
Articles
- Page Path
- HOME > Acute Crit Care > Volume 34(1); 2019 > Article
- Image in Critical Care Splenic Liquefaction after Splenic Artery Embolization
-
Byung Hee Kang

-
Acute and Critical Care 2018;34(1):92-94.
DOI: https://doi.org/10.4266/acc.2018.00073
Published online: November 13, 2018
Department of Trauma Surgery, Ajou University School of Medicine, Suwon, Korea
- Corresponding author Byung Hee Kang Department of Trauma Surgery, Ajou University School of Medicine, 206 World cup-ro, Yeongtong-gu, Suwon 16499, Korea Tel: +82-31-219-7764 Fax: +82-31-219-7781 E-mail: kbhname@gmail.com
• Received: February 20, 2018 • Revised: May 16, 2018 • Accepted: May 17, 2018
Copyright © 2019 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 6,133 Views
- 98 Download
Figure 1.Spleen laceration with bleeding and rib fracture were presented (white arrow). Liver laceration was also presented (black arrow).



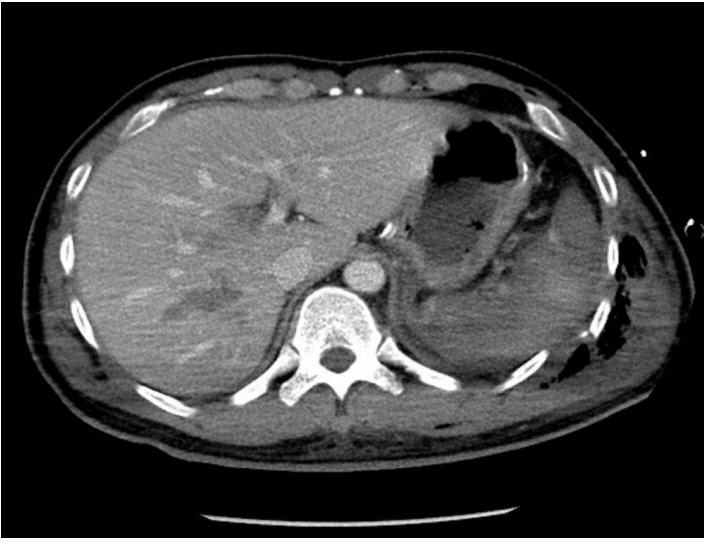
Figure 5.Eleven days post-embolization, splenic liquefaction was presented (white arrow). Liver laceration was improved (black arrow).


- 1. Crichton JC, Naidoo K, Yet B, Brundage SI, Perkins Z. The role of splenic angioembolization as an adjunct to nonoperative management of blunt splenic injuries: a systematic review and meta-analysis. J Trauma Acute Care Surg 2017;83:934-43.ArticlePubMed
- 2. Li ES, Mu JX, Ji SM, Li XM, Xu LB, Chai TC, et al. Total splenic artery embolization for splenic artery aneurysms in patients with normal spleen. World J Gastroenterol 2014;20:555-60.ArticlePubMedPMC
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 PubReader
PubReader ePub Link
ePub Link Cite
Cite






