Abstract
- In critically ill patients, disseminated intravascular coagulation (DIC) is a common and fatal hematological disorder. DIC is a physiological response to a variety of underlying stimuli that provoke generalized activation of the hemostatic mechanism and is common in septic patients and those with hematological or non-hematological malignant neoplasms. Bleeding is a common clinical feature, and diffuse or multiple-site mucocutaneous bleeding, such as petechia, ecchymosis and hemorrhage from gastrointestinal tract, is often seen. A 58-year-old male was recently diagnosed with intracranial hemorrhage (ICH) caused by DIC associated with sepsis. Mortality of ICH caused by DIC is very high because the underlying condition cannot be quickly treated. Awareness of the possibility of DIC developing in a critically ill patient and the need for immediate initiation of plasma or platelet replacement therapy are important. To the best of our knowledge, this is the first reported case of intracranial hemorrhage in a Korean patient with DIC associated with sepsis.
-
Keywords: disseminated intravascular coagulation; intracranial hemorrhage; sepsis
Disseminated intravascular coagulation (DIC) is a common clinicopathological syndrome in intensive-care patients. It may develop as a complication of infectious disease, an ABO-mismatched transfusion, trauma, an obstetric disease, a hematological malignancy, or a solid tumor.[1] Infectious disease, in particular sepsis and/or septic shock, is the most common clinical condition associated with DIC.[1-3] The common clinical manifestation is diffuse mucocutaneous bleeding; deep part bleeding has relatively rarely been reported. Intracranial hemorrhage (ICH) associated with non-traumatic DIC has been reported in non-infectious condition.[4,5] Here, we describe a case of fatal ICH caused by DIC secondary to sepsis.
Case Report
A 58-year-old male visited our emergency department complaining of a fever, chills, and sensations of paralysis in all extremities, without specific symptoms, 2 days in duration. He had no specific recent history of travel or unusual food consumption. He had undergone mitral valve replacement 12 years prior to treat mitral chordal rupture. Since then, he had taken warfarin to prevent thrombotic accidents, but had ceased taking the drug 5 months prior.
On admission, he was alert but lethargic and sweating. His initial vital signs were blood pressure 138/98 mmHg, heart rate 110 beats/min, respiratory rate 18 breaths/min, body temperature 38.3ºC, and pulse oximetry 98% on room air. A complete blood count showed leukocytes, 20,460/mm3 (segmented neutrophils 96.5%), hemoglobin, 12.7 g/dL, hematocrit 36.9%, and platelets 107,000/mm3. Blood chemistry was as follows: blood urea nitrogen (BUN) 19.5 mg/dL, creatinine 1.20 mg/dL, aspartate transaminase 25 U/L, alanine transaminase 19 U/L, total bilirubin 0.99 mg/dL, amylase 80 U/L, lipase 15 U/L, alkaline phosphatase 41 IU/L, lactate dehydrogenase 1,049 U/L, creatine phosphokinase 91 U/L, C-reactive protein 7.34 mg/dL, and procalcitonin 64.65 ng/mL. The prothrombin time (PT), international normalized ratio (INR), and activated partial thromboplastin time (aPTT) were 15.8 s, 1.31, and 31.9 s, respectively. Urine examination revealed 1+ proteinuria, pyuria (10-20 leukocytes under a high-power field), and hematuria (30-99 red blood cells under a high-power field). Electrocardiography and echocardiography demonstrated no definite evidence of endocarditis. On echocardiography, the prosthetic mitral valve was observed to be functioning well.
On the initial chest radiograph, his prior history of sternotomy and mitral valvular ring replacement were evident, but no definite parenchymal lung lesion was noted (Fig. 1A). We performed abdominopelvic computed tomography (CT) to determine the origin of the sepsis. The scan raised the suspicion of acute cholecystitis (Fig. 1B), but few correlations with his symptoms were evident. To rule out a cerebrovascular accident, the brain was subjected to CT and magnetic resonance imaging (MRI). No definite abnormalities were evident (Fig. 2). Blood, urine, sputum, and cerebrospinal fluid samples were immediately sent for microbial culture. As an infectious origin of disease could not be definitely established, ceftriaxone and metronidazole were given intravenously to counter any biliary tract infection.
Approximately 15 hours later, the patient developed chest tightness and dyspnea. His blood pressure was 90/60 mmHg, heart rate 120 beats/min, and respiratory rate 30 breaths/min. No definite motor weakness was evident upon neurological examination. Follow up laboratory findings showed, arterial blood gas analysis pH 7.42, PaCO2 25.4 mm Hg, PaO2 71.7 mm Hg, HCO3–17.1 mmol/L, SaO2 95%, and lactate level was 4.44 mmol/L. The platelet count had fallen to 43,000/mm3, and BUN and creatinine levels had increased to 34.7 mg/dL and 1.57 mg/dL, respectively. The PT, INR, aPTT, fibrinogen level, and D-dimer level were elevated to 20.7 s, 1.71, 77.0 s, 534 mg/dL, and 43,300 ng/mL, respectively.
The patient developed a confused mentality and sleepiness; this is the typical medical course of septic shock associated with DIC. Concentrated platelets and thawed freshly frozen plasma were transfused immediately. Fluid replacement, norepinephrine, and vasopressin were prescribed to treat the septic shock. The antibiotics were changed to meropenem and vancomycin. However, the tachypnea persisted and his mental status deteriorated further. Eventually, invasive mechanical ventilation was applied. About 1 hour later, an abnormal pupil light reflex was detected. Follow-up brain CT revealed acute intracerebral hemorrhage of the left frontal lobe with intraventricular hemorrhages throughout all of the ventricles (Fig. 3). To ensure proper management of the hemorrhages, the patient was referred to a neurosurgeon. However, he was in an inoperable condition because of his septic shock and DIC. The patient died on the third hospital day from ICH and septic shock. Blood and urine culture data obtained 1 day later confirmed the presence of methicillin-resistant Staphylococcus aureus.
Discussion
DIC is a physiological response to a variety of underlying stimuli that provoke generalized activation of the hemostatic mechanism. It features ongoing systemic activation of blood coagulation, impaired synthesis and increased degradation of coagulation proteins and protease inhibitors, and exhaustion of coagulation factors and platelets. These changes can cause severe bleeding from various sites.[1,3] It is classically characterized by the simultaneous development of widespread (micro)vascular thromboses, thereby compromising the blood supply to many organs, in turn contributing to organ failure.[1] It has also been shown to be an independent and relatively strong predictor of organ dysfunction and mortality in patients with sepsis and severe trauma.[6, 7]
DIC develops in about 35% of patients with severe sepsis. [6,7] Mortality is higher in patients with DIC (40-46.2%) than in those without it (22.2-26.5%).[8] Thus, the prognosis of sepsis is affected by the presence of DIC. Trauma, particularly neurotrauma, is also frequently associated with the condition, which is more commonly observed in trauma patients with systemic inflammatory response syndrome.[9] Evidence indicates that inflammatory cytokines play central roles in DIC in both trauma patients and septic patients. In fact, the systemic cytokine profiles of septic patients and trauma patients are nearly identical.[10] If neurological changes (including disturbances of consciousness, impaired cognitive function, personality changes, lack of concentration, and depressive symptoms) develop in an intensive-care patient, the common causes are neurotrauma, delirium, and sepsis. Encephalopathy and polyneuropathy frequently develop in septic patients; these conditions are often grouped as “septic encephalopathy.” Such encephalopathy is diffuse, appears early, is often severe, but resolves quickly upon successful treatment of the sepsis.[11,12]
Most common cause of non-traumatic ICH is hypertensive damage to blood vessel (e.g., hypertension, eclampsia). But, there are other causes such as autoregulatory dysfunction with excessive cerebral blood flow (e.g., reperfusion injury, hemorrhagic transformation, cold exposure), rupture of an aneurysm or arteriovenous malformation and altered hemostasis (e.g., thrombolysis, anticoagulation, bleeding diathesis).[5] In our case, widespread thrombin generation and clotting results in coagulopathies and bleeding tendency from depletion of coagulation factors, platelets and secondary fibrinolysis with resultant hemorrhage.[13]
ICH associated with non-traumatic DIC is often accompanied by encephalopathy.[11,14] The incidence of ICH in intensive-care populations with DIC remains unknown. In many patients with life-threatening sepsis who experience progressive organ failure, transport to the imaging suite such as CT or MRI is often postponed until ventilatory and vital signs become stabilized.[11]
ICH associated with DIC has been reported in non-sepsis patients.[4,5,15,16] Radiological findings of subdural hematoma, subarachnoid and massive lobar hemorrhages, and hemorrhagic infarcts (often in association with venous sinus thrombosis), have been occasionally described.[5,15-17] However, reports on ICH associated with DIC caused by sepsis are rare in English-language literature.[11,18] Wijdicks et al.[11] reported a case of subcortical hemorrhage in two patients with DIC associated with sepsis; both patients died about 2 weeks after sudden-onset hemorrhage. Neligan et al.[18] reported a case with microhemorrhages caused by acute DIC that developed secondary to sepsis; the patient had a history of sickle cell disease and developed extensive microhemorrhages both supratentorially and infratentorially. An ICH associated with DIC and sepsis has not been previously described in Korea. Thus, to the best of our knowledge, this is the first such report. Our patient had symptoms of a neurological deficit suggestive of a cerebral vascular accident (cerebral infarction or cerebral hemorrhage). We postulate that the ICH was a consequence of the DIC because hemorrhage was not observed at the time of admission and the patient had no history of trauma at or after admission.
Although we diagnosed ICH associated with DIC, our surgical management options were very limited. The patient was poorly operable because of his hematological instability. DIC is a severe, often fatal complication of sepsis, and should be diagnosed as soon as possible.[19] If blood tests imply that a septic patient has DIC accompanied by ICH, plasma or platelet substitution therapy and sepsis treatment should be initiated as soon as possible. As DIC is characterized by extensive activation of coagulation, anticoagulant treatment may be a reasonable approach.[1,3,20]
In conclusion, intensivist should be aware that ICH can develop in patients with DIC caused by sepsis. It is essential to monitor mental status; if this changes, conscientious efforts should be made to identify the cause.
NOTES
-
No potential conflict of interest relevant to this article was reported.
Fig. 1.Initial chest radiography and abdominopelvic computed tomography. (A) The chest radiography revealed a history of a median sternotomy and replacement of a mitral valvular ring. (B) Abdominopelvic computed tomography revealed a few tiny stones with mild distension without wall thickening of the gall bladder.

Fig. 2.Initial brain computed tomography and magnetic resonance imaging. (A, B) Computed tomography revealed cerebromalacia with diffuse brain atrophy in the right lower frontal and left parietal areas. (C, D) Magnetic resonance imaging (fluid-attenuated inversion recovery) revealed encephalomalacic change in the right frontal and left parietal regions, the basal ganglia, and both cerebellar hemispheres.

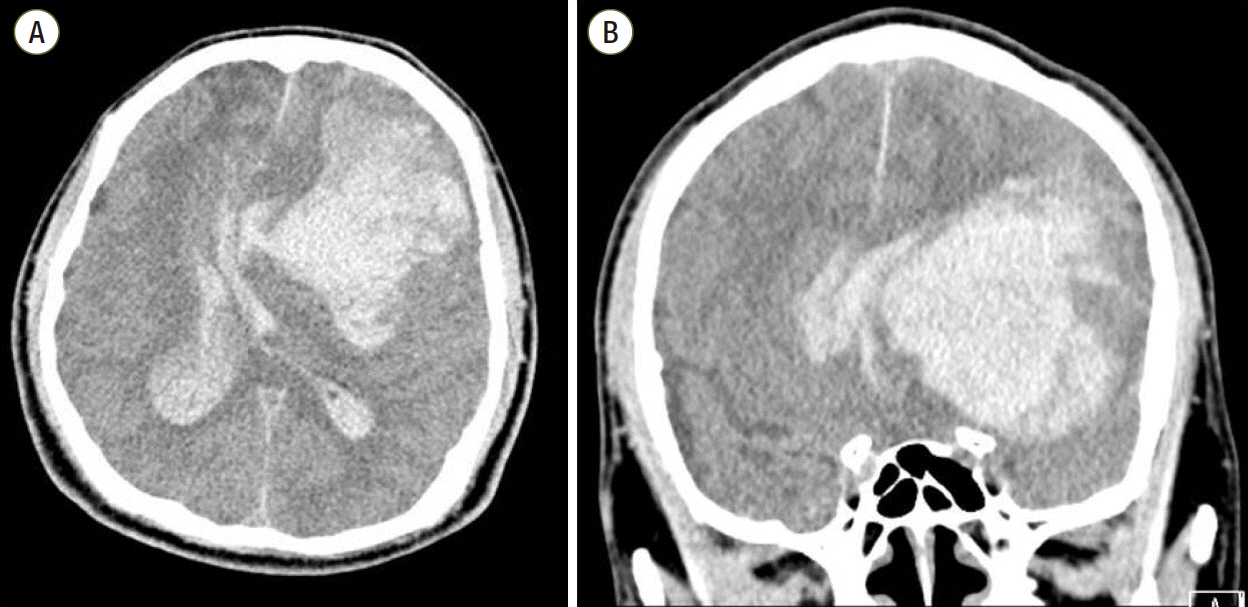
Fig. 3.On hospital day 2, (A, B) brain computed tomography revealed an acute intracranial hemorrhage in the left frontal region, with a mass effect, and intraventricular hemorrhages evident over all ventricles.
References
- 1. Levi M, Ten Cate H. Disseminated intravascular coagulation. N Engl J Med 1999;341:586-92.ArticlePubMed
- 2. Fourrier F, Chopin C, Goudemand J, Hendrycx S, Caron C, Rime A, et al. Septic shock, multiple organ failure, and disseminated intravascular coagulation. Compared patterns of antithrombin III, protein C, and protein S deficiencies. Chest 1992;101:816-23.ArticlePubMed
- 3. Levi M. Disseminated intravascular coagulation. Crit Care Med 2007;35:2191-5.ArticlePubMed
- 4. Park TH, Kim YB, Lee KH. A case of intracranial hemorrhage associated with disseminated intravascular coagulation caused by dissecting aortic aneurysm. Korean J Stroke 2004;6:124.
- 5. Kawakami Y, Ueki K. Chikama M, Shimamura Y, Naito T. Intracranial hemorrhage associated with nontraumatic disseminated intravascular coagulation--report of four cases. Neurol Med Chir (Tokyo) 1990;30:610-7.ArticlePubMed
- 6. Bakhtiari K, Meijers JC, de Jonge E, Levi M. Prospective validation of the International Society of Thrombosis and Haemostasis scoring system for disseminated intravascular coagulation. Crit Care Med 2004;32:2416-21.ArticlePubMed
- 7. Dhainaut JF, Yan SB, Joyce DE, Pettilä V, Basson B, Brandt JT, et al. Treatment effects of drotrecogin alfa (activated) in patients with severe sepsis with or without overt disseminated intravascular coagulation. J Thromb Haemost 2004;2:1924-33.ArticlePubMed
- 8. Warren BL, Eid A, Singer P, Pillay SS, Carl P, Novak I, et al. Caring for the critically ill patient. High-dose antithrombin III in severe sepsis: a randomized controlled trial. JAMA 2001;286:1869-78.ArticlePubMed
- 9. Gando S. Disseminated intravascular coagulation in trauma patients. Semin Thromb Hemost 2001;27:585-92.ArticlePubMed
- 10. Gando S, Nakanishi Y, Tedo I. Cytokines and plasminogen activator inhibitor-1 in posttrauma disseminated intravascular coagulation: relationship to multiple organ dysfunction syndrome. Crit Care Med 1995;23:1835-42.ArticlePubMed
- 11. Wijdicks EF, Silbert PL, Jack CR, Parisi JE. Subcortical hemorrhage in disseminated intravascular coagulation associated with sepsis. AJNR Am J Neuroradiol 1994;15:763-5.PubMedPMC
- 12. Young GB, Bolton CF, Austin TW, Archibald YM, Gonder J, Wells GA. The encephalopathy associated with septic illness. Clin Invest Med 1990;13:297-304.PubMed
- 13. Rubin RN, Colman RW. Disseminated intravascular coagulation. Approach to treatment. Drugs 1992;44:963-71.ArticlePubMed
- 14. Schwartzman RJ, Hill JB. Neurologic complications of disseminated intravascular coagulation. Neurology 1982;32:791-7.ArticlePubMed
- 15. Furui T, lchihara K, Ikeda A, lnao S, Hirai N, Yoshida J, et al. Subdural hematoma associated with disseminated in travascular coagulation in patients with advanced cancer. J Neurosurg 1983;58:398-401.ArticlePubMed
- 16. Yokota H, Kobayashi S, Nakazawa S, Yano M, Yamamoto Y, Otsuka T. Clinical studies of intracranial lesions of disseminated intravascular coagulation syndrome by computerized tomography. Neurol Med Chir (Tokyo) 1986;26:870-6.ArticlePubMed
- 17. Buonanno FS, Cooper MR, Moody DM, Laster DW, Ball MR, Toole JF. Neuroradiologic aspects of cerebral disseminated intravascular coagulation. AJNR Am J Neuroradiol 1980;1:245-50.PubMedPMC
- 18. Neligan A, Rajakulendran S, Nortley R, Manji H. Extensive cerebral microhemorrhages caused by acute disseminated intravascular coagulation secondary to sepsis. JAMA Neurol 2014;71:510-1.ArticlePubMed
- 19. Hardaway RM, William CH, Vasquez Y. Disseminated intravascular coagulation in sepsis. Semin Thromb Hemost 2001;27:577-83.ArticlePubMed
- 20. Levi M, Toh CH, Thachil J, Watson HG. Guidelines for the diagnosis and management of disseminated intravascular coagulation. British Committee for Standards in Haematology. Br J Haematol 2009;145:24-33.ArticlePubMed
Citations
Citations to this article as recorded by

- Abdominal mass in a septic infant: Case of a fatal intraluminal intestinal hematoma
Mana Taweevisit, Paul Scott Thorner
Pediatric Hematology Oncology Journal.2021; 6(3): 139. CrossRef - Perforated Mesenteric Cyst with Sepsis and Neurological Complication in a 9 Month Old Child
Mandal KC, Saha D, Halder P, Chakraborty P, Debnath B, Mukhopadhyay B
Asploro Journal of Pediatrics and Child Health.2020; 2(1): 30. CrossRef



 PubReader
PubReader ePub Link
ePub Link Cite
Cite



