Articles
- Page Path
- HOME > Acute Crit Care > Volume 35(4); 2020 > Article
-
Original Article
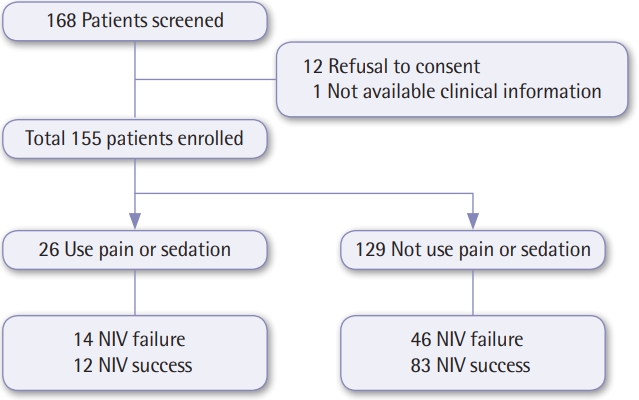
Pulmonary Utilization of pain and sedation therapy on noninvasive mechanical ventilation in Korean intensive care units: a multi-center prospective observational study -
Taehee Kim1
 , Jung Soo Kim2, Eun Young Choi3, Youjin Chang4, Won-Il Choi5, Jae-Joon Hwang6, Jae Young Moon7, Kwangha Lee8, Sei Won Kim9, Hyung Koo Kang10, Yun Su Sim1, Tai Sun Park11, Seung Yong Park12, Sunghoon Park13, Jae Hwa Cho14,
, Jung Soo Kim2, Eun Young Choi3, Youjin Chang4, Won-Il Choi5, Jae-Joon Hwang6, Jae Young Moon7, Kwangha Lee8, Sei Won Kim9, Hyung Koo Kang10, Yun Su Sim1, Tai Sun Park11, Seung Yong Park12, Sunghoon Park13, Jae Hwa Cho14, -
Acute and Critical Care 2020;35(4):255-262.
DOI: https://doi.org/10.4266/acc.2020.00164
Published online: November 9, 2020
1Department of Pulmonary, Allergy and Critical Care Medicine, Hallym University Kangnam Sacred Heart Hospital, Seoul, Korea
2Department of Pulmonary and Critical Care Medicine, Inha University College of Medicine, Incheon, Korea
3Department of Pulmonary and Critical Care Medicine, Yeungnam University Hospital, Daegu, Korea
4Department of Pulmonary and Critical Care Medicine, Inje University Sanggye Paik Hospital, Seoul, Korea
5Department of Internal Medicine, Myongji Hospital, Goyang, Korea
6Department of Pulmonary and Critical Care Medicine, Kyung Hee University Hospital at Gangdong, Seoul, Korea
7Department of Pulmonary and Critical Care Medicine, Chungnam National University Hospital, Daejeon, Korea
8Department of Internal Medicine, Pusan National University Hospital, Busan, Korea
9Department of Pulmonary, Critical Care and Sleep Medicine, St. Paul’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
10Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Inje University Ilsan Paik Hospital, Goyang, Korea
11Department of Internal Medicine, Hanyang University Guri Hospital, Guri, Korea
12Department of Pulmonary, Allergy and Critical Care Medicine, Jeonbuk National University Hospital, Jeonju, Korea
13Department of Pulmonary, Allergy and Critical Care Medicine, Hallym University Sacred Heart Hospital, Anyang, Korea
14Department of Internal Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
- Corresponding author Jae Hwa Cho Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, 211 Eonju-ro, Gangnam-gu, Seoul 06273, Korea Tel: +82-2-2019-3345 Fax: +82-2-3463-3882 E-mail: jhcho66@yuhs.ac
Copyright © 2020 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

Figure & Data
References
Citations
- Sedation and analgesia strategies for non-invasive mechanical ventilation: A systematic review and meta-analysis
Baolu Yang, Leyi Gao, Zhaohui Tong
Heart & Lung.2024; 63: 42. CrossRef - Effect of Music Therapy and Sound Isolation on the Comfort of Mechanically Ventilated Patients
Sinem Çalışkan, Esra Akın, Mehmet Uyar
Turkish Journal of Intensive Care.2024; 22(1): 83. CrossRef - 2021 KSCCM clinical practice guidelines for pain, agitation, delirium, immobility, and sleep disturbance in the intensive care unit
Yijun Seo, Hak-Jae Lee, Eun Jin Ha, Tae Sun Ha
Acute and Critical Care.2022; 37(1): 1. CrossRef - Comfort During Non-invasive Ventilation
Gianmaria Cammarota, Rachele Simonte, Edoardo De Robertis
Frontiers in Medicine.2022;[Epub] CrossRef - Current status of treatment of acute respiratory failure in Korea
Yong Jun Choi, Jae Hwa Cho
Journal of the Korean Medical Association.2022; 65(3): 124. CrossRef - Treatment of acute respiratory failure: noninvasive mechanical ventilation
Sunghoon Park
Journal of the Korean Medical Association.2022; 65(3): 144. CrossRef - Dexmedetomidine-Induced Aortic Contraction Involves Transactivation of the Epidermal Growth Factor Receptor in Rats
Soo Hee Lee, Seong-Chun Kwon, Seong-Ho Ok, Seung Hyun Ahn, Sung Il Bae, Ji-Yoon Kim, Yeran Hwang, Kyeong-Eon Park, Mingu Kim, Ju-Tae Sohn
International Journal of Molecular Sciences.2022; 23(8): 4320. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite