. [20] studied the utility of the ROX index in predicting the need for IMV in COVID-19 pneumonia patients and found that a score <5 at initiation predicted the need for IMV (odds ratio [OR], 2.137; P=0.052) . The mean time to intubation was 2.5 days with 47% mortality in patients requiring IMV. The average ROX index of the patients admitted to our ICU was 5.41±1.92 on initiation of HFNO.
In this study, we classified COVID-19 patients who required IMV in our ICU into two groups: one group was intubated within 12 hours of ROX index <4.88 (early) and the other group was intubated 12 hours or more after ROX index<4.88 (delayed). Successful extubation (88.2%) and higher survival were noted in the early intubation group. These observations are in agreement with multiple studies that showed early intubation after hospital admission in COVID-19 patients to be associated with favorable outcomes [10,21]. The systematic review and meta-analysis of non-randomized cohort studies by Papoutsi et al. [22] showed different results from ours in intubated COVID-19 patients. Those authors concluded that timing of intubation had no effect on mortality or morbidity of such critically ill patients. However, their definitions of early and late were intubation within 24 hours or after 24 hours of ICU admission. This definition was not related to patients’ clinical status and could be the reason for the difference in findings.
The decision to intubate patients with COVID-19 pneumonia is based on multiple factors and varies among centers and clinicians. The standard intubating criteria in acute hypoxemic respiratory failure used in non-COVID-19 patients might not be enough in these patients. Intubating COVID-19 patients early may have several benefits, like prevention of P-SILI due to spontaneous breathing with large tidal volumes and increasing respiratory effort [23]. Therefore, it is important to identify an objective score to predict the need for intubation that can lead to favorable outcomes, and ROX index fits this requirement.
Factors like age, comorbidities, APACHE and SOFA scores, or day of intubation after diagnosis of COVID-19 that can affect extubation and survival in critically ill patients were analyzed along with timing of intubation based on ROX index. Presence of acute kidney injury and hemodynamic compromise were not different in the patients who were successfully extubated. The multiple logistic regression analysis in this study showed the role of early intubation based on ROX index in extubation (Table 3).
The mortality rate (79.3%) in our study population of severe COVID-19 with IMV was high, and bleak outcomes have been reported in ventilated COVID-19 patients worldwide [24]. This study was performed during the second wave of the pandemic in Kerala, India, which had a higher case fatality rate [25] with more frequent severe ARDS than in the first wave. Early intubation based on ROX index improved survival in our study population as evidenced by Kaplan-Meier survival analysis (Figure 2), and this was not influenced by demographics or comorbidities of the patients.
A limitation of the present study is the small sample size. This was a single-center study performed in a medium-sized hospital that services a relatively small geographic area. Therefore, our results must be considered with caution. However, in a pandemic, any new information that can change the trajectory of the disease is relevant, and little information is available on an objective measure to decide when to intubate in COVID-19 patients with pneumonia and ARDS. A multi-centric prospective study for the use of ROX index in timing of intubation of these patients may provide robust evidence for a change in practice for treatment of COVID-19 patients.
In pneumonia due to COVID-19, early intubation within 12 hours of ROX index less than 4.88 is associated with improved chances of successful extubation and survival. As ROX index is a simple tool, its use as an objective method to predict failure of HFNO and to decide on IMV in patients with COVID-19 should be encouraged.
KEY MESSAGES
▪ There is need for methods to improve poor outcomes in coronavirus disease 2019 (COVID-19) patients with pneumonia who require mechanical ventilation.
▪ The respiratory rate-oxygenation (ROX) index can be used as an objective method to determine failure of non-invasive methods of oxygenation and timing of initiation of ventilation.
▪ In patients with COVID-19 pneumonia, early intubation within 12 hours of ROX index.
NOTES
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: SVK, MG. Methodology: VP, NCP, MT. Data curation: SVK, NCP, NP, MT. Visualization: VP, NCP. Project administration: SP. Writing–original draft: SVK. Writing–review & editing: SVK, VP, MG.
Acknowledgments
We acknowledge Dr. Kalesh M Karun and Dr. Sharon Baisil for statistical analysis.
Figure 1.Flowchart of patients with confirmed diagnosis of coronavirus disease 2019 (COVID-19) infection. NRBM: non-rebreather mask; HFNO: high-flow nasal oxygen; BiPAP: bilevel positive airway pressure; ROX: respiratory rate-oxygenation.
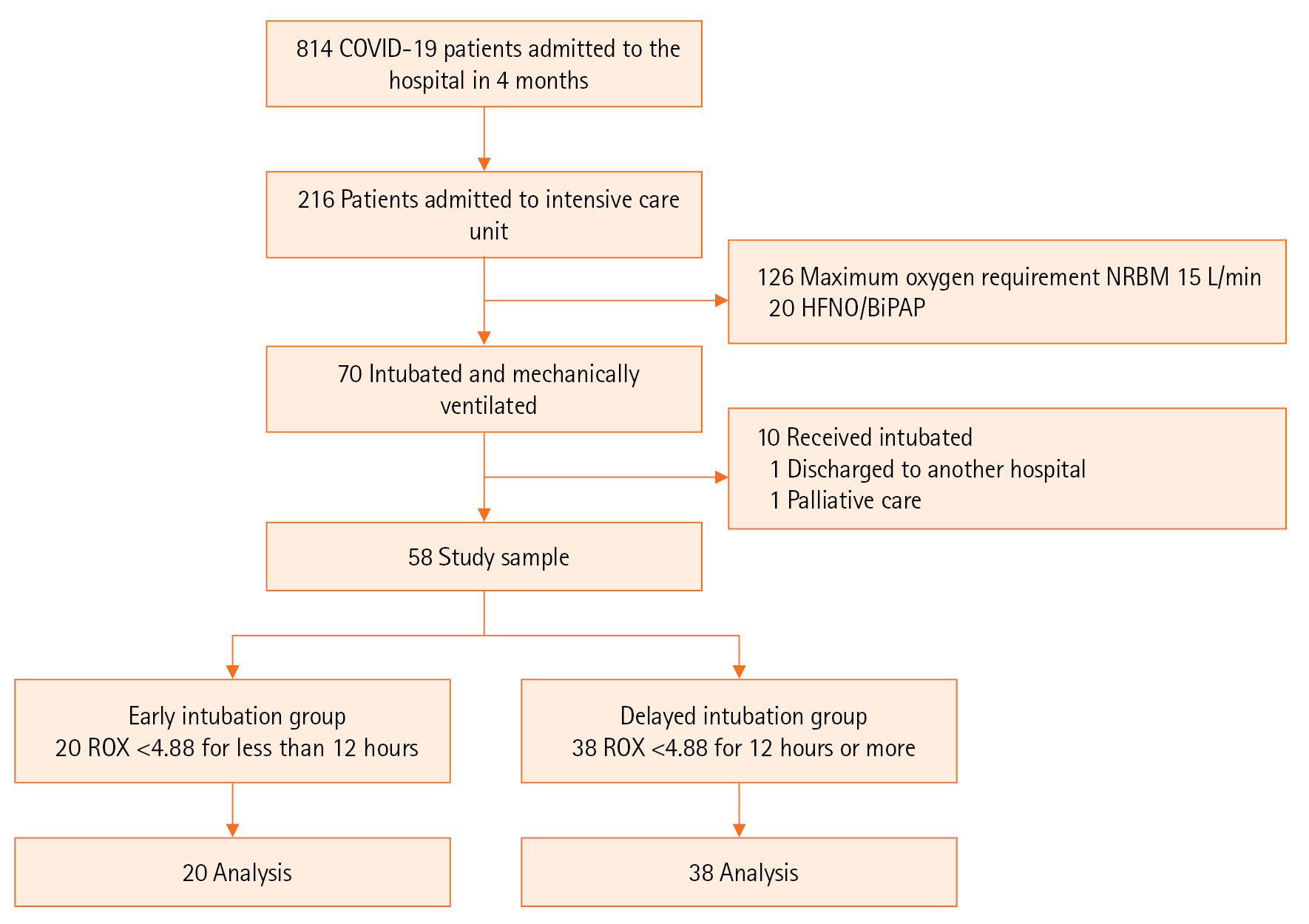
Figure 2.Kaplan-Meier plots for survival of patients with coronavirus disease 2019 (COVID-19) pneumonia and early or delayed intubation. ROX: respiratory rate-oxygenation.
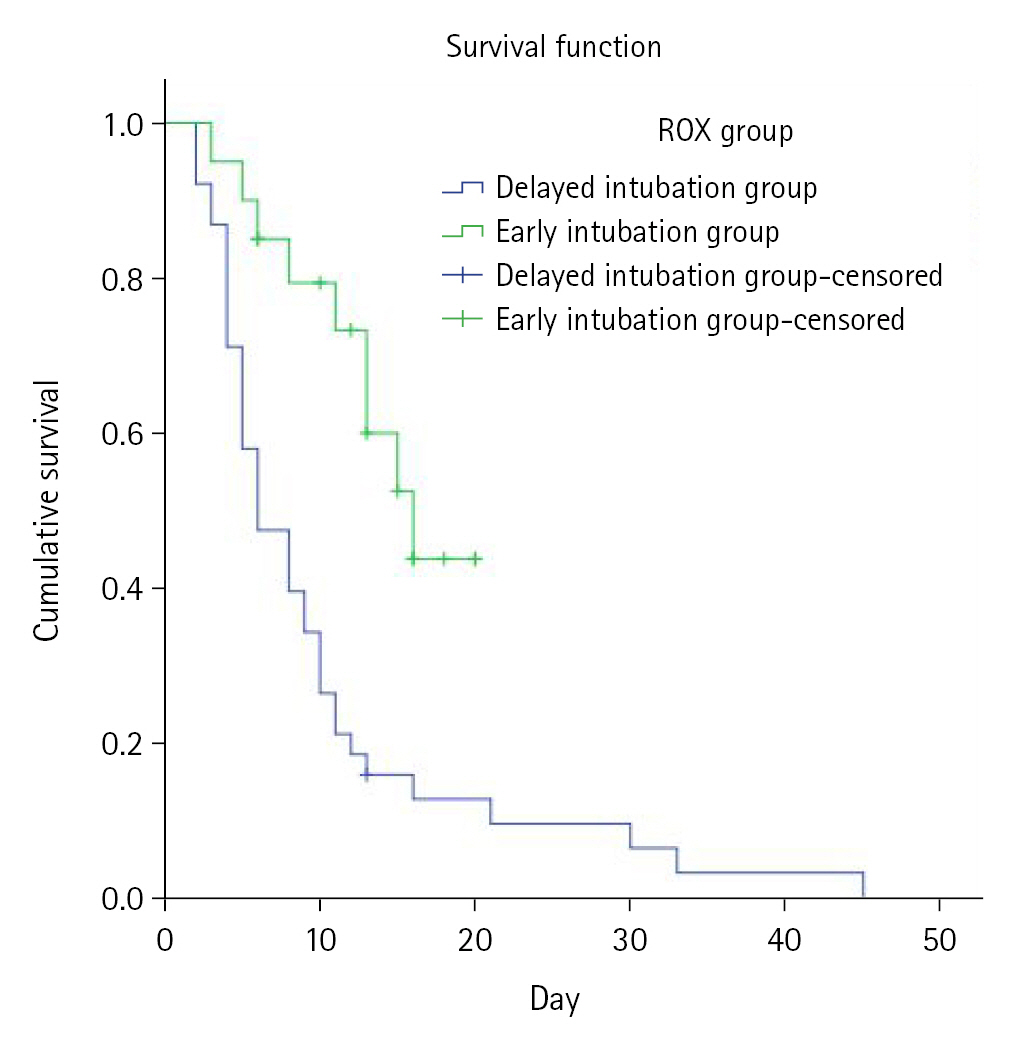
Table 1.Clinical characteristics of COVID-19 patients who required mechanical ventilation
|
Parameter |
Total (n=58) |
Time from ROX <4.88 to intubation
|
P-value |
|
<12 hr (n=20) |
≥12 hr (n=38) |
|
Age (yr) |
57±14 |
55±14 |
58±14 |
0.73 |
|
Male (%) |
55.0 |
55.0 |
55.3 |
0.98 |
|
DM (%) |
48.3 |
50.0 |
47.4 |
0.84 |
|
HTN (%) |
50.0 |
40.0 |
55.0 |
0.27 |
|
COPD (%) |
3.4 |
5.0 |
2.6 |
1.00 |
|
CKD (%) |
6.9 |
5.0 |
8.0 |
1.00 |
|
CAD |
13.8 |
15.0 |
13.0 |
1.00 |
|
Charlson Comorbidity Index |
2 (1–3) |
2 (1–3) |
2 (1–3) |
0.26 |
|
Day of intubation after confirmed COVID-19 infection |
9 (3–13) |
7 (4–12) |
9 (3–13) |
0.85 |
|
SOFA score at admission |
3 (2–4) |
3 (2–4) |
3 (2–4) |
0.51 |
|
SOFA score at intubation |
4 (4–5) |
4 (4–4) |
4 (4–5) |
0.33 |
|
APACHE II score at admission |
15.1±3.3 |
13.8±3.3 |
16.0±2.5 |
0.85 |
|
ROX index at initiation of HFNO |
5.4±1.9 |
5.3±2.3 |
5.0±1.4 |
0.57 |
Table 2.Comparison of main outcome variables between early and delayed intubation groups
|
Parameter |
Time from ROX <4.88 to intubation
|
P-value |
|
<12 hr (n=20) |
≥12 hr (n=38) |
|
Extubation (%) |
88.2 |
11.8 |
<0.001 |
|
Survival (%) |
91.7 |
8.3 |
<0.001 |
|
Shock (%) |
20.0 |
10.5 |
0.061 |
|
AKI (%) |
20.0 |
80.0 |
0.051 |
|
ICU day |
13 (7–16) |
6 (4–11) |
0.007 |
|
Hospital day |
18 (14–28) |
10 (5–14) |
0.001 |
Table 3.Predictors of extubation in mechanically ventilated COVID-19 patients
|
Variable |
Univariable model
|
Multivariable model
|
|
OR (95% CI) |
P-value |
OR (95% CI) |
P-value |
|
Age |
0.97 (0.93–1.02) |
0.30 |
0.93 (0.70–1.11) |
0.45 |
|
Male |
0.98 (0.32–3.01) |
0.97 |
0.32 (0.20–45.3) |
0.36 |
|
Day of intubation after confirmed COVID-19 infection |
0.96 (0.64–1.04) |
0.40 |
0.81 (0.64–1.04) |
0.11 |
|
Early intubation based on ROX index |
34.6 (6.59–182.71) |
0.00 |
690 (8.19–581) |
0.004 |
|
CAD |
0.33 (0.39–2.98) |
0.33 |
0.02 (0.00–4.69) |
0.16 |
|
HTN |
0.47 (0.15–1.51) |
0.20 |
2.32 (0.14–37.8) |
0.55 |
|
DM |
0.37 (0.30–2.84) |
0.00 |
0.15 (0.00–3.55) |
0.24 |
|
AKI |
0.48 (0.13–1.74) |
0.27 |
0.65 (0.04–9.90) |
0.75 |
|
Charlson Comorbidity Index |
0.77 (0.27–1.18) |
0.24 |
1.67 (0.27–10.30) |
0.57 |
|
APACHE II score at admission |
0.52 (0.56–1.05) |
0.34 |
0.82 (0.56–1.05) |
0.21 |
|
SOFA score at admission |
0.92 (0.66–1.56) |
0.69 |
4.13 (0.66–25.80) |
0.13 |
|
SOFA score at intubation |
0.29 (0.40–2.85) |
0.49 |
0.29 (0.30–2.85) |
0.29 |
References
- 1. Varikasuvu SR, Varshney S, Dutt N, Munikumar M, Asfahan S, Kulkarni PP, et al. D-dimer, disease severity, and deaths (3D-study) in patients with COVID-19: a systematic review and meta-analysis of 100 studies. Sci Rep 2021;11:21888. ArticlePubMedPMCPDF
- 2. Meng L, Qiu H, Wan L, Ai Y, Xue Z, Guo Q, et al. Intubation and ventilation amid the COVID-19 outbreak: Wuhan's experience. Anesthesiology 2020;132:1317-32.PubMed
- 3. Tobin MJ, Laghi F, Jubran A. Caution about early intubation and mechanical ventilation in COVID-19. Ann Intensive Care 2020;10:78. ArticlePubMedPMCPDF
- 4. Kang BJ, Koh Y, Lim CM, Huh JW, Baek S, Han M, et al. Failure of high-flow nasal cannula therapy may delay intubation and increase mortality. Intensive Care Med 2015;41:623-32.ArticlePubMedPDF
- 5. Roca O, Caralt B, Messika J, Samper M, Sztrymf B, Hernández G, et al. An index combining respiratory rate and oxygenation to predict outcome of nasal high-flow therapy. Am J Respir Crit Care Med 2019;199:1368-76.ArticlePubMed
- 6. Patel BK, Wolfe KS, Pohlman AS, Hall JB, Kress JP. Effect of noninvasive ventilation delivered by helmet vs face mask on the rate of endotracheal intubation in patients with acute respiratory distress syndrome: a randomized clinical trial. JAMA 2016;315:2435-41.ArticlePubMedPMC
- 7. Suliman LA, Abdelgawad TT, Farrag NS, Abdelwahab HW. Validity of ROX index in prediction of risk of intubation in patients with COVID-19 pneumonia. Adv Respir Med 2021;89:1-7.ArticlePubMed
- 8. Kim JH, Baek AR, Lee SI, Kim WY, Na YS, Lee BY, et al. ROX index and SpO2/FiO2 ratio for predicting high-flow nasal cannula failure in hypoxemic COVID-19 patients: a multicenter retrospective study. PLoS One 2022;17:e0268431.ArticlePubMedPMC
- 9. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 2008;61:344-9.ArticlePubMed
- 10. Zirpe KG, Tiwari AM, Gurav SK, Deshmukh AM, Suryawanshi PB, Wankhede PP, et al. Timing of invasive mechanical ventilation and mortality among patients with severe COVID-19-associated acute respiratory distress syndrome. Indian J Crit Care Med 2021;25:493-8.ArticlePubMedPMC
- 11. Wunsch H. Mechanical ventilation in COVID-19: interpreting the current epidemiology. Am J Respir Crit Care Med 2020;202:1-4.ArticlePubMedPMC
- 12. Wang Y, Lu X, Li Y, Chen H, Chen T, Su N, et al. Clinical course and outcomes of 344 intensive care patients with COVID-19. Am J Respir Crit Care Med 2020;201:1430-4.ArticlePubMedPMC
- 13. Pfortmueller CA, Spinetti T, Urman RD, Luedi MM, Schefold JC. COVID-19-associated acute respiratory distress syndrome (CARDS): current knowledge on pathophysiology and ICU treatment. A narrative review. Best Pract Res Clin Anaesthesiol 2021;35:351-68.ArticlePubMed
- 14. Wang Z, Deng H, Ou C, Liang J, Wang Y, Jiang M, et al. Clinical symptoms, comorbidities and complications in severe and non-severe patients with COVID-19: a systematic review and meta-analysis without cases duplication. Medicine (Baltimore) 2020;99:e23327.PubMedPMC
- 15. Song SE, Lee SH, Jo EJ, Eom JS, Mok JH, Kim MH, et al. The prognostic value of the Charlson's comorbidity index in patients with prolonged acute mechanical ventilation: a single center experience. Tuberc Respir Dis (Seoul) 2016;79:289-94.ArticlePubMedPMCPDF
- 16. Ferreira FL, Bota DP, Bross A, Mélot C, Vincent JL. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA 2001;286:1754-8.ArticlePubMed
- 17. Fuchs PA, Czech IJ, Krzych ŁJ. Mortality prediction using SOFA score in critically ill surgical and non-surgical patients: which parameter is the most valuable? Medicina (Kaunas) 2020;56:273. ArticlePubMedPMC
- 18. Raschke RA, Agarwal S, Rangan P, Heise CW, Curry SC. Discriminant accuracy of the SOFA score for determining the probable mortality of patients with COVID-19 pneumonia requiring mechanical ventilation. JAMA 2021;325:1469-70.ArticlePubMedPMC
- 19. Gianstefani A, Farina G, Salvatore V, Alvau F, Artesiani ML, Bonfatti S, et al. Role of ROX index in the first assessment of COVID-19 patients in the emergency department. Intern Emerg Med 2021;16:1959-65.ArticlePubMedPMCPDF
- 20. Patel M, Chowdhury J, Mills N, Marron R, Gangemi A, Dorey-Stein Z, et al. Utility of the ROX index in predicting intubation for patients with COVID-19-related hypoxemic respiratory failure receiving high-flow nasal therapy: retrospective cohort study. JMIRx Med 2021;2:e29062.ArticlePubMedPMC
- 21. Hyman JB, Leibner ES, Tandon P, Egorova NN, Bassily-Marcus A, Kohli-Seth R, et al. Timing of intubation and in-hospital mortality in patients with coronavirus disease 2019. Crit Care Explor 2020;2:e0254.ArticlePubMedPMC
- 22. Papoutsi E, Giannakoulis VG, Xourgia E, Routsi C, Kotanidou A, Siempos II. Effect of timing of intubation on clinical outcomes of critically ill patients with COVID-19: a systematic review and meta-analysis of non-randomized cohort studies. Crit Care 2021;25:121. ArticlePubMedPMCPDF
- 23. Weaver L, Das A, Saffaran S, Yehya N, Scott TE, Chikhani M, et al. High risk of patient self-inflicted lung injury in COVID-19 with frequently encountered spontaneous breathing patterns: a computational modelling study. Ann Intensive Care 2021;11:109. ArticlePubMedPMCPDF
- 24. Chaddha U, Kaul V, Agrawal A. What is the true mortality in the critically ill patients with COVID-19? Indian J Crit Care Med 2020;24:383-4.ArticlePubMedPMC
- 25. Nath R, Gupta NK, Jaswal A, Gupta S, Kaur N, Kohli S, et al. Mortality among adult hospitalized patients during the first wave and second wave of COVID-19 pandemic at a tertiary care center in India. Monaldi Arch Chest Dis 2021;92.ArticlePDF
Citations
Citations to this article as recorded by


 , Sam Philip1
, Sam Philip1

 PubReader
PubReader ePub Link
ePub Link Cite
Cite


