Abstract
-
Background:
- We compared the clinical outcomes of cardiac valve surgery in adult Jehovah’s Witness patients refusing blood transfusion to those in non-Jehovah’s Witness patients without any transfusion limitations.
-
Methods:
- From 2005 to 2014, 25 Jehovah’s Witnesses (JW group) underwent cardiac valve surgery using a blood conservation strategy. Twenty-five matched control patients (non-JW group) were selected according to sex, age, operation date, and surgeon. Both groups were managed according to general guidelines of anticoagulation for valve surgery.
-
Results:
- The operative mortality rate was 4.0% in the JW group and 0% in the non-JW group (p = 1.000). There was no difference in postoperative major complications between the groups (p = 1.000). The overall survival rate at 5 and 10 years was 85.6% ± 7.9% and 85.6% ± 7.9% in the JW group, respectively, and 100.0% ± 0.0% and 66.7% ± 27.2% in the non-JW group (p = 0.313). The valve-related morbidity-free survival rates (p = 0.625) and late morbidity-free survival rates (p = 0.885) were not significantly different between the groups.
-
Conclusions:
- Using a perioperative strategy for blood conservation, cardiac valve surgery without transfusion had comparable clinical outcomes in adult patients. This blood conservation strategy could be broadly applied to major surgeries with careful perioperative care.
-
Keywords: blood; heart valves; Jehovah’s witness; open heart surgery; perioperative care; transfusion
Introduction
Cardiac valve surgery is considered a major surgery with a high chance of hemorrhage and extracorporeal circulation dilution. Members of Jehovah’s Witnesses (JW), a Christian denomination, refuse blood transfusions based on religious beliefs.[1,2] Therefore, cardiac surgery, which is often accompanied by massive bleeding, can be challenging in these patients and requires alternative operative techniques and perioperative management.
Since the early 2000s, our institution has applied a comprehensive multimodality program for the refusal of blood transfusion in JW undergoing open heart surgery. This blood conservation strategy without transfusion has been set and modified based on previous studies.[3-5] Our strategy comprises four phases, with two objectives in each phase.
Using similar specialized programs, prior studies have reported excellent outcomes of cardiac surgery in JW.[6-12] However, most included various types of open heart surgeries.[13-16]
Comparative studies of perioperative and long-term results following cardiac valve operations are lacking. Therefore, we focused on the clinical outcomes of JW after cardiac valve procedures and compared these results to those of non-JW patients who underwent cardiac valve operation without any transfusion limitations.
Materials and Methods
1) Study population
We reviewed our database of 94 JW patients undergoing cardiac surgery from July 1, 2005 to December 31, 2014. We excluded cases of off-pump coronary bypass surgery (n = 18), patients younger than 19 years (n = 22), and repeat operations (n = 4), resulting in the inclusion of 50 adult patients who underwent initial open heart surgery using cardiopulmonary bypass (CPB). Finally, patients who did not undergo cardiac valve surgery were excluded (coronary bypass surgery, n = 11; atrial septal defect repair, n = 4; ventricular septal defect repair, n = 3; myxoma resection, n = 3; other, n = 4), leaving a final population of 25 JW patients (JW group). Among patients who were not JW and underwent cardiac valve surgery during the same period, 41 were selected according to sex, age (± 1 year), date of surgery (± 1 year), and operating surgeon. Of those, 25 patients (non-JW group) were selected by one-to-one matching with each patient of the JW group.
The preoperative and operative data in the JW and non-JW groups are described in Table 1. A specific protocol was used in the management of JW patients, while the control group received blood transfusions as needed without any restrictions. In the non-JW group, the perioperative transfusion rate was 88.0% (n = 22). The blood conservation strategy at our center, which contains four phases and two objectives in each phase, is briefly summarized in Table 2. This study was reviewed and approved by the Institutional Review Board of our center. Individual patient consent was waived.
2) Blood conservation strategy
During the study period, patients were managed according to standardized clinical protocols, as described below. Anesthetic and surgical techniques were standardized for all patients.
In the JW group, alcohol consumption and medications or supplements that can increase the risk of bleeding (e.g., celecoxib, vitamin E, ginkgo supplements, garlic) were discontinued before the operation. Erythropoietin (500 units/kg per day, every-other-day) was subcutaneously injected, as indicated, toward a goal hemoglobin level of 13 g/dL (male) or 12 g/dL (female). Components of iron, folate, calcium, and vitamin C were supplied. Aspirin (three to five days before operation) and clopidogrel (seven days before operation) were withheld in all patients. The international normalized ratio (INR) was normalized and converted to unfractionated heparin in patients receiving warfarin. Heparin infusion was adjusted to maintain an activated partial thromboplastin time of 50-70 seconds.
In some cases in each group, acute normovolemic hemodilution was performed (5-8 mL/kg).[17] The inclusion criterion was a hemoglobin level higher than 13 g/dL in males and 12 g/dL in females. After anesthetic induction, venous blood was drained into a collecting bag through a central venous line, and the same volume of colloid solution was replaced through another venous line. Blood in the collecting bag was stored at room temperature during the operation and then re-transfused after protamine administration.
All patients underwent the operation under moderate hypothermia (32°C) and alpha-stat pH management. The components of the CPB circuits were identical for both groups. A centrifugal pump with a hollow-fiber oxygenator and polymethylpentene-coated CPB circuits (Capiox, Terumo, Tokyo, Japan) were used in all cases. An initial dose of heparin (300 units/kg) was administered to achieve and maintain an activated clotting time (ACT) longer than 480 seconds. The ACT was measured every hour during CPB. In both groups, heparin and protamine administrations were monitored by a dose-response assay.
We conducted a retrograde autologous priming (RAP) technique in the JW group, using a modified protocol based on previous studies.[18,19] The CPB circuits were primed with 1,700 mL of crystalloid solution. Before the initiation of bypass, some of the prime volume was slowly removed from the reservoir and venous line. The crystalloid solution in the CPB circuit was slowly substituted for the patient’s blood by retrograde filling. The volume in the venous side of the circuit was drained, followed by that in the arterial side. The drainage was stopped when the patient’s systolic blood pressure decreased to less than 90 mmHg. With this technique, we were able to reduce the crystalloid prime volume to an average of 700 mL. As a result, about 1,000 mL of crystalloid solution could be removed.
Myocardial protection was achieved with cold antegrade crystalloid cardioplegia (HTK solution, Alsbach-Hähnlein, Germany) or cold retrograde blood cardioplegia (1:4), according to surgeon preference, supplemented by topical cooling with cold saline solution. Field blood was aspirated into a cardiotomy pump sucker during CPB and into a cell saving device (autoLog Autotransfusion System, Medtronic, Minneapolis, MN, USA) before and after CPB. Field blood collected in the suckers was not discarded. All sponges were wrung into a bowel, and the drainage was directed to a cell saving device.
Modified ultrahemofiltration during CPB was used to concentrate blood whenever feasible. After separation from CPB, heparin was neutralized with protamine sulfate, 1 mg per 100 units of heparin, to achieve an ACT within 10% of the baseline. In the JW group, after the operation and during the intensive care unit stay, shed mediastinal and pleural blood was collected into a reservoir and reinfused using a cell saving device. Antifibrinolytic drugs such as tranexamic acid or aprotinin were used prophylactically, depending on bleeding risk. Aprotinin was last used in October 2007. After the operation, patients were transferred to the intensive care unit and managed according to protocol.
3) Anticoagulation
The JW patients were subject to the same general guidelines of anticoagulation for prosthetic cardiac valve as were the non-JW patients. We recommended a biologic valve in patients older than 65 years or those with contraindication to anticoagulation. In contrast, patients younger than 65 years were advised to choose a mechanical valve. In cases using mechanical valves, warfarin treatment was started with a target range of prothrombin time INR of 2.0 to 3.0. In patients with atrial fibrillation and a history of thromboembolic event, INR was maintained between 2.5 and 3.5 with warfarin. Patients with biological valves were advised to take warfarin for the first three months and then were discharged for the follow-up period.
4) Data definitions
The primary outcomes of this study were perioperative mortality and morbidity. For this analysis, operative mortality was defined as death during the hospitalization period after surgery or after discharge but within 30 days of surgery. Major postoperative complications included myocardial infarction; intra-aortic balloon pump usage; moderate to severe left ventricular dysfunction (ejection fraction less than 40%); new onset of supraventricular arrhythmia; permanent stroke; reoperation for any reason including bleeding control, sternal wound infection including mediastinitis, renal insufficiency, or renal failure requiring dialysis or hemofiltration; and pneumonia. Renal insufficiency was defined as a serum creatinine level higher than 2.0 mg/dL or an increase to at least 2.0 times the preoperative baseline concentration. Late morbidity and mortality were defined by the “Guidelines for reporting morbidity and mortality after cardiac valvular operations.”[20] In addition, new onset of congestive heart failure or supraventricular arrhythmia requiring medical or surgical treatment was defined as late morbidity.
5) Follow-up
Clinical follow-up data were collected from our database through retrospective review of medical records. Follow-up information was obtained by telephone interviews of patients or their relatives and through the national medical insurance database. The mean duration of follow-up was 70.6 ± 38.8 and 76.5 ± 34.2 months in the JW group and the non-JW group, respectively (p = 0.576), and 98.0% (n = 49) of surviving patients completed the follow-up. Overall survival was measured from the date of surgery to the date of death or of the last contact while the patient was alive. Event-free survival was measured from the date of surgery to the date of the first event or the last contact while the patient was alive.
6) Statistical analysis
Descriptive statistics were calculated using the mean ± standard deviation for continuous variables and number and percentage for categorical variables. Differences between groups for continuous and categorical variables were calculated using Student’s t-test and Fisher’s exact test, respectively. Results with p-values less than 0.05 were considered statistically significant. Long-term survival and event-free survival were analyzed using the Kaplan-Meier method. A log-rank test was used to compare the survival curves between groups. The SPSS Statistical software 20.0 program (SPSS, Chicago, IL, USA) was used for statistical analyses.
Results
1) Operative outcomes
The operative mortality rate was 4.0% (one patient) in the JW group, and there were no operative deaths in the non-JW group (p = 1.000). The cause of operative death in the JW group was right ventricular (RV) failure. RV failure and concomitant mediastinal hematoma collection were postoperatively detected by echocardiography. Hemodynamic status temporally improved after emergency explo-thoracotomy. However, no right ventricular assistance device could easily be applied at that time. Because the patient’s hemoglobin level was 8.4 g/dL and the platelet count was 30,000/mm3, mechanical circulatory support could not be performed without blood transfusion due to the high bleeding risk.
Major postoperative complications occurred in seven patients in each group (p = 1.000) (Table 3). There were no bleeding events in the JW group. In the two cases of sternal wound infection in the JW group, additional wound repair was successfully achieved without blood transfusion.
2) Long-term outcomes
Overall, there were four late deaths during the follow-up period, including three in the JW group and one in the non-JW group. The causes of death in the JW group were intracranial hemorrhage (n = 1), cardiogenic shock during percutaneous coronary intervention (n = 1), and unknown (n = 1). In the non-JW group, one patient died due to acute heart failure soon after aortic surgery, which was performed nine years after valve surgery. The late morbidities in both groups are summarized in Table 3.
There were no significant differences in overall survival, valve-related morbidity, or late morbidity between the two groups. The actuarial rates of overall survival at 1, 5, and 10 years were 95.8% ± 4.1%, 85.6% ± 7.9%, and 85.6% ± 7.9% in the JW group, respectively, and 100.0% ± 0.0%, 100.0% ± 0.0%, and 66.7% ± 27.2% in the non-JW group (log-rank, p = 0.313) (Fig. 1). The actuarial valve-related morbidity-free survival rates at 1, 2, and 5 years were 85.7% ± 6.8%, 85.7% ± 6.8%, and 81.3% ± 8.7% in the JW group, respectively, and 96.0% ± 3.9%, 91.6% ± 5.7%, and 86.5% ± 7.3% in the non-JW group (log-rank, p = 0.625) (Fig. 2). The actuarial late morbidity-free survival rates at 1, 2, and 5 years were 91.7% ± 5.6%, 83.3% ± 7.6%, and 76.9% ± 9.3% in the JW group, respectively, and 96.0% ± 3.9%, 87.6% ± 6.7%, and 77.8% ± 8.9% in the non-JW group (log-rank, p = 0.885) (Fig. 3).
3) Hematologic data
There were no significant differences in preoperative, intraoperative, or postoperative hematologic values between the JW group and the non-JW group (Table 4). In addition, the decreased levels of hemoglobin and hematocrit were within the acceptable ranges for both groups. Creatinine level as an indicator of renal injury was not statistically significant between the groups.
Discussion
A major finding of this study was that cardiac valve surgery using a blood conservation strategy without transfusion for Jehovah’s Witnesses had similar perioperative results compared to those in non-Jehovah’s Witnesses undergoing a strategy involving transfusion. In addition, long-term clinical outcomes for Jehovah’s Witnesses were satisfactory without any modifications to the general anticoagulation guidelines for the management of a prosthetic cardiac valve.
Rosengart et al.[3] introduced a multimodality blood conservation program that included technical and pharmacologic measures. Their algorithmic application of the multimodality program was divided into preoperative, intraoperative, and postoperative periods. Using their protocol, there were no significant differences in the operative results of Jehovah’s Witnesses compared with those of non-Jehovah’s Witnesses. However, their comparative study did not include cardiac valve surgery. Although others have compared the clinical outcomes between Jehovah’s Witnesses and control groups, their reports did not dictate the exact proportion of valve procedures among the total population.[13,14] In recent comparative studies, cardiac valve surgery comprised only one-quarter or one-half of the total population.[15,16] In a report by Pattakos et al.,[16] about 8% of the total cohort did not undergo cardiopulmonary bypass Our study included only cases of cardiac valve surgery using cardiopulmonary bypass, distinguishing it from other studies.
In the 1970s, Ott and Cooley[21] reported the results of cardiovascular surgery in 542 Jehovah’s Witnesses patients. Among these patients, the early mortality rate of the 362 patients requiring cardiopulmonary bypass was 10.7%. However, among 126 patients who underwent valve operation, the early mortality rate was 13.5%. Cardiac valve operation accompanied by a relatively long cardiotomy is considered different than coronary artery bypass surgery. Direct incision in the cardiac chamber can increase the chance of postoperative bleeding. Also, valvular heart disease has different clinical and hemodynamic features from coronary artery disease. In addition, a heterogeneous study population can inevitably cause bias. We tried to focus on cardiac valve surgery, for which it is imperative to open the cardiac chamber, unlike coronary artery bypass surgery. For direct comparison without unnecessary bias, a total of 25 matched patients (non-JW group) were randomly selected from our database according to sex, age (± 1 year), date of surgery (± 1 year), and operating surgeon.
Extracorporeal hemodilution is common with the use of a CPB circuit and can be associated with adverse outcomes. [22,23] The RAP technique has been used to reduce the degree of hemodilution during CPB. Since the early 2000s, we have routinely performed this technique in Jehovah’s Witnesses in order to reduce the CPB prime volume.[18,19] Rosengart et al.[19] withdrew about 900 mL from 1,400 mL of initial prime, leaving about 500 mL in volume. With our technique, up to 700 mL of prime volume can be removed. Although the remaining prime volume was larger than in the previous study, the lowest hematocrit value during CPB in our study was 23.1% ± 2.3%. This was satisfactory and in good agreement with previous results (22% ± 3%).
A low hematocrit value less than 22% during CPB significantly increased the risk of stroke, myocardial infarction, low cardiac output, cardiac arrest, renal failure, prolonged ventilation, pulmonary edema, etc.[22] In contrast, moderate hemodilution (21-25%) during CPB was not significantly correlated with acute renal failure requiring dialysis. [24,25] The lowest hematocrit values in our study were 23.3% in the JW group and 22.8% in the non-JW group (Table 4). These results are within a safe range to prevent adverse clinical outcomes. Even though the intraoperative transfusion rate in the non-JW group was 88.0% (n = 22), it is worth noting that the lowest hematocrit values in the JW group was similar to that of the non-JW group (p = 0.511). Our findings verified that the RAP technique is an effective method to reduce extracorporeal hemodilution and is helpful in decreasing perioperative adverse outcomes.
Our study has some inherent limitations as it is a retrospective review performed in a single medical institution. The clinical outcomes of our study had low statistical power due to the small number of patients and events. However, we were able to obtain meaningful results with respect to postoperative outcomes by performing statistical analysis. Although we have successfully implemented this blood conservation strategy without transfusion in the management of Jehovah’s Witnesses, this program has not been extended to the general population undergoing cardiac operations in our institution, because this approach would require the alteration of general perioperative processes and lead to higher costs for pharmacologic agents and appropriate instruments. Our institution does not have strict or specific guidelines for blood transfusion, but we consider blood transfusion in cases where the hemoglobin level is lower than 10 g/dL. We are not concerned about the amount of postoperative chest tube drainage. In this retrospective study, it was difficult to quantify the amount of postoperative bleeding because mediastinal and pleural blood being shed was reinfused using a cell saving device (autoLog Autotransfusion System, Medtronic, Minneapolis, MN, USA). Also, it was impossible for us to evaluate the sanguinity of this blood. Thus, we excluded this variable in the statistical analysis. We last used the drug aprotinin in October 2007, but the effect of this drug was not considered in this study.
In conclusion, the importance of our study is that cardiac valve surgery was performed safely without blood transfusion by applying an optimal blood conservation strategy. More generalized application of these measures might allow for increased “transfusion-free” operations in the general population. However, more definitive and reliable evidence should be provided by well-designed trials including other major operations and a larger population.
NOTES
-
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank our consultant statistician, Hyonggin Ann, Ph.D., for biostatistical advice on this study.
Fig. 1.Actuarial overall survival in the JW and non-JW groups (log-rank, p = 0.313). JW: Jehovah’s Witness.

Fig. 2.Actuarial valve-related morbidity-free survival in the JW and non-JW groups (log-rank, p = 0.625). JW: Jehovah’s Witness.

Fig. 3.Actuarial late morbidity-free survival in the JW and non-JW groups (log-rank, p = 0.885). JW: Jehovah’s Witness.
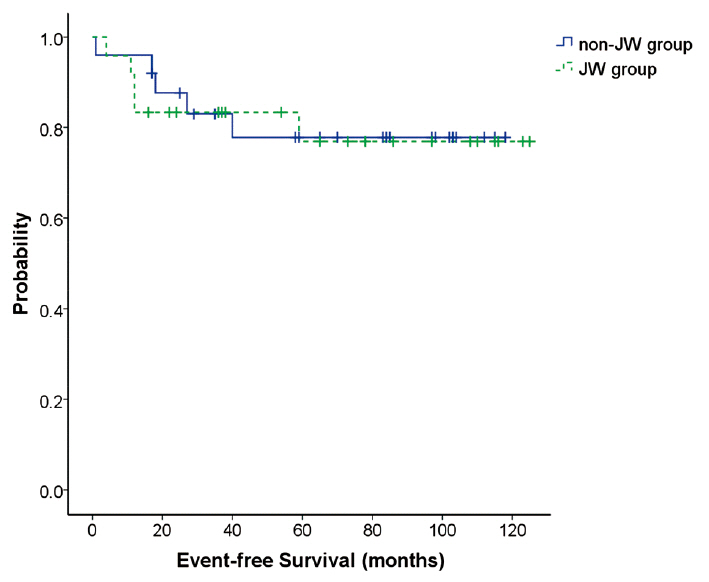
Table 1.Preoperative and operative data
|
Variables |
JW group (n = 25) |
non-JW group (n = 25) |
p*
|
|
Age (years) |
54.0 ± 11.5 |
54.1 ± 11.5 |
0.993 |
|
Female |
18 (72.0%) |
18 (72.0%) |
1.000 |
|
NYHA functional class |
2.6 ± 0.8 |
2.6 ± 0.6 |
1.000 |
|
DM |
2 (8.0%) |
2 (8.0%) |
1.000 |
|
Hypertension |
5 (20.0%) |
5 (20.0%) |
1.000 |
|
CVA |
1 (4.0%) |
2 (8.0%) |
1.000 |
|
Hyperlipidemia |
3 (12.0%) |
5 (20.0%) |
0.702 |
|
Peripheral artery disease |
1 (4.0%) |
0 (0.0%) |
1.000 |
|
Atrial fibrillation |
10 (40.0%) |
6 (24.0%) |
0.364 |
|
Preop EF (%) |
62.8 ± 7.9 |
59.4 ± 12.8 |
0.253 |
|
Operated valve |
|
|
|
|
Aortic |
11 (44.0%) |
15 (60.0%) |
0.396 |
|
Mitral |
17 (68.0%) |
16 (64.0%) |
1.000 |
|
Tricuspid |
10 (40.0%) |
4 (16.0%) |
0.114 |
|
Multiple valve surgery |
11 (44.0%) |
7 (28.0%) |
0.377 |
|
Valve replacement |
18 (72.0%) |
21 (84.0%) |
0.496 |
|
Mechanical valve |
15 (60.0%) |
16 (64.0%) |
1.000 |
|
Concomitant procedures |
9 (36.0%) |
7 (28.0%) |
0.762 |
|
Maze procedure |
8 |
17 |
|
|
Ascending aorta replacement |
1 |
1 |
|
|
ASD closure |
0 |
1 |
|
|
CPB time (min) |
133.3 ± 35.6 |
130.8 ± 34.1 |
0.799 |
|
ACC time (min) |
100.3 ± 30.0 |
96.3 ± 27.9 |
0.628 |
|
Acute normovolemic hemodilution |
6 (24.0%) |
3 (12.0%) |
0.463 |
|
Blood cardioplegia |
18 (72.0%) |
19 (76.0%) |
1.000 |
|
Emergency or urgency |
1 (4.0%) |
0 (0.0%) |
1.000 |
|
Perioperative transfusion |
0 (0.0%) |
22 (88.0%) |
< 0.000 |
Table 2.Blood conservation strategy for adult Jehovah’s witnesses
|
Phase |
Objective |
Contents |
|
Preoperative |
Maintenance |
Discontinue intake of alcohol, and medications or supplements that may increase bleeding risk |
|
|
Withdrawal of aspirin (3 to 5 days before operation) and clopidogrel (7 days before operation) |
|
|
Conversion warfarin to unfractionated heparin |
|
|
Reduced laboratory sampling |
|
Reinforcement |
Subcutaneous erythropoietin (500 units/kg per day, every-other-day) as indicated, toward goal hemoglobin of 13 g/dL (male) or 12 g/dL (female) |
|
|
Supplement of iron, folate, calcium, vitamin C |
|
Intraoperative |
Maintenance |
Hyperoxic ventilation |
|
|
Hypotensive anesthesia |
|
|
Low-volume acute normovolemic hemodilution; volume target to Hb 10 g/dL and simultaneous replacement of same volume colloid solution |
|
|
Hemostatic operative technique |
|
|
Reduced laboratory sampling |
|
Reinforcement |
Cell salvage and re-transfusion using a cell saving device |
|
CPB |
Maintenance |
Minimum volume in cardiopulmonary bypass circuit |
|
|
Retrograde autologous priming |
|
Reinforcement |
Modified ultrahemofiltration |
|
Postoperative |
Maintenance |
Anticoagulants including tranexamic acid |
|
|
Reduced laboratory sampling |
|
Reinforcement |
Shed mediastinal and pleural blood reinfusion using a cell saving device |
|
|
Preoperative drugs re-use (erythropoietin, iron, folate, calcium, vitamin C) |
Table 3.Perioperative and late outcomes
|
Variables |
JW group (n = 25) |
non-JW group (n = 25) |
p*
|
|
Operative death |
1 (4.0%) |
0 (0.0%) |
1.000 |
|
Postoperative complications |
7 (28.0%) |
7 (28.0%) |
1.000 |
|
LV dysfunction |
2 |
2 |
|
|
RV failure |
1 |
0 |
|
|
IABP support |
0 |
2 |
|
|
Arrhythmia |
1 |
2 |
|
|
Renal failure or insufficiency |
3 |
1 |
|
|
Sternal wound infection |
2 |
1 |
|
|
Re-sternotomy bleeding control |
0 |
1 |
|
|
Gastrointestinal bleeding |
0 |
1 |
|
|
Postop length of stay (days) |
20.2 ± 13.3 |
16.7 ± 6.5 |
0.252 |
|
Postop EF (%) |
56.6 ± 10.9 |
56.1 ± 11.5 |
0.866 |
|
(pre–post) difference of EF (%) |
6.2 ± 11.0 |
3.3 ± 9.1 |
0.309 |
|
Late mortality |
3 |
1 |
0.313 |
|
Late morbidity |
5 |
5 |
0.885 |
|
Bleeding |
1 |
2 |
|
|
Embolism |
1 |
1 |
|
|
Reintervention |
2 |
0 |
|
|
Congestive heart failure |
1 |
2 |
|
|
Arrhythmia |
0 |
2 |
|
|
Late valve-related morbidity |
4 |
3 |
0.625 |
Table 4.Hematologic data
|
Variables |
JW group (n = 25) |
non-JW group (n = 25) |
p*
|
|
Preop Hb (g/dL) |
13.0 ± 1.5 |
13.2 ± 1.4 |
0.705 |
|
Postop Hb (g/dL) |
11.7 ± 1.6 |
12.2 ± 1.7 |
0.273 |
|
(pre–post) difference of Hb (g/dL) |
1.3 ± 1.3 |
0.9 ± 1.9 |
0.414 |
|
Preop Hct (%) |
38.9 ± 3.9 |
39.0 ± 3.7 |
0.936 |
|
Lowest Hct during CPB (%) |
23.3 ± 2.5 |
22.8 ± 2.2 |
0.511 |
|
Postop Hct (%) |
35.2 ± 5.1 |
35.9 ± 4.7 |
0.639 |
|
(pre–post) difference of Hct (%) |
3.7 ± 4.0 |
3.1 ± 5.4 |
0.677 |
|
(pre–CPB) difference of Hct (%) |
15.6 ± 3.5 |
16.1 ± 3.3 |
0.584 |
|
Preop Cr (mg/dL) |
0.96 ± 0.30 |
0.88 ± 0.25 |
0.292 |
|
Postop Cr (mg/dL) |
1.23 ± 0.43 |
1.11 ± 0.38 |
0.289 |
|
(post–pre) difference of Cr (mg/dL) |
0.27 ± 0.28 |
0.22 ± 0.27 |
0.600 |
References
- 1. Goodnough LT, Shander A, Spence R. Bloodless medicine: clinical care without allogeneic blood transfusion. Transfusion 2003;43:668-76.ArticlePubMed
- 2. Jo KI, Shin JW, Choi TY, Park YJ, Youm W, Kim MJ. Eight-year experience of bloodless surgery at a tertiary care hospital in Korea. Transfusion 2013;53:948-54.ArticlePubMed
- 3. Rosengart TK, Helm RE, DeBois WJ, Garcia N, Krieger KH, Isom OW. Open heart operations without transfusion using a multimodality blood conservation strategy in 50 Jehovah’s Witness patients: implications for a “bloodless” surgical technique. J Am Coll Surg 1997;184:618-29.PubMed
- 4. Helm RE, Rosengart TK, Gomez M, Klemperer JD, DeBois WJ, Velasco F, et al. Comprehensive multimodality blood conservation: 100 consecutive CABG operations without transfusion. Ann Thorac Surg 1998;65:125-36.ArticlePubMed
- 5. Spahn DR, Casutt M. Eliminating blood transfusions: new aspects and perspectives. Anesthesiology 2000;93:242-55.ArticlePubMed
- 6. Juraszek A, Dziodzio T, Roedler S, Kral A, Hutschala D, Wolner E, et al. Results of open heart surgery in Jehovah’s Witnesses patients. J Cardiovasc Surg (Torino) 2009;50:247-50.PubMed
- 7. Pompei E, Tursi V, Guzzi G, Vendramin I, Ius F, Muzzi R, et al. Mid-term clinical outcomes in cardiac surgery of Jehovah’s witnesses. J Cardiovasc Med (Hagerstown) 2010;11:170-4.ArticlePubMed
- 8. Moraca RJ, Wanamaker KM, Bailey SH, McGregor WE, Benckart DH, Maher TD, et al. Strategies and outcomes of cardiac surgery in Jehovah’s Witnesses. J Card Surg 2011;26:135-43.ArticlePubMed
- 9. Emmert MY, Salzberg SP, Theusinger OM, Felix C, Plass A, Hoerstrup SP, et al. How good patient blood management leads to excellent outcomes in Jehovah’s witness patients undergoing cardiac surgery. Interact Cardiovasc Thorac Surg 2011;12:183-8.ArticlePubMed
- 10. Vaislic CD, Dalibon N, Ponzio O, Ba M, Jugan E, Lagneau F, et al. Outcomes in cardiac surgery in 500 consecutive Jehovah’s Witness patients: 21 year experience. J Cardiothorac Surg 2012;7:95. ArticlePubMedPMCPDF
- 11. Marshall L, Krampl C, Vrtik M, Haluska B, Griffin R, Mundy J, et al. Short term outcomes after cardiac surgery in a Jehovah’s Witness population: an institutional experience. Heart Lung Circ 2012;21:101-4.ArticlePubMed
- 12. Jassar AS, Ford PA, Haber HL, Isidro A, Swain JD, Bavaria JE, et al. Cardiac surgery in Jehovah’s Witness patients: ten-year experience. Ann Thorac Surg 2012;93:19-25.ArticlePubMed
- 13. Stamou SC, White T, Barnett S, Boyce SW, Corso PJ, Lefrak EA. Comparisons of cardiac surgery outcomes in Jehovah’s versus non-Jehovah’s Witnesses. Am J Cardiol 2006;98:1223-5.ArticlePubMed
- 14. Reyes G, Nuche JM, Sarraj A, Cobiella J, Orts M, Martin G, et al. Bloodless cardiac surgery in Jehovah’s witnesses: outcomes compared with a control group. Rev Esp Cardiol 2007;60:727-31.ArticlePubMed
- 15. Bhaskar B, Jack RK, Mullany D, Fraser J. Comparison of outcome in Jehovah’s Witness patients in cardiac surgery: an Australian experience. Heart Lung Circ 2010;19:655-9.ArticlePubMed
- 16. Pattakos G, Koch CG, Brizzio ME, Batizy LH, Sabik JF 3rd, Blackstone EH, et al. Outcome of patients who refuse transfusion after cardiac surgery: a natural experiment with severe blood conservation. Arch Intern Med 2012;172:1154-60.ArticlePubMed
- 17. Casati V, Speziali G, D’Alessandro C, Cianchi C, Antonietta Grasso M, Spagnolo S, et al. Intraoperative low-volume acute normovolemic hemodilution in adult open-heart surgery. Anesthesiology 2002;97:367-73.ArticlePubMed
- 18. Shapira OM, Aldea GS, Treanor PR, Chartrand RM, DeAndrade KM, Lazar HL, et al. Reduction of allogeneic blood transfusions after open heart operations by lowering cardiopulmonary bypass prime volume. Ann Thorac Surg 1998;65:724-30.ArticlePubMed
- 19. Rosengart TK, DeBois W, O’Hara M, Helm R, Gomez M, Lang SJ, et al. Retrograde autologous priming for cardiopulmonary bypass: a safe and effective means of decreasing hemodilution and transfusion requirements. J Thorac Cardiovasc Surg 1998;115:426-38.ArticlePubMed
- 20. Akins CW, Miller DC, Turina MI, Kouchoukos NT, Blackstone EH, Grunkemeier GL, et al. Guidelines for reporting mortality and morbidity after cardiac valve interventions. Eur J Cardiothorac Surg 2008;33:523-8.ArticlePubMed
- 21. Ott DA, Cooley DA. Cardiovascular surgery in Jehovah’s Witnesses. Report of 542 operations without blood transfusion. JAMA 1977;238:1256-8.ArticlePubMed
- 22. Habib RH, Zacharias A, Schwann TA, Riordan CJ, Durham SJ, Shah A. Adverse effects of low hematocrit during cardiopulmonary bypass in the adult: should current practice be changed. J Thorac Cardiovasc Surg 2003;125:1438-50.ArticlePubMed
- 23. Ranucci M, Conti D, Castelvecchio S, Menicanti L, Frigiola A, Ballotta A, et al. Hematocrit on cardiopulmonary bypass and outcome after coronary surgery in nontransfused patients. Ann Thorac Surg 2010;89:11-7.ArticlePubMed
- 24. Karkouti K, Beattie WS, Wijeysundera DN, Rao V, Chan C, Dattilo KM, et al. Hemodilution during cardiopulmonary bypass is an independent risk factor for acute renal failure in adult cardiac surgery. J Thorac Cardiovasc Surg 2005;129:391-400.ArticlePubMed
- 25. Habib RH, Zacharias A, Schwann TA, Riordan CJ, Engoren M, Durham SJ, et al. Role of hemodilutional anemia and transfusion during cardiopulmonary bypass in renal injury after coronary revascularization: implications on operative outcome. Crit Care Med 2005;33:1749-56.ArticlePubMed
Citations
Citations to this article as recorded by

- Optimising bloodless cardiovascular surgery for Jehovah’s Witnesses and beyond
Matti Jubouri, Fatemeh Hedayat, Sakina Abrar, Sophie L. Mellor, Louise J. Brown, Amer Harky
Coronary Artery Disease.2022; 33(1): 52. CrossRef - Outcomes of perioperative management in Jehovah's Witness patients undergoing surgeries with a risk of bleeding: a retrospective, single-center, observational study
Keum Young So, Sang Hun Kim
Medical Biological Science and Engineering.2022; 5(1): 6. CrossRef



 PubReader
PubReader ePub Link
ePub Link Cite
Cite



