Articles
- Page Path
- HOME > Acute Crit Care > Volume 35(2); 2020 > Article
-
Review Article
Basic science and research Sepsis-induced cardiac dysfunction: a review of pathophysiology -
Reverien Habimana1
 , Insu Choi2, Hwa Jin Cho3, Dowan Kim4, Kyoseon Lee4, Inseok Jeong4
, Insu Choi2, Hwa Jin Cho3, Dowan Kim4, Kyoseon Lee4, Inseok Jeong4 -
Acute and Critical Care 2020;35(2):57-66.
DOI: https://doi.org/10.4266/acc.2020.00248
Published online: May 31, 2020
1Chonnam National University Graduate School, Gwangju, Korea
2Department of Pediatrics, Chonnam National University Children’s Hospital, Gwangju, Korea
3Department of Pediatrics, Chonnam National University Children’s Hospital and Medical School, Gwangju, Korea
4Department of Thoracic and Cardiovascular Surgery, Chonnam National University Hospital and Medical School, Gwangju, Korea
- Corresponding author Inseok Jeong Department of Thoracic and Cardiovascular Surgery, Chonnam National University Hospital and Medical School, 42 Jebong-ro, Dong-gu, Gwangju 61469, Korea Tel: +82-62-220-6456 Fax: +82-62-227-1636 E-mail: isjeong1201@gmail.com
- *These authors contributed equally to this work.
Copyright © 2020 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
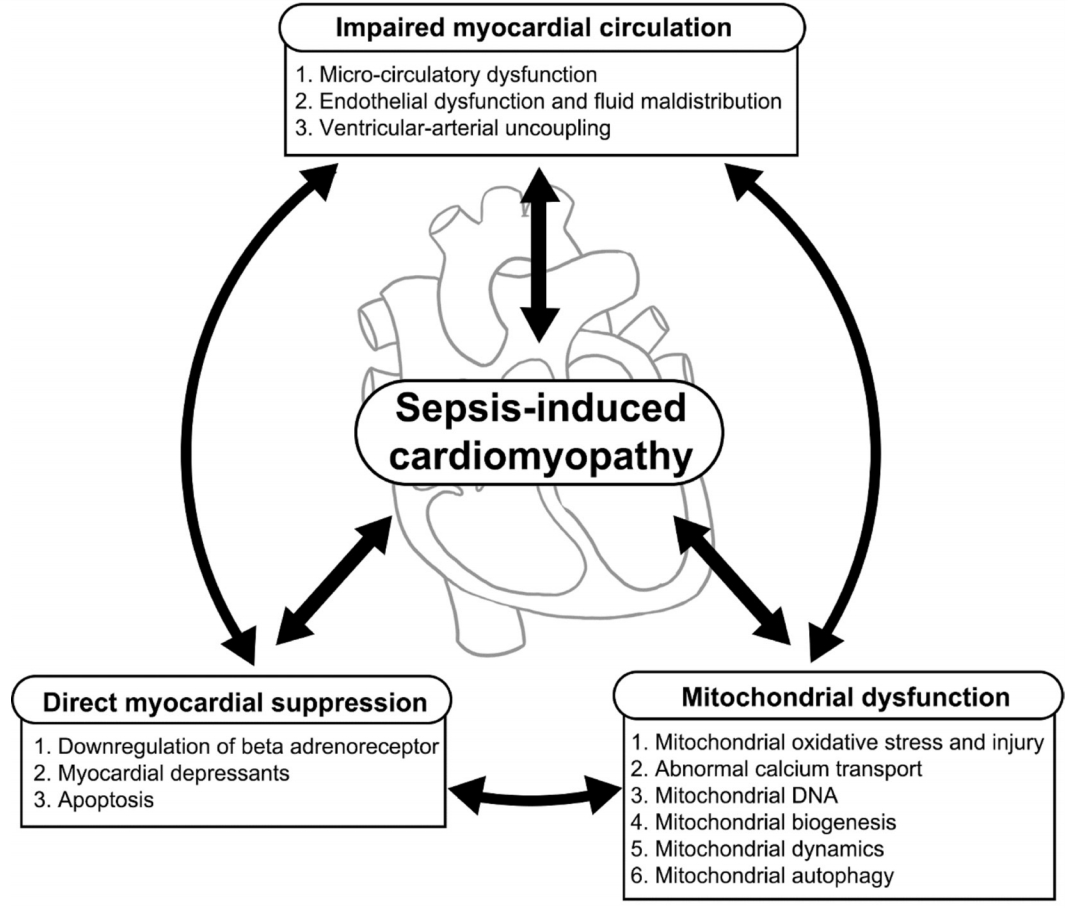
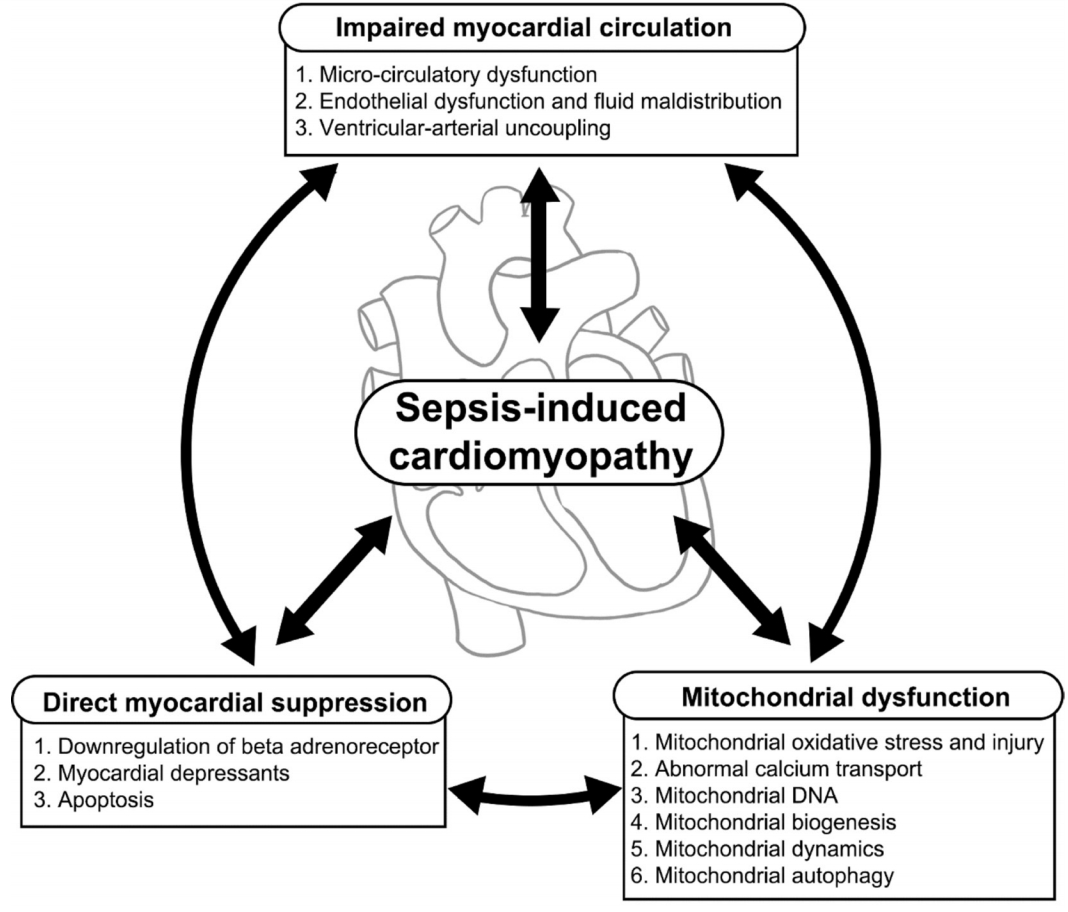
- It is well known that cardiac dysfunction in sepsis is associated with significantly increased mortality. The pathophysiology of sepsis-induced cardiac dysfunction can be summarized as involving impaired myocardial circulation, direct myocardial depression, and mitochondrial dysfunction. Impaired blood flow to the myocardium is associated with microvascular dysfunction, impaired endothelium, and ventriculo-arterial uncoupling. The mechanisms behind direct myocardial depression consist of downregulation of β-adrenoceptors and several myocardial suppressants (such as cytokine and nitric oxide). Recent research has highlighted that mitochondrial dysfunction, which results in energy depletion, is a major factor in sepsis-induced cardiac dysfunction. Therefore, the authors summarize the pathophysiological process of cardiac dysfunction in sepsis based on the results of recent studies.
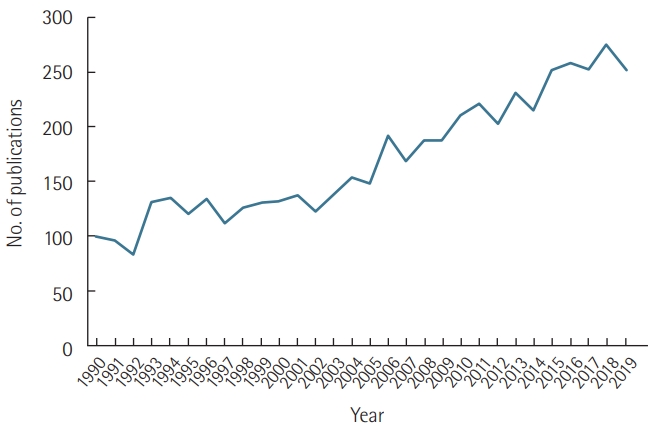
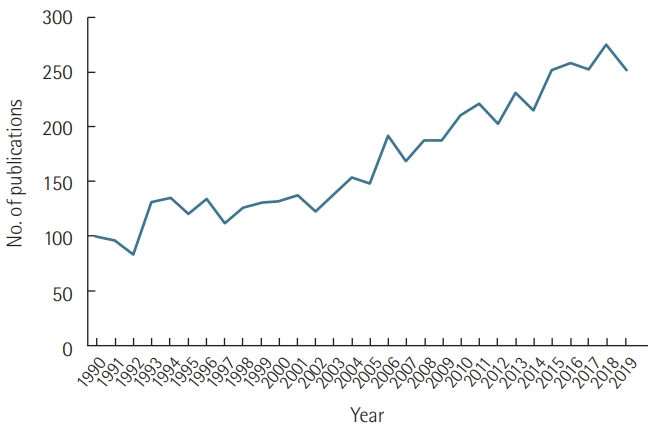
INTRODUCTION
CLINICAL MANIFESTATIONS OF SEPSISINDUCED CARDIAC DYSFUNCTION
PATHOPHYSIOLOGY OF SEPSIS-INDUCED CARDIAC DYSFUNCTION
Cytokines
Nitric oxide
Prostanoids
Endothelin-1
Intracellular adhesion molecules
Complement system
Histones and high mobility group box 1 (HMGB1)
Other mediators
Mitochondrial oxidative stress and injury
Abnormal calcium transport in mitochondria
Mitochondrial DNA
Mitochondrial dynamics
Mitochondrial biogenesis
Mitochondrial autophagy
CONCLUSIONS
KEY MESSAGES
-
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization & Data curation: all authors. Visualization: DK, KL, IJ. Writing–original draft: RH, IC. Writing–review&editing: HJC, IJ.
NOTES
- 1. Vieillard-Baron A. Septic cardiomyopathy. Ann Intensive Care 2011;1:6. ArticlePubMedPMCPDF
- 2. Hotchkiss RS, Karl IE. The pathophysiology and treatment of sepsis. N Engl J Med 2003;348:138-50.ArticlePubMed
- 3. Geri G, Vignon P, Aubry A, Fedou AL, Charron C, Silva S, et al. Cardiovascular clusters in septic shock combining clinical and echocardiographic parameters: a post hoc analysis. Intensive Care Med 2019;45:657-67.ArticlePubMedPDF
- 4. Fernandes CJ Jr, de Assuncao MS. Myocardial dysfunction in sepsis: a large, unsolved puzzle. Crit Care Res Pract 2012;2012:896430. ArticlePubMedPMCPDF
- 5. L’Heureux M, Sternberg M, Brath L, Turlington J, Kashiouris MG. Sepsis-induced cardiomyopathy: a comprehensive review. Curr Cardiol Rep 2020;22:35. ArticlePubMedPMCPDF
- 6. Pulido JN, Afessa B, Masaki M, Yuasa T, Gillespie S, Herasevich V, et al. Clinical spectrum, frequency, and significance of myocardial dysfunction in severe sepsis and septic shock. Mayo Clin Proc 2012;87:620-8.ArticlePubMedPMC
- 7. Muller-Werdan U, Buerke M, Ebelt H, Heinroth KM, Herklotz A, Loppnow H, et al. Septic cardiomyopathy: a not yet discovered cardiomyopathy? Exp Clin Cardiol 2006;11:226-36.PubMedPMC
- 8. Hoesel LM, Niederbichler AD, Ward PA. Complement-related molecular events in sepsis leading to heart failure. Mol Immunol 2007;44:95-102.ArticlePubMed
- 9. Parker MM, Suffredini AF, Natanson C, Ognibene FP, Shelhamer JH, Parrillo JE. Responses of left ventricular function in survivors and nonsurvivors of septic shock. J Crit Care 1989;4:19-25.Article
- 10. Poelaert J, Declerck C, Vogelaers D, Colardyn F, Visser CA. Left ventricular systolic and diastolic function in septic shock. Intensive Care Med 1997;23:553-60.ArticlePubMedPDF
- 11. Parker MM, Shelhamer JH, Bacharach SL, Green MV, Natanson C, Frederick TM, et al. Profound but reversible myocardial depression in patients with septic shock. Ann Intern Med 1984;100:483-90.ArticlePubMed
- 12. Parker MM, McCarthy KE, Ognibene FP, Parrillo JE. Right ventricular dysfunction and dilatation, similar to left ventricular changes, characterize the cardiac depression of septic shock in humans. Chest 1990;97:126-31.ArticlePubMed
- 13. Akira S, Uematsu S, Takeuchi O. Pathogen recognition and innate immunity. Cell 2006;124:783-801.ArticlePubMed
- 14. Raeburn CD, Sheppard F, Barsness KA, Arya J, Harken AH. Cytokines for surgeons. Am J Surg 2002;183:268-73.ArticlePubMed
- 15. Levy RJ, Piel DA, Acton PD, Zhou R, Ferrari VA, Karp JS, et al. Evidence of myocardial hibernation in the septic heart. Crit Care Med 2005;33:2752-6.ArticlePubMed
- 16. Antonucci E, Fiaccadori E, Donadello K, Taccone FS, Franchi F, Scolletta S. Myocardial depression in sepsis: from pathogenesis to clinical manifestations and treatment. J Crit Care 2014;29:500-11.ArticlePubMed
- 17. Kakihana Y, Ito T, Nakahara M, Yamaguchi K, Yasuda T. Sepsis-induced myocardial dysfunction: pathophysiology and management. J Intensive Care 2016;4:22. ArticlePubMedPMC
- 18. Kumar A, Krieger A, Symeoneides S, Kumar A, Parrillo JE. Myocardial dysfunction in septic shock. Part II. Role of cytokines and nitric oxide. J Cardiothorac Vasc Anesth 2001;15:485-511.ArticlePubMed
- 19. Pathan N, Hemingway CA, Alizadeh AA, Stephens AC, Boldrick JC, Oragui EE, et al. Role of interleukin 6 in myocardial dysfunction of meningococcal septic shock. Lancet 2004;363:203-9.ArticlePubMed
- 20. Loppnow H, Werdan K, Reuter G, Flad HD. The interleukin-1 and interleukin-1 converting enzyme families in the cardiovascular system. Eur Cytokine Netw 1998;9:675-80.PubMed
- 21. Kelly RA, Balligand JL, Smith TW. Nitric oxide and cardiac function. Circ Res 1996;79:363-80.ArticlePubMed
- 22. Francis SE, Holden H, Holt CM, Duff GW. Interleukin-1 in myocardium and coronary arteries of patients with dilated cardiomyopathy. J Mol Cell Cardiol 1998;30:215-23.ArticlePubMed
- 23. Opal SM, Fisher CJ Jr, Dhainaut JF, Vincent JL, Brase R, Lowry SF, et al. Confirmatory interleukin-1 receptor antagonist trial in severe sepsis: a phase III, randomized, double-blind, placebo- controlled, multicenter trial. The Interleukin-1 Receptor Antagonist Sepsis Investigator Group. Crit Care Med 1997;25:1115-24.ArticlePubMed
- 24. Müller-Werdan U, Werdan K. Immune modulation by catecholamines: a potential mechanism of cytokine release in heart failure? Herz 2000;25:271-3.ArticlePubMedPDF
- 25. Geppert A, Steiner A, Zorn G, Delle-Karth G, Koreny M, Haumer M, et al. Multiple organ failure in patients with cardiogenic shock is associated with high plasma levels of interleukin-6. Crit Care Med 2002;30:1987-94.ArticlePubMed
- 26. Rudiger A, Singer M. Mechanisms of sepsis-induced cardiac dysfunction. Crit Care Med 2007;35:1599-608.ArticlePubMed
- 27. Zanotti-Cavazzoni SL, Hollenberg SM. Cardiac dysfunction in severe sepsis and septic shock. Curr Opin Crit Care 2009;15:392-7.ArticlePubMed
- 28. Crouser ED, Julian MW, Huff JE, Joshi MS, Bauer JA, Gadd ME, et al. Abnormal permeability of inner and outer mitochondrial membranes contributes independently to mitochondrial dysfunction in the liver during acute endotoxemia. Crit Care Med 2004;32:478-88.ArticlePubMed
- 29. Memiş D, Karamanlioğlu B, Turan A, Koyuncu O, Pamukçu Z. Effects of lornoxicam on the physiology of severe sepsis. Crit Care 2004;8:R474-82.ArticlePubMedPMC
- 30. Konrad D, Oldner A, Rossi P, Wanecek M, Rudehill A, Weitzberg E. Differentiated and dose-related cardiovascular effects of a dual endothelin receptor antagonist in endotoxin shock. Crit Care Med 2004;32:1192-9.ArticlePubMed
- 31. Raeburn CD, Calkins CM, Zimmerman MA, Song Y, Ao L, Banerjee A, et al. ICAM-1 and VCAM-1 mediate endotoxemic myocardial dysfunction independent of neutrophil accumulation. Am J Physiol Regul Integr Comp Physiol 2002;283:R477-86.ArticlePubMed
- 32. Raeburn CD, Calkins CM, Zimmerman MA, Song Y, Ao L, Banerjee A, et al. Vascular cell adhesion molecule: 1 expression is obligatory for endotoxin-induced myocardial neutrophil accumulation and contractile dysfunction. Surgery 2001;130:319-25.ArticlePubMed
- 33. Niederbichler AD, Hoesel LM, Westfall MV, Gao H, Ipaktchi KR, Sun L, et al. An essential role for complement C5a in the pathogenesis of septic cardiac dysfunction. J Exp Med 2006;203:53-61.ArticlePubMedPMCPDF
- 34. Alhamdi Y, Abrams ST, Cheng Z, Jing S, Su D, Liu Z, et al. Circulating histones are major mediators of cardiac injury in patients with sepsis. Crit Care Med 2015;43:2094-103.ArticlePubMed
- 35. VanPatten S, Al-Abed Y. High mobility group box-1 (HMGb1):current wisdom and advancement as a potential drug target. J Med Chem 2018;61:5093-107.ArticlePubMed
- 36. Court O, Kumar A, Parrillo JE, Kumar A. Clinical review: myocardial depression in sepsis and septic shock. Crit Care 2002;6:500-8.ArticlePubMedPMC
- 37. Witthaut R, Busch C, Fraunberger P, Walli A, Seidel D, Pilz G, et al. Plasma atrial natriuretic peptide and brain natriuretic peptide are increased in septic shock: impact of interleukin-6 and sepsis-associated left ventricular dysfunction. Intensive Care Med 2003;29:1696-702.ArticlePubMedPDF
- 38. Grandel U, Hopf M, Buerke M, Hattar K, Heep M, Fink L, et al. Mechanisms of cardiac depression caused by lipoteichoic acids from Staphylococcus aureus in isolated rat hearts. Circulation 2005;112:691-8.ArticlePubMed
- 39. Jang DH, Greenwood JC, Spyres MB, Eckmann DM. Measurement of mitochondrial respiration and motility in acute care: sepsis, trauma, and poisoning. J Intensive Care Med 2017;32:86-94.ArticlePubMed
- 40. Carré JE, Singer M. Cellular energetic metabolism in sepsis: the need for a systems approach. Biochim Biophys Acta 2008;1777:763-71.ArticlePubMed
- 41. Brealey D, Brand M, Hargreaves I, Heales S, Land J, Smolenski R, et al. Association between mitochondrial dysfunction and severity and outcome of septic shock. Lancet 2002;360:219-23.ArticlePubMed
- 42. Potz BA, Sellke FW, Abid MR. Endothelial ROS and impaired myocardial oxygen consumption in sepsis-induced cardiac dysfunction. J Intensive Crit Care 2016;2:20. ArticlePubMedPMC
- 43. Larsen FJ, Schiffer TA, Weitzberg E, Lundberg JO. Regulation of mitochondrial function and energetics by reactive nitrogen oxides. Free Radic Biol Med 2012;53:1919-28.ArticlePubMed
- 44. Crouser ED. Mitochondrial dysfunction in septic shock and multiple organ dysfunction syndrome. Mitochondrion 2004;4:729-41.ArticlePubMed
- 45. Kayali R, Aydin S, Cakatay U. Effect of gender on main clinical chemistry parameters in aged rats. Curr Aging Sci 2009;2:67-71.ArticlePubMed
- 46. Galley HF. Oxidative stress and mitochondrial dysfunction in sepsis. Br J Anaesth 2011;107:57-64.ArticlePubMedPDF
- 47. Lowes DA, Webster NR, Murphy MP, Galley HF. Antioxidants that protect mitochondria reduce interleukin-6 and oxidative stress, improve mitochondrial function, and reduce biochemical markers of organ dysfunction in a rat model of acute sepsis. Br J Anaesth 2013;110:472-80.ArticlePubMedPMCPDF
- 48. Bernardi P, Di Lisa F. The mitochondrial permeability transition pore: molecular nature and role as a target in cardioprotection. J Mol Cell Cardiol 2015;78:100-6.ArticlePubMedPMC
- 49. Duncan DJ, Yang Z, Hopkins PM, Steele DS, Harrison SM. TNFalpha and IL-1beta increase Ca2+ leak from the sarcoplasmic reticulum and susceptibility to arrhythmia in rat ventricular myocytes. Cell Calcium 2010;47:378-86.ArticlePubMedPMC
- 50. Hassoun SM, Marechal X, Montaigne D, Bouazza Y, Decoster B, Lancel S, et al. Prevention of endotoxin-induced sarcoplasmic reticulum calcium leak improves mitochondrial and myocardial dysfunction. Crit Care Med 2008;36:2590-6.ArticlePubMed
- 51. Shanmuganathan S, Hausenloy DJ, Duchen MR, Yellon DM. Mitochondrial permeability transition pore as a target for cardioprotection in the human heart. Am J Physiol Heart Circ Physiol 2005;289:H237-42.ArticlePubMed
- 52. Smeding L, Plötz FB, Groeneveld AB, Kneyber MC. Structural changes of the heart during severe sepsis or septic shock. Shock 2012;37:449-56.ArticlePubMed
- 53. Finkel MS, Oddis CV, Jacob TD, Watkins SC, Hattler BG, Simmons RL. Negative inotropic effects of cytokines on the heart mediated by nitric oxide. Science 1992;257:387-9.ArticlePubMed
- 54. Wu LL, Ji Y, Dong LW, Liu MS. Calcium uptake by sarcoplasmic reticulum is impaired during the hypodynamic phase of sepsis in the rat heart. Shock 2001;15:49-55.ArticlePubMed
- 55. Galluzzi L, Kepp O, Trojel-Hansen C, Kroemer G. Mitochondrial control of cellular life, stress, and death. Circ Res 2012;111:1198-207.ArticlePubMed
- 56. Nunnari J, Suomalainen A. Mitochondria: in sickness and in health. Cell 2012;148:1145-59.ArticlePubMedPMC
- 57. Harrington JS, Choi AM, Nakahira K. Mitochondrial DNA in Sepsis. Curr Opin Crit Care 2017;23:284-90.ArticlePubMedPMC
- 58. Nakahira K, Haspel JA, Rathinam VA, Lee SJ, Dolinay T, Lam HC, et al. Autophagy proteins regulate innate immune responses by inhibiting the release of mitochondrial DNA mediated by the NALP3 inflammasome. Nat Immunol 2011;12:222-30.ArticlePubMedPDF
- 59. Nakahira K, Kyung SY, Rogers AJ, Gazourian L, Youn S, Massaro AF, et al. Circulating mitochondrial DNA in patients in the ICU as a marker of mortality: derivation and validation. PLoS Med 2013;10:e1001577.ArticlePubMedPMC
- 60. Bhagirath VC, Dwivedi DJ, Liaw PC. Comparison of the proinflammatory and procoagulant properties of nuclear, mitochondrial, and bacterial DNA. Shock 2015;44:265-71.ArticlePubMed
- 61. Sánchez-Villamil JP, D’Annunzio V, Finocchietto P, Holod S, Rebagliati I, Pérez H, et al. Cardiac-specific overexpression of thioredoxin 1 attenuates mitochondrial and myocardial dysfunction in septic mice. Int J Biochem Cell Biol 2016;81(Pt B):323-34.ArticlePubMed
- 62. Liesa M, Palacín M, Zorzano A. Mitochondrial dynamics in mammalian health and disease. Physiol Rev 2009;89:799-845.ArticlePubMed
- 63. Zhan M, Brooks C, Liu F, Sun L, Dong Z. Mitochondrial dynamics: regulatory mechanisms and emerging role in renal pathophysiology. Kidney Int 2013;83:568-81.ArticlePubMedPMC
- 64. Wu Y, Yao YM, Lu ZQ. Mitochondrial quality control mechanisms as potential therapeutic targets in sepsis-induced multiple organ failure. J Mol Med (Berl) 2019;97:451-62.ArticlePubMedPDF
- 65. Singer M. The role of mitochondrial dysfunction in sepsis-induced multi-organ failure. Virulence 2014;5:66-72.ArticlePubMed
- 66. Gunst J, Derese I, Aertgeerts A, Ververs EJ, Wauters A, Van den Berghe G, et al. Insufficient autophagy contributes to mitochondrial dysfunction, organ failure, and adverse outcome in an animal model of critical illness. Crit Care Med 2013;41:182-94.ArticlePubMed
- 67. Rocha M, Herance R, Rovira S, Hernández-Mijares A, Victor VM. Mitochondrial dysfunction and antioxidant therapy in sepsis. Infect Disord Drug Targets 2012;12:161-78.ArticlePubMed
References
Figure & Data
References
Citations
- Neonatal sepsis and cardiovascular dysfunction I: mechanisms and pathophysiology
Sophie M. Duignan, Satyan Lakshminrusimha, Kathryn Armstrong, Willem P. de Boode, Afif El-Khuffash, Orla Franklin, Eleanor J. Molloy, Willem P. de Boode, Franz B. Plötz, Tobias Strunk, Marina Degtyareva, Helmut Küster, Eric Giannoni, Joseph M. Bliss, H. R
Pediatric Research.2024; 95(5): 1207. CrossRef - 6-Gingerol, an ingredient of Zingiber officinale, abrogates lipopolysaccharide-induced cardiomyocyte injury by reducing oxidative stress and inflammation
Azar Hosseini, Mohaddeseh Sadat Alavi, Mitra Ghane Nikookar Toos, Tannaz Jamialahmadi, Amirhossein Sahebkar
Journal of Agriculture and Food Research.2024; 15: 101034. CrossRef - Inflammation and arrhythmogenesis: a narrative review of the complex relationship
Andia Taghdiri
International Journal of Arrhythmia.2024;[Epub] CrossRef - Inotropic drugs in septic shock
Nutnicha Yolsiriwat, Surat Tongyoo
Clinical Critical Care.2024;[Epub] CrossRef - Epigallocatechin-3-gallate protects sepsis‐induced myocardial dysfunction by inhibiting the nuclear factor-κB signaling pathway
Bei Chen, Ya-Fei Li, Zhang Fang, Wen-Yi Cai, Zhi-Qiang Tian, Dianfu Li, Ze-Mu Wang
Heliyon.2024; 10(5): e27163. CrossRef - Myocardial Injury as a Harbinger of Multi-organ Failure in Septic Shock: A Comprehensive Review
Amol Singam
Cureus.2024;[Epub] CrossRef - Case 9-2024: An 84-Year-Old Man with a Fall
Richard C. Cabot, Eric S. Rosenberg, David M. Dudzinski, Meridale V. Baggett, Kathy M. Tran, Dennis C. Sgroi, Jo-Anne O. Shepard, Emily K. McDonald, Tara Corpuz, Zaven Sargsyan, Sunita D. Srivastava, Virginia A. Triant, Brian B. Ghoshhajra
New England Journal of Medicine.2024; 390(12): 1129. CrossRef - Melatonin: A potential protective multifaceted force for sepsis-induced cardiomyopathy
Eman Casper, Lamia El Wakeel, Nagwa Sabri, Ramy Khorshid, Sarah F. Fahmy
Life Sciences.2024; 346: 122611. CrossRef - Hemodynamic goals in sepsis and septic shock resuscitation: An umbrella review of systematic reviews and meta-analyses with trial sequential analysis
Daniele Orso, Nicola Federici, Cristina Lio, Filippo Mearelli, Tiziana Bove
Australian Critical Care.2024;[Epub] CrossRef - NOVEL ECHOCARDIOGRAM ANALYSIS OF CARDIAC DYSFUNCTION IS ASSOCIATED WITH MORTALITY IN PEDIATRIC SEPSIS
Daniel T. Cater, Brett A. Meyers, Shailee Mitra, Sayantan Bhattacharya, Roberto F. Machado, Ryan Serrano, Courtney M. Rowan, Benjamin Gaston, Pavlos Vlachos
Shock.2024; 62(1): 26. CrossRef - From Molecular Mechanisms to Clinical Therapy: Understanding Sepsis-Induced Multiple Organ Dysfunction
Tijana Srdić, Siniša Đurašević, Iva Lakić, Aleksandra Ružičić, Predrag Vujović, Tanja Jevđović, Tamara Dakić, Jelena Đorđević, Tomislav Tosti, Sofija Glumac, Zoran Todorović, Nebojša Jasnić
International Journal of Molecular Sciences.2024; 25(14): 7770. CrossRef - A case of sepsis‐induced cardiomyopathy successfully treated with venoarterial extracorporeal membrane oxygenation
Keigo Sato, Akihiro Naito, Taichi Shiratori, Masahiro Yamamoto, Kenichi Shimane, Manabu Mikami, Mariko Senda, Haruki Kume, Motofumi Suzuki
IJU Case Reports.2023; 6(1): 26. CrossRef - Jujuboside A attenuates sepsis-induced cardiomyopathy by inhibiting inflammation and regulating autophagy
Zi Wang, Danrui Xiao, Qingqi Ji, Yanjie Li, Zhaohua Cai, Liang Fang, Huanhuan Huo, Guo Zhou, Xiangming Yan, Linghong Shen, Ben He
European Journal of Pharmacology.2023; 947: 175451. CrossRef - Mitochondrial transplantation protects against sepsis-induced myocardial dysfunction by modulating mitochondrial biogenesis and fission/fusion and inflammatory response
Behnaz Mokhtari, Masoud Hamidi, Reza Badalzadeh, Ata Mahmoodpoor
Molecular Biology Reports.2023; 50(3): 2147. CrossRef - Therapeutic potentials of stem cell–derived exosomes in cardiovascular diseases
Saiprahalad Mani, Narasimman Gurusamy, Thennavan Ulaganathan, Autumn J Paluck, Satish Ramalingam, Johnson Rajasingh
Experimental Biology and Medicine.2023; 248(5): 434. CrossRef - CLINICAL, MOLECULAR, AND EXOSOMAL MECHANISMS OF CARDIAC AND BRAIN DYSFUNCTION IN SEPSIS
Daniel C. Morris, Zheng Gang Zhang, Anja K. Jaehne, Jing Zhang, Emanuel P. Rivers
Shock.2023; 59(2): 173. CrossRef - Circulating protein and lipid markers of early sepsis diagnosis and prognosis: a scoping review
Gemma Barber, Jelena Tanic, Aleksandra Leligdowicz
Current Opinion in Lipidology.2023; 34(2): 70. CrossRef - Extracellular Histone-Induced Protein Kinase C Alpha Activation and Troponin Phosphorylation Is a Potential Mechanism of Cardiac Contractility Depression in Sepsis
Simon T. Abrams, Yasir Alhamdi, Min Zi, Fengmei Guo, Min Du, Guozheng Wang, Elizabeth J. Cartwright, Cheng-Hock Toh
International Journal of Molecular Sciences.2023; 24(4): 3225. CrossRef - Septic cardiomyopathy: A narrative review
Maria Rita Lima, Doroteia Silva
Revista Portuguesa de Cardiologia.2023; 42(5): 471. CrossRef - Enfoque de la miocardiopatía séptica como causa de choque refractario en escenarios de recursos limitados: reporte de caso
Liliana Correa-Pérez, Diana Carolina Otálora Álvarez, Gloria Camila Álvarez Gallego
Acta Colombiana de Cuidado Intensivo.2023; 23(3): 303. CrossRef - Role of Pellino-1 in Inflammation and Cardioprotection following Severe Sepsis: A Novel Mechanism in a Murine Severe Sepsis Model †
Mahesh Thirunavukkarasu, Santosh Swaminathan, Andrew Kemerley, Seetur R. Pradeep, Sue Ting Lim, Diego Accorsi, Rickesha Wilson, Jacob Campbell, Ibnalwalid Saad, Siu-Pok Yee, J. Alexander Palesty, David W. McFadden, Nilanjana Maulik
Cells.2023; 12(11): 1527. CrossRef - circHIPK3 exacerbates sepsis-induced acute kidney injury and cardiopulmonary function by regulating microRNA-106a-5p/ROCK2 axis
Heng Li, Lingkai Kang, Jianglu Tan, Wanli Li, Dongrui He, Jing Han, Jie Zhang, Yulin Guan, Ying Huang, Xiaoyue Li
Process Biochemistry.2023; 131: 272. CrossRef - Estradiol as the Trigger of Sirtuin-1-Dependent Cell Signaling with a Potential Utility in Anti-Aging Therapies
Kamil Karolczak, Cezary Watala
International Journal of Molecular Sciences.2023; 24(18): 13753. CrossRef - Baricitinib protects mice from sepsis-induced cardiac dysfunction and multiple-organ failure
Chiara Verra, Shireen Mohammad, Gustavo Ferreira Alves, Elisa Porchietto, Sina Maren Coldewey, Massimo Collino, Christoph Thiemermann
Frontiers in Immunology.2023;[Epub] CrossRef - Therapeutic S100A8/A9 blockade inhibits myocardial and systemic inflammation and mitigates sepsis-induced myocardial dysfunction
Gabriel Jakobsson, Praveen Papareddy, Henrik Andersson, Megan Mulholland, Ravi Bhongir, Irena Ljungcrantz, Daniel Engelbertsen, Harry Björkbacka, Jan Nilsson, Adrian Manea, Heiko Herwald, Marisol Ruiz-Meana, Antonio Rodríguez-Sinovas, Michelle Chew, Alexa
Critical Care.2023;[Epub] CrossRef - Cardiac troponin as a prognosticator of mortality in patients with sepsis: A systematic review and meta‐analysis
Peiqiu Zheng, Xing Wang, Tao Guo, Wei Gao, Qiang Huang, Jie Yang, Hui Gao, Qian Liu
Immunity, Inflammation and Disease.2023;[Epub] CrossRef - Decoding molecular signature on heart of septic mice with distinct left ventricular ejection fraction
Lina Zhang, Desheng Qi, Milin Peng, Binbin Meng, Xinrun Wang, Xiaolei Zhang, Zhihong Zuo, Li Li, Zhanwen Wang, Wenxuan Zou, Zhonghua Hu, Zhaoxin Qian
iScience.2023; 26(10): 107825. CrossRef - Role of toll-like receptor-mediated pyroptosis in sepsis-induced cardiomyopathy
Yixuan Fan, Baoyi Guan, Jianxing Xu, He Zhang, Liang Yi, Zhixu Yang
Biomedicine & Pharmacotherapy.2023; 167: 115493. CrossRef - Understanding yellow fever-associated myocardial injury: an autopsy study
Fernando Rabioglio Giugni, Vera Demarchi Aiello, Caroline Silverio Faria, Shahab Zaki Pour, Marielton dos Passos Cunha, Melina Valdo Giugni, Henrique Trombini Pinesi, Felipe Lourenço Ledesma, Carolina Esteves Morais, Yeh-Li Ho, Jaques Sztajnbok, Sandra de
eBioMedicine.2023; 96: 104810. CrossRef - The role of beta-blocker drugs in critically ill patients: a SIAARTI expert consensus statement
Fabio Guarracino, Andrea Cortegiani, Massimo Antonelli, Astrid Behr, Giandomenico Biancofiore, Alfredo Del Gaudio, Francesco Forfori, Nicola Galdieri, Giacomo Grasselli, Gianluca Paternoster, Monica Rocco, Stefano Romagnoli, Salvatore Sardo, Sascha Treska
Journal of Anesthesia, Analgesia and Critical Care.2023;[Epub] CrossRef - Sedation for Patients with Sepsis: Towards a Personalised Approach
José Miguel Marcos-Vidal, Rafael González, María Merino, Eva Higuera, Cristina García
Journal of Personalized Medicine.2023; 13(12): 1641. CrossRef - High serum nitrates levels in non-survivor COVID-19 patients
L. Lorente, F. Gómez-Bernal, M.M. Martín, J.A. Navarro-Gonzálvez, M. Argueso, A. Perez, L. Ramos-Gómez, J. Solé-Violán, J.A. Marcos y Ramos, N. Ojeda, A. Jiménez
Medicina Intensiva.2022; 46(3): 132. CrossRef - Vital signs as physiomarkers of neonatal sepsis
Brynne A. Sullivan, Karen D. Fairchild
Pediatric Research.2022; 91(2): 273. CrossRef - Fluid therapy for severe malaria
Laura C Kalkman, Thomas Hänscheid, Sanjeev Krishna, Martin P Grobusch
The Lancet Infectious Diseases.2022; 22(6): e160. CrossRef - High serum nitrates levels in non-survivor COVID-19 patients
L. Lorente, F. Gómez-Bernal, M.M. Martín, J.A. Navarro-Gonzálvez, M. Argueso, A. Perez, L. Ramos-Gómez, J. Solé-Violán, J.A. Marcos y Ramos, N. Ojeda, A. Jiménez
Medicina Intensiva (English Edition).2022; 46(3): 132. CrossRef - Expression of Peripheral Blood DCs CD86, CD80, and Th1/Th2 in Sepsis Patients and Their Value on Survival Prediction
Ke Du, Shaobo Hao, Heyun Luan, Min Tang
Computational and Mathematical Methods in Medicine.2022; 2022: 1. CrossRef - Recombinant Activated Protein C (rhAPC) Affects Lipopolysaccharide-Induced Mechanical Compliance Changes and Beat Frequency of mESC-Derived Cardiomyocyte Monolayers
Aysegül Temiz Artmann, Eylem Kurulgan Demirci, Ipek Seda Fırat, Hakan Oflaz, Gerhard M. Artmann
Shock.2022; 57(4): 544. CrossRef - Acute cholecystitis associated with sepsis-induced ischemic cardiomyopathy
Ke-Shiuan Ju, Ying-Shih Su, Wen-Sen Lee
Journal of Infection.2022; 84(6): 834. CrossRef - An Overview on Mitochondrial-Based Therapies in Sepsis-Related Myocardial Dysfunction: Mitochondrial Transplantation as a Promising Approach
Behnaz Mokhtari, Rana Yavari, Reza Badalzadeh, Ata Mahmoodpoor, Jayaraman Tharmalingam
Canadian Journal of Infectious Diseases and Medical Microbiology.2022; 2022: 1. CrossRef - Pathological role of the calcium‐sensing receptor in sepsis‐induced hypotensive shock: Therapeutic possibilities and unanswered questions
Ankita Sood, Gaaminepreet Singh, Thakur G. Singh, Kirti Gupta
Drug Development Research.2022; 83(6): 1241. CrossRef - Diminazene aceturate mitigates cardiomyopathy by interfering with renin-angiotensin system in a septic rat model
Zhaoqing Lu, Di Wu, Zheng Wang, Hanyu Zhang, Yufan Du, Guoxing Wang
BMC Pharmacology and Toxicology.2022;[Epub] CrossRef - Serum Sestrin2 Was Lower in Septic Shock Patients with Cardiomyopathy
Rongjin Huang, Feng Chen, Aiying Zeng, Jun Ke, Shirong Lin, QiXing Chen
Disease Markers.2022; 2022: 1. CrossRef - Tidy up - The unfolded protein response in sepsis
Wolfgang Vivas, Sebastian Weis
Frontiers in Immunology.2022;[Epub] CrossRef - DAMPs Released from Proinflammatory Macrophages Induce Inflammation in Cardiomyocytes via Activation of TLR4 and TNFR
Carolina Neu, Yvonne Thiele, Fabienne Horr, Christian Beckers, Nadine Frank, Gernot Marx, Lukas Martin, Sandra Kraemer, Elisabeth Zechendorf
International Journal of Molecular Sciences.2022; 23(24): 15522. CrossRef - Targeting the TXNIP‐NLRP3 interaction with PSSM1443 to suppress inflammation in sepsis‐induced myocardial dysfunction
Linhua Wang, Hongsheng Zhao, Huifen Xu, Xiangxin Liu, Xinlong Chen, Qingyun Peng, Mingbing Xiao
Journal of Cellular Physiology.2021; 236(6): 4625. CrossRef - Sepsis—Pathophysiology and Therapeutic Concepts
Dominik Jarczak, Stefan Kluge, Axel Nierhaus
Frontiers in Medicine.2021;[Epub] CrossRef - Rho-Proteins and Downstream Pathways as Potential Targets in Sepsis and Septic Shock: What Have We Learned from Basic Research
Maria Luísa da Silveira Hahmeyer, José Eduardo da Silva-Santos
Cells.2021; 10(8): 1844. CrossRef - Deep-learning model for screening sepsis using electrocardiography
Joon-myoung Kwon, Ye Rang Lee, Min-Seung Jung, Yoon-Ji Lee, Yong-Yeon Jo, Da-Young Kang, Soo Youn Lee, Yong-Hyeon Cho, Jae-Hyun Shin, Jang-Hyeon Ban, Kyung-Hee Kim
Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine.2021;[Epub] CrossRef - Levosimendan versus dobutamine for sepsis-induced cardiac dysfunction: a systematic review and meta-analysis
Dong-Hua Liu, Yi-Le Ning, Yan-Yan Lei, Jing Chen, Yan-Yan Liu, Xin-Feng Lin, Zhong-Qi Yang, Shao-Xiang Xian, Wei-Tao Chen
Scientific Reports.2021;[Epub] CrossRef - Exosomes Derived from miR-146a-5p-Enriched Mesenchymal Stem Cells Protect the Cardiomyocytes and Myocardial Tissues in the Polymicrobial Sepsis through Regulating MYBL1
Chun Liu, Jianhua Xue, Bo Xu, Aixian Zhang, Lili Qin, Jiajia Liu, Yang Yang, Antonio C. Campos de Carvalho
Stem Cells International.2021; 2021: 1. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite