Articles
- Page Path
- HOME > Acute Crit Care > Volume 35(1); 2020 > Article
-
Original Article
Surgery Outcomes of bedside peripherally inserted central catheter placement: a retrospective study at a single institution -
Sukyung Kwon1
 , Soo mi Son2, Seul Hee Lee2, Joung Hee Kim2, Hyangkyoung Kim1, Jang Yong Kim1, Ji Il Kim3, In Sung Moon4
, Soo mi Son2, Seul Hee Lee2, Joung Hee Kim2, Hyangkyoung Kim1, Jang Yong Kim1, Ji Il Kim3, In Sung Moon4 -
Acute and Critical Care 2020;35(1):31-37.
DOI: https://doi.org/10.4266/acc.2019.00731
Published online: February 11, 2020
1Division of Vascular and Transplant Surgery, Department of Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Division of Vascular and Transplant Surgery, Department of Nursing, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
3Division of Vascular and Transplant Surgery, Department of Surgery, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea
4Division of Vascular and Transplant Surgery, Department of Surgery, Yeouido St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- Corresponding author Hyangkyoung Kim Division of Vascular and Transplant Surgery, Department of Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea Tel: +82-2-2258-6744 Fax: +82-2-595-2822 E-mail: cindycrow7456@gmail.com
Copyright © 2020 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background:
- Bedside insertion of peripherally inserted central catheters (PICCs) has higher rates of malposition than fluoroscopic-guided PICC placement. This study evaluated the success rate of bedside PICC placement, variations in tip location, and risk factors for malposition.
-
Methods:
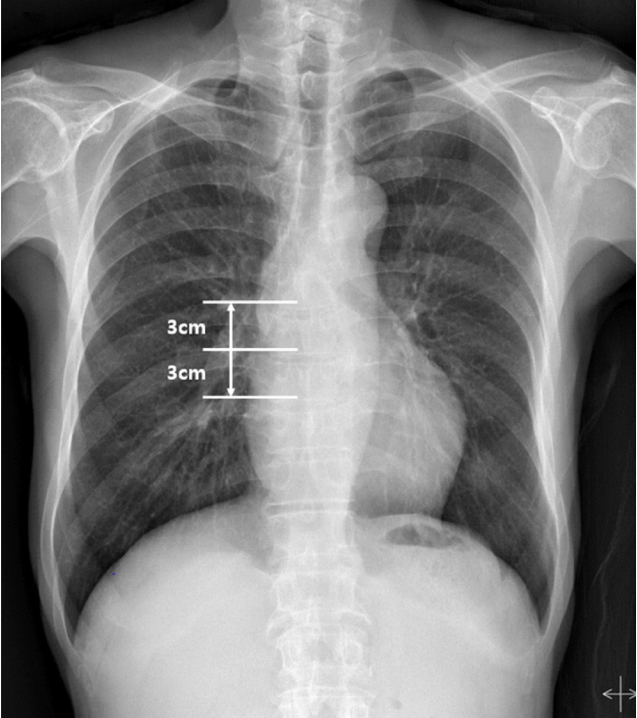
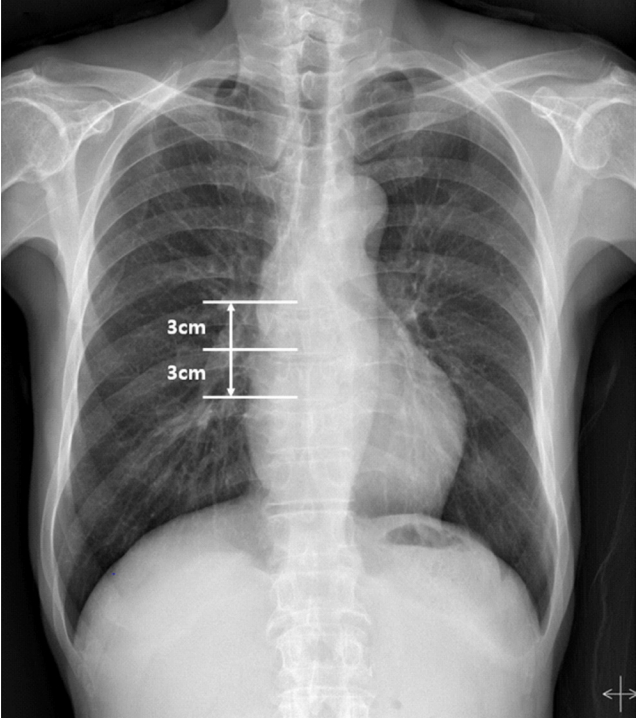
- This retrospective study included patients who underwent bedside PICC placement from January 2013 to September 2014 in a single institution. The procedure was conducted under ultrasound guidance or by a blind method. After PICC placement, tip location was determined by chest X-ray.
-
Results:
- The overall venous access success rate with bedside PICC placement was 98.1% (1,302/ 1,327). There was no significant difference in the venous access success rate between ultrasound-guided placement (868/880, 98.6%) and a blind approach placement (434/447, 97.1%). Optimal tip position was achieved on the first attempt in 1,192 cases (91.6%). Repositioning was attempted in 65 patients; 60 PICCs were repositioned at the bedside, two PICCs were repositioned under fluoroscopic guidance, and three PICCs moved to the desired position without intervention. Final optimal tip position after repositioning was achieved in 1,229 (94.4%). In logistic regression analysis, five factors associated with tip malposition included female sex (Exp(B), 1.687; 95% confidence interval [CI], 1.180 to 2.412; P=0.004), older age (Exp(B), 1.026; 95% CI, 1.012 to 1.039; P<0.001), cancer (Exp(B), 0.650; 95% CI, 0.455 to 0.929; P=0.018), lung disease (Exp(B), 2.416; 95% CI, 1.592 to 3.666; P<0.001), and previous catheter insertions (Exp(B), 1.262; 95% CI, 1.126 to 1.414; P<0.001).
-
Conclusions:
- Bedside PICC placement without fluoroscopy is effective and safe in central venous catheters. Potential risk factors associated with catheter tip malposition include older age, female sex, cancer, pulmonary disease, and previous central vein catheterizations.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
KEY MESSAGES
-
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: JYK, HK, JIK, ISM. Data curation: SMS, SHL, JHK, SK. Formal analysis: SMS, SK, HK, JYK. Methodology: SK, SMS, HK, JYK. Project administration: JYK, JIK, ISM. Visualization: SK, HK. Writing - original draft: SK, SMS, HK. Writing - review & editing: all authors.
NOTES
Acknowledgments
- 1. Parkinson R, Gandhi M, Harper J, Archibald C. Establishing an ultrasound guided peripherally inserted central catheter (PICC) insertion service. Clin Radiol 1998;53:33-6.ArticlePubMed
- 2. Botella-Carretero JI, Carrero C, Guerra E, Valbuena B, Arrieta F, Calañas A, et al. Role of peripherally inserted central catheters in home parenteral nutrition: a 5-year prospective study. JPEN J Parenter Enteral Nutr 2013;37:544-9.ArticlePubMed
- 3. Spaziani S, Micheli T, Vincenzi B, Campisi C. Groshong PICC and home care: an opportunity: clinical experience after the first 200 implants. J Vasc Access 2000;1:108-11.ArticlePubMed
- 4. Todd J. Peripherally inserted central catheters and their use in i.v. therapy. Br J Nurs 1999;8:140-4.ArticlePubMed
- 5. Seckold T, Walker S, Dwyer T. A comparison of silicone and polyurethane PICC lines and postinsertion complication rates: a systematic review. J Vasc Access 2015;16:167-77.ArticlePubMed
- 6. Hoshal VL Jr. Total intravenous nutrition with peripherally inserted silicone elastomer central venous catheters. Arch Surg 1975;110:644-6.ArticlePubMed
- 7. Scrivens N, Sabri E, Bredeson C, McDiarmid S. Comparison of complication rates and incidences associated with different peripherally inserted central catheters (PICC) in patients with hematological malignancies: a retrospective cohort study. Leuk Lymphoma 2020;61:156-64.ArticlePubMed
- 8. Glauser F, Breault S, Rigamonti F, Sotiriadis C, Jouannic AM, Qanadli SD. Tip malposition of peripherally inserted central catheters: a prospective randomized controlled trial to compare bedside insertion to fluoroscopically guided placement. Eur Radiol 2017;27:2843-9.ArticlePubMedPDF
- 9. Trerotola SO, Thompson S, Chittams J, Vierregger KS. Analysis of tip malposition and correction in peripherally inserted central catheters placed at bedside by a dedicated nursing team. J Vasc Interv Radiol 2007;18:513-8.ArticlePubMed
- 10. Racadio JM, Doellman DA, Johnson ND, Bean JA, Jacobs BR. Pediatric peripherally inserted central catheters: complication rates related to catheter tip location. Pediatrics 2001;107:E28. ArticlePubMed
- 11. Petersen J, Delaney JH, Brakstad MT, Rowbotham RK, Bagley CM Jr. Silicone venous access devices positioned with their tips high in the superior vena cava are more likely to malfunction. Am J Surg 1999;178:38-41.ArticlePubMed
- 12. Luciani A, Clement O, Halimi P, Goudot D, Portier F, Bassot V, et al. Catheter-related upper extremity deep venous thrombosis in cancer patients: a prospective study based on Doppler US. Radiology 2001;220:655-60.ArticlePubMed
- 13. LaRue GD. Efficacy of ultrasonography in peripheral venous cannulation. J Intraven Nurs 2000;23:29-34.PubMed
- 14. Mazzola JR, Schott-Baer D, Addy L. Clinical factors associated with the development of phlebitis after insertion of a peripherally inserted central catheter. J Intraven Nurs 1999;22:36-42.PubMed
- 15. Jeon EY, Koh SH, Lee IJ, Ha HI, Park BJ. Useful equation for proper estimate of left side peripherally inserted central venous catheter length in relation to the height. J Vasc Access 2015;16:42-6.ArticlePubMed
- 16. Song L, Li X, Guo Y, Ye M, Ma Y, Guo M, et al. Malposition of peripherally inserted central catheter: experience from 3012 cancer patients. Int J Nurs Pract 2014;20:446-9.ArticlePubMed
- 17. Nakamuta S, Nishizawa T, Matsuhashi S, Shimizu A, Uraoka T, Yamamoto M. Real-time ultrasound-guided placement of peripherally inserted central venous catheter without fluoroscopy. J Vasc Access 2018;19:609-614.ArticlePubMed
- 18. Rasuli P, Hammond DI, Peterkin IR. Spontaneous intrajugular migration of long-term central venous access catheters. Radiology 1992;182:822-4.ArticlePubMed
- 19. Qiu XX, Guo Y, Fan HB, Shao J, Zhang XB. Incidence, risk factors and clinical outcomes of peripherally inserted central catheter spontaneous dislodgment in oncology patients: a prospective cohort study. Int J Nurs Stud 2014;51:955-63.ArticlePubMed
- 20. Muhm M, Sunder-Plassmann G, Apsner R, Pernerstorfer T, Rajek A, Lassnigg A, et al. Malposition of central venous catheters: incidence, management and preventive practices. Wien Klin Wochenschr 1997;109:400-5.PubMed
- 21. Ruesch S, Walder B, Tramèr MR. Complications of central venous catheters: internal jugular versus subclavian access: a systematic review. Crit Care Med 2002;30:454-60.ArticlePubMed
- 22. Vesely TM. Central venous catheter tip position: a continuing controversy. J Vasc Interv Radiol 2003;14:527-34.ArticlePubMed
- 23. Weber E, Liberek T, Wołyniec W, Rutkowski B. Catheter tip malposition after percutaneous placement of tunneled hemodialysis catheters. Hemodial Int 2015;19:509-13.ArticlePubMed
- 24. Sharp R, Cummings M, Childs J, Fielder A, Mikocka-Walus A, Grech C, et al. Measurement of vein diameter for peripherally inserted central catheter (PICC) insertion: an observational study. J Infus Nurs 2015;38:351-7.ArticlePubMed
- 25. Cho HH, Jeon EY, Lee HJ, Lee H, Koh SH, Choi SY, et al. A new formula to estimate the length of right upper extremity vein from elbow crease to carina calculated by peripherally inserted central catheter insertion through right basilic vein puncture. J Korean Soc Radiol 2012;66:229-33.Article
References
Figure & Data
References
Citations
- The Outcomes of Peripherally Inserted Central Catheter (PICC) Insertion in Pediatric Patients at Siriraj Hospital
Niracha Wongchompoo, Khanita Kasikan, Prasert Sawasdiwipachai
Siriraj Medical Journal.2024; 76(3): 135. CrossRef - Catheter detection by transthoracic echocardiography during placement of peripherally inserted central catheters: a real-time method for eliminating misplacement
Yong Chae Jung, Man-shik Shim, Hee Sun Park, Min-Woong Kang
Acute and Critical Care.2024; 39(2): 266. CrossRef - Factors Associated with Successful First-attempt Puncture in Pediatric Patients Undergoing Ultrasound-guided Peripherally Inserted Central Catheter
Midan Zhang, Xiaofei Chen, Hongqin Zhou, Meifang Xu
Innovative Journal of Pediatrics.2023;[Epub] CrossRef - Factors Associated with Successful First-attempt Puncture in Pediatric Patients Undergoing Ultrasound-guided Peripherally Inserted Central Catheter
Midan Zhang, Xiaofei Chen, Hongqin Zhou, Meifang Xu
Iranian Journal of Pediatrics.2023;[Epub] CrossRef - Feasibility of Ultrasound-Guided, Peripherally Inserted Central Catheter Placement at the Bedside in a Communicable-Disease Isolation Unit
Kyoung Won Yoon, Wongook Wi, Moon Suk Choi, Eunmi Gil, Chi-Min Park, Keesang Yoo
Journal of Personalized Medicine.2023; 13(5): 863. CrossRef - Development and validation of an updated PICC length prediction formula based on anteroposterior chest radiographs for the ultrasound-guided bedside placement
Hyoung Nam Lee, Sangjoon Lee, Sung-Joon Park, Youngjong Cho, Hwan Hoon Chung, Robert Jeenchen Chen
PLOS ONE.2023; 18(11): e0294598. CrossRef - Analysis of tip malposition and correction of peripherally inserted central catheters under ultrasound-guidance: 5-year outcomes from a single center
Eunju Jang, Soo Mi Son, Ki-yoon Moon, Seunghoon Lee, Hong Seok Han, Sun Cheol Park, Jang Yong Kim, Sang Seob Yun
The Journal of Vascular Access.2023;[Epub] CrossRef - Precision at the Bedside: Practical Efficacy of Clockwise Catheter Torque for Accurate Tip Positioning of Peripherally Inserted Central Catheters
Masayuki Akatsuka, Eriko Sugiyama
Cureus.2023;[Epub] CrossRef - Guidewire-Assisted Reduction Technology Combined with Postural Reduction Improves the Success Rate of Internal Vein Catheterisation
Feng-Xian Li, Yan-Ping Li, Hong-Yang Zhang, Mei-Jing Tian, Huan-Huan Gao, Gui-Juan Zhang, Peng Su, Daniel Espino
Journal of Healthcare Engineering.2022; 2022: 1. CrossRef - Therapeutic Effect of Ultrasound-Guided Peripherally Inserted Central Catheter Combined with Predictive Nursing in Patients with Large-Area Severe Burns
Baiyan He, Aiqiong Zhang, Shuting He, Pan Zheng
Computational and Mathematical Methods in Medicine.2022; 2022: 1. CrossRef - Bedside peripherally inserted central catheter placement: focus on the procedure
Dong Hun Kim
Trauma Image and Procedure.2022; 7(1): 21. CrossRef - Validation of the PICC length prediction formula based on anteroposterior chest radiographs for bedside ultrasound-guided placement
Youngjong Cho, Sangjoon Lee, Sung-Joon Park, Hyoung Nam Lee, Hwan Hoon Chung, Robert Jeenchen Chen
PLOS ONE.2022; 17(11): e0277526. CrossRef - Feasibility of Peripherally Inserted Central Catheter Placement in COVID-19 Patients Isolated in the Intensive Care Unit of a Small Volume Center (291-Bed Hospital)
Min Chang Kang, Kyungwon Lee
Journal of Acute Care Surgery.2022; 12(3): 125. CrossRef - Prevalence of complications associated with the use of a peripherally inserted central catheter in newborns: A systematic review protocol
Edienne Rosângela Sarmento Diniz, Kleyton Santos de Medeiros, Richardson Augusto Rosendo da Silva, Ricardo Ney Cobucci, Angelo Giuseppe Roncalli, Raffaele Serra
PLOS ONE.2021; 16(7): e0255090. CrossRef - Ultrasound-guided insertion of peripherally inserted central catheter after anesthetic induction in children undergoing surgery for moyamoya disease - Thirty cases report-
Sang-Hwan Ji, Sol Ji Yoo, Sung-Ae Cho, Young-Eun Jang, Eun-Hee Kim, Ji-Hyun Lee, Jin-Tae Kim, Hee-Soo Kim
Anesthesia and Pain Medicine.2021; 16(3): 273. CrossRef - Comparing the accuracy and complications of peripherally inserted central catheter (PICC) placement using fluoroscopic and the blind pushing technique
Brendan Erskine, Pierre Bradley, Tim Joseph, Sabrina Yeh, Warren Clements
Journal of Medical Radiation Sciences.2021; 68(4): 349. CrossRef - Pneumothorax as a rare complication of peripherally inserted central catheter (PICC) in neonates: A case report study
Rasoul Goli, Sina Zafarmokhtarian, Mahmoodreza Ghalandari, Navid Babakeshi-sheytanabad, Sajjad Rostami, Hossna Farajollahi
International Journal of Surgery Case Reports.2021; 88: 106472. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite