Articles
- Page Path
- HOME > Acute Crit Care > Volume 38(1); 2023 > Article
-
Review Article
Basic science and research Extracorporeal circulation models in small animals: beyond the limits of preclinical research -
Mukhammad Kayumov1,2,3
 , Reverien Habimana3,4, Dowan Kim2,3, Francis O Obiweluozor2,3, In Seok Jeong2,3, Hwa Jin Cho3,5
, Reverien Habimana3,4, Dowan Kim2,3, Francis O Obiweluozor2,3, In Seok Jeong2,3, Hwa Jin Cho3,5 -
Acute and Critical Care 2023;38(1):1-7.
DOI: https://doi.org/10.4266/acc.2023.00381
Published online: February 28, 2023
1Department of Medical Science, Chonnam National University Graduate School, Gwangju, Korea
2Department of Thoracic and Cardiovascular Surgery, Chonnam National University, Chonnam National University Hospital Medical School, Gwangju, Korea
3Extracorporeal Circulation Research Team, Chonnam National University Hospital, Gwangju, Korea
4Department of Biomedical Sciences, Chonnam National University Graduate School, Chonnam National University Medical School, Gwangju, Korea
5Department of Pediatrics, Chonnam National University Children’s Hospital, Chonnam National University Medical School, Gwangju, Korea
- Corresponding author: Hwa Jin Cho Department of Pediatrics, Chonnam National University Children’s Hospital, Chonnam National University Medical School and Extracorporeal Circulation Research Team, Chonnam National University Hospital, 42 Jebong-ro, Dong-gu, Gwangju 61469, Korea Tel: +82-62-220-6646, Fax: +82-62-222-6103, Email: chhj98@gmail.com
Copyright © 2023 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
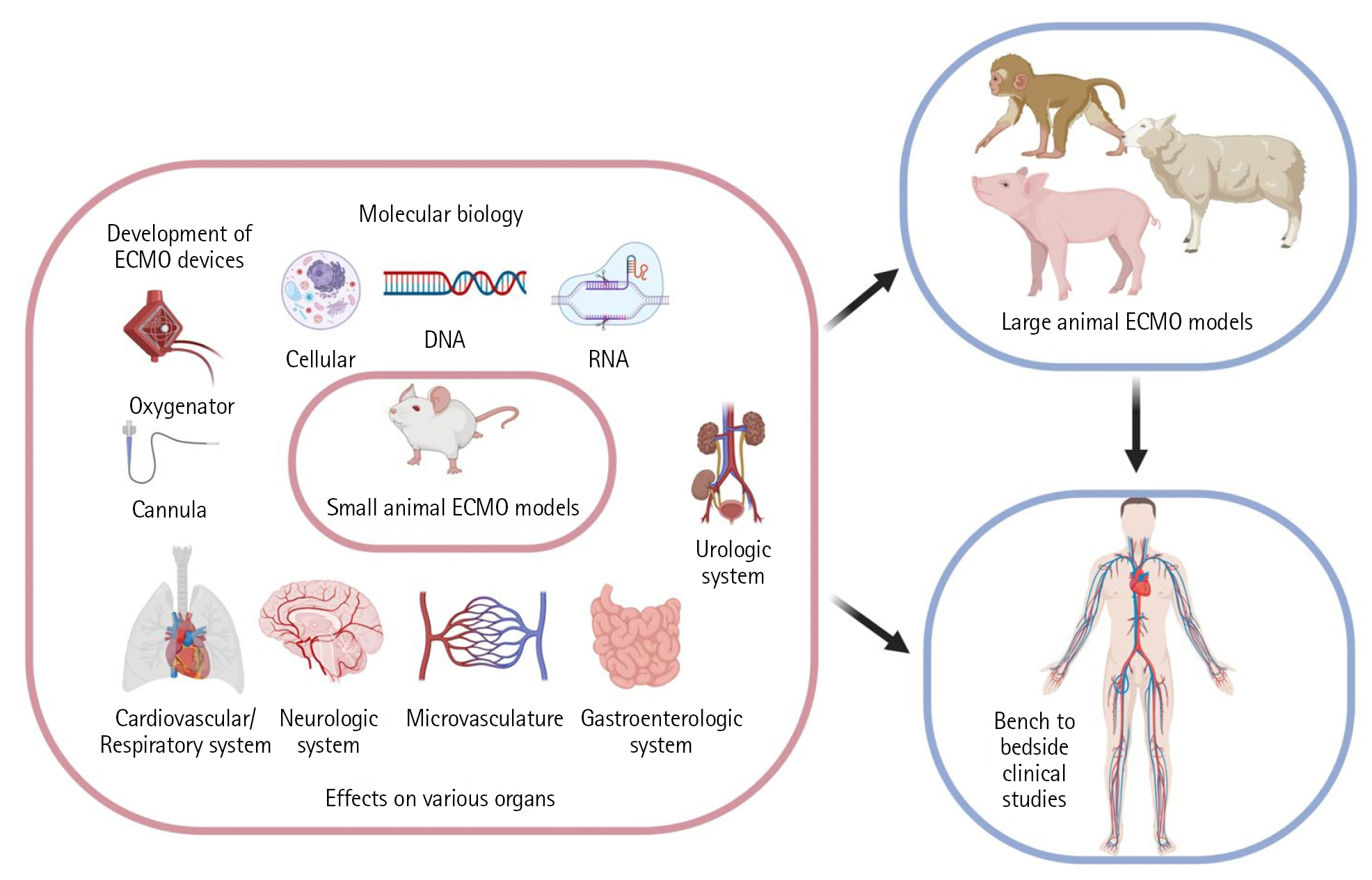
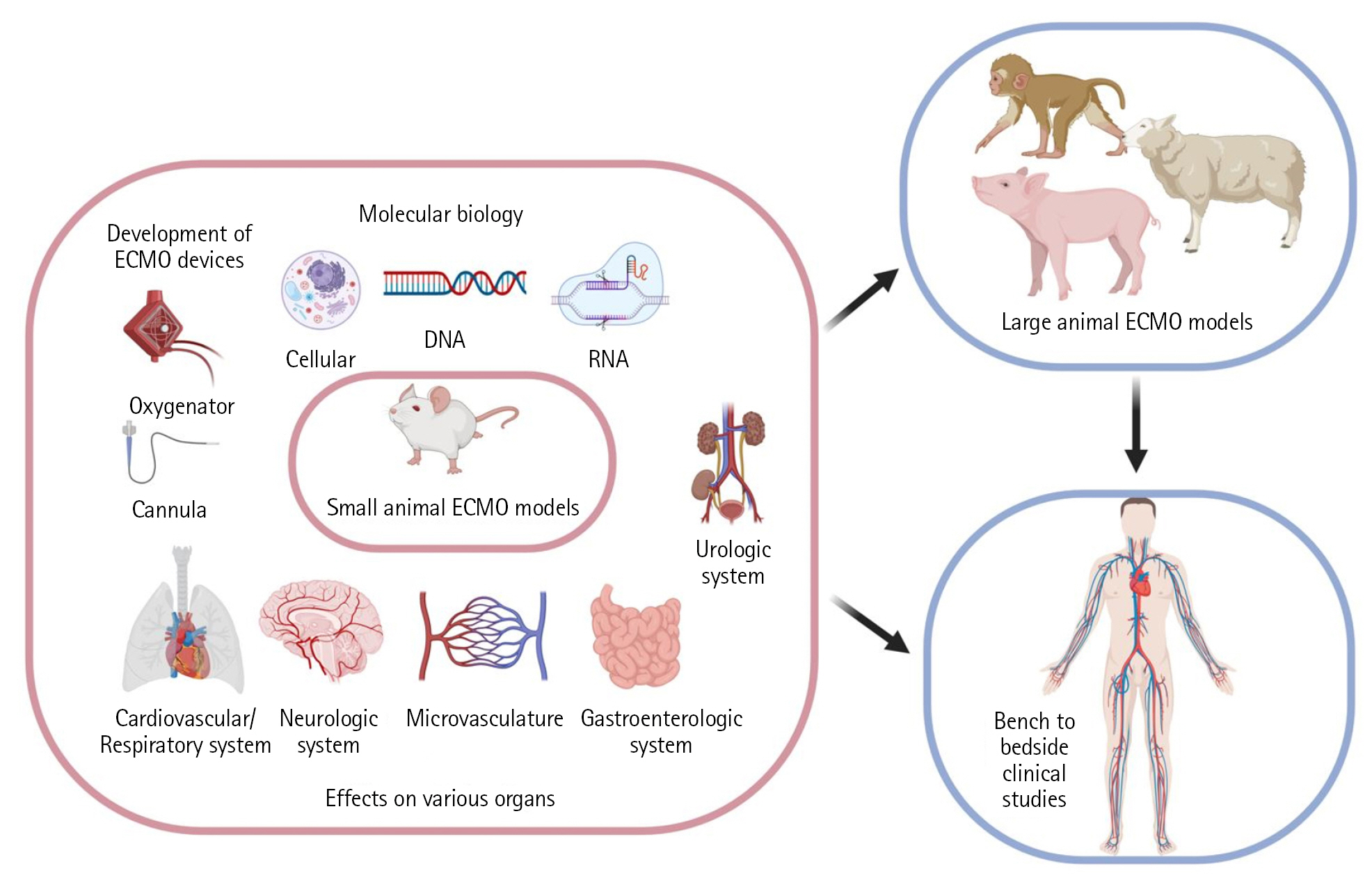
- Extracorporeal membrane oxygenation (ECMO) use has remarkably increased in recent years. Although ECMO has become essential for patients with refractory cardiac and respiratory failure, extracorporeal circulation (ECC) is associated with significant complications. Small-animal models of ECC have been developed and widely used to better understand ECC-induced pathophysiology. This review article summarizes the development of small-animal ECC models, including the animal species, circuit configuration, priming, perioperative procedures, cannulation, and future perspectives of small-animal ECMO models.
INTRODUCTION
MODEL ESTABLISHMENT
Species and weight of models
Circuit configuration
Priming
Perioperative procedures
Cannulation
FUTURE PERSPECTIVES OF SMALL-ANIMAL ECMO MODELS: AFFORDABLE IN VIVO STUDIES
CONCLUSIONS
HIGHLIGHTS
-
CONFLICT OF INTEREST
Hwa Jin Cho Dong-Ick Shin is an editorial board member of the journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: HJC, DK, FOO, ISJ. Data curation: MK, RH. Formal analysis: ISJ. Funding acquisition: HJC, DK, ISJ. Methodology: MK, RH. Project administration: MK, ISJ. Visualization: HJC, RH, ISJ. Writing–original draft: MK, HJC. Writing–review & editing: all authors.
NOTES
Acknowledgments
| Study | Year | Species | ECC type | Duration of ECC (min) | Drainage catheter | Perfusion catheter | Priming volume (ml) | Purpose of study |
|---|---|---|---|---|---|---|---|---|
| Popovic et al. [14] | 1968 | Rat | VA/CPB | 70 | PE 200 tubing (ID: 1.4 mm) | PE 90 tubing (0.86 mm) | 13.7 | Model development |
| Alexander et al. [15] | 1983 | Rat | VA/CPB | 360 | NA | NA | 8.7 | Device development |
| Grocott et al. [16 | 2001 | Rat | VA/CPB | 60 | Dual-stage venous cannula (4.5 Fr) | Angiocatheter (20G) | 45 | Neuropathophysiology |
| Dong et al. [17] | 2005 | Rat | VA/CPB | 60 | Angiocatheter (16G) | Angiocatheter (22G) | 16 | Model establishment |
| Ordodi et al. [18] | 2008 | Rat | AA/CPB | 120 | Angiocatheter (24G) | Angiocatheter (24G) | 20 | Device development |
| Huang et al. [19] | 2007 | Rat | VA/CPB | 60 | Angiocatheter (16G) | Angiocatheter (22G) | 10 | Pathophysiology |
| Jungwirth et al. [20] | 2007 | Rat | VA/CPB | 90 | Dual-stage venous cannula (4.5 Fr) | Angiocatheter (20G) | 16 | Neuropathophysiology |
| Qing et al. [21] | 2011 | Rat | VA/CPB | 90 | Dual-stage venous cannula (4.5 Fr) | Angiocatheter (20G) | 18 | Neuropathophysiology |
| Waterbury et al. [22] | 2011 | Rat | VA/CPB | 80 | Angiocatheter (16G) | Angiocatheter (20G) | 12 | CPB and DHCA development |
| Rungatscher et al. [12] | 2012 | Rat | VA/CPB | 90 | Angiocatheter (16G) | Angiocatheter (18G) | 10.5 | Pharmacology |
| Mackensen et al. [23] | 2001 | Rat | VA/CPB | 150 | Angiocatheter (16G) | Angiocatheter (22G) | 10 | Model establishment |
| Fujii et al. [24] | 2013 | Rat | VA/CPB | 60 | Angiocatheter (16G) | Polyethylene tubing (NA) | 15 | Pharmacology |
| Fujii et al. [25] | 2013 | Rat | VA/CPB | 120 | Angiocatheter (16G) | Polyethylene tubing (NA) | 15 | CPB pathophysiology |
| Ali et al. [1] | 2014 | Rat | VA/ECMO | 10 | Angiocatheter (20G) | Angiocatheter (24G) | 8 | Model establishment |
| Luo et al. [2] | 2015 | Mouse | VA/ECC | 30 | Angiocatheter (24G) | Angiocatheter (24G) | 0.4 | ECC-induced SIRS |
| Du et al. [26] | 2016 | Mouse | NA | NA | NA | NA | NA | ECMO treatment in pneumonia |
| Chang et al. [7] | 2017 | Rat | VA/CPB, ECLS | 30 | Angiocatheter (14G) | Angiocatheter (20G) | 20 | CPB pathophysiology |
| Bianchini et al. [10] | 2018 | Rat | VA/CPB | 60 | Angiocatheter (16G) | Angiocatheter (22G) | 10 | Pharmacology |
| Madrahimov et al. [27] | 2018 | Mouse | VA/CPB | 90 | Polyurethane tube (2 Fr) | Angiocatheter (27G) | 0.85 | Model establishment |
| Xie et al. [28] | 2012 | Rat | VA | 120 | Trocar (24G) | Trocar (24G) | NA | Platelet therapy with CPB |
| Natanov et al. [29] | 2019 | Mouse | VV/ECMO | 240 | Double-lumen silicone catheter (2 Fr) | Double-lumen silicone-based catheter (2 Fr) | 0.5 | VV-ECMO induced pathophysiology |
| Cho et al. [13] | 2021 | Rat | VA+VV/ECMO | 120 | Modified neonatal feeding tube (5 Fr) | Angiocatheter (24G) | 14 | Immunology |
| Kayumov et al. [30] | 2022 | Rat | VA/ECMO | 120 | Modified neonatal feeding tube (5 Fr) | Angiocatheter (24G) | 14 | Septic shock, pressure-volume change |
ECC: extracorporeal circulation; VA: veno-arterial; CPB: cardiopulmonary bypass; NA: not applicable; AA: arterio-arterial; DHCA: deep hypothermic circulatory arrest; ECMO: extracorporeal membrane oxygenation; SIRS: systemic inflammatory response syndrome; ECLS: extracorporeal life support; VV: veno-venous.
- 1. Ali AA, Downey P, Singh G, Qi W, George I, Takayama H, et al. Rat model of veno-arterial extracorporeal membrane oxygenation. J Transl Med 2014;12:37. ArticlePubMedPMC
- 2. Luo S, Tang M, Du L, Gong L, Xu J, Chen Y, et al. A novel minimal invasive mouse model of extracorporeal circulation. Mediators Inflamm 2015;2015:412319. ArticlePubMedPMCPDF
- 3. Tramm R, Ilic D, Davies AR, Pellegrino VA, Romero L, Hodgson C. Extracorporeal membrane oxygenation for critically ill adults. Cochrane Database Syst Rev 2015;1:CD010381. ArticlePubMed
- 4. Bateman RM, Sharpe MD, Jagger JE, Ellis CG, Solé-Violán J, López-Rodríguez M, et al. 36th International Symposium on Intensive Care and Emergency Medicine : Brussels, Belgium. 15-18 March 2016. Crit Care 2016;20(Suppl 2):94. PubMedPMC
- 5. Abrams D, Bacchetta M, Brodie D. When the momentum has gone: what will be the role of extracorporeal lung support in the future? Curr Opin Crit Care 2018;24:23-8.ArticlePubMed
- 6. Raleigh L, Ha R, Hill C. Extracorporeal membrane oxygenation applications in cardiac critical care. Semin Cardiothorac Vasc Anesth 2015;19:342-52.ArticlePubMedPDF
- 7. Chang RW, Luo CM, Yu HY, Chen YS, Wang CH. Investigation of the pathophysiology of cardiopulmonary bypass using rodent extracorporeal life support model. BMC Cardiovasc Disord 2017;17:123. ArticlePubMedPMCPDF
- 8. Cresce GD, Walpoth BH, Mugnai D, Innocente F, Rungatscher A, Luciani GB, et al. Validation of a rat model of cardiopulmonary bypass with a new miniaturized hollow fiber oxygenator. ASAIO J 2008;54:514-8.ArticlePubMed
- 9. Giridharan GA, Lee TJ, Ising M, Sobieski MA, Koenig SC, Gray LA, et al. Miniaturization of mechanical circulatory support systems. Artif Organs 2012;36:731-9.ArticlePubMedPMC
- 10. Bianchini EP, Sebestyen A, Abache T, Bourti Y, Fontayne A, Richard V, et al. Inactivated antithombin as anticoagulant reversal in a rat model of cardiopulmonary bypass: a potent and potentially safer alternative to protamine. Br J Haematol 2018;180:715-20.ArticlePubMedPDF
- 11. Yuan L, Su D, Liu X, Lu H, Li Y, Tong S. Cerebral blood flow changes during rat cardiopulmonary bypass and deep hypothermic circulatory arrest model: a preliminary study. Annu Int Conf IEEE Eng Med Biol Soc 2013;2013:1807-10.PubMed
- 12. Rungatscher A, Linardi D, Tessari M, Menon T, Luciani GB, Mazzucco A, et al. Levosimendan is superior to epinephrine in improving myocardial function after cardiopulmonary bypass with deep hypothermic circulatory arrest in rats. J Thorac Cardiovasc Surg 2012;143:209-14.ArticlePubMed
- 13. Cho HJ, Kayumov M, Kim D, Lee K, Onyekachi FO, Jeung KW, et al. Acute immune response in venoarterial and venovenous extracorporeal membrane oxygenation models of rats. ASAIO J 2021;67:546-53.ArticlePubMed
- 14. Popovic P, Horecky J, Popovic VP. Hypothermic cardiopulmonary bypass in white rats. Ann Surg 1968;168:298-301.ArticlePubMedPMC
- 15. Alexander B, Al Ani HR. Prolonged partial cardiopulmonary bypass in rats. J Surg Res 1983;35:28-34.ArticlePubMed
- 16. Grocott HP, Mackensen GB, Newman MF, Warner DS. Neurological injury during cardiopulmonary bypass in the rat. Perfusion 2001;16:75-81.ArticlePDF
- 17. Dong GH, Xu B, Wang CT, Qian JJ, Liu H, Huang G, et al. A rat model of cardiopulmonary bypass with excellent survival. J Surg Res 2005;123:171-5.ArticlePubMed
- 18. Ordodi VL, Paunescu V, Ionac M, Sandesc D, Mic AA, Tatu CA, et al. Artificial device for extracorporeal blood oxygenation in rats. Artif Organs 2008;32:66-70.ArticlePubMed
- 19. Huang H, Yin R, Zhu J, Feng X, Wang C, Sheng Y, et al. Protective effects of melatonin and N-acetylcysteine on hepatic injury in a rat cardiopulmonary bypass model. J Surg Res 2007;142:153-61.ArticlePubMed
- 20. Jungwirth B, Kellermann K, Blobner M, Schmehl W, Kochs EF, Mackensen GB. Cerebral air emboli differentially alter outcome after cardiopulmonary bypass in rats compared with normal circulation. Anesthesiology 2007;107:768-75.ArticlePubMedPDF
- 21. Qing M, Shim JK, Grocott HP, Sheng H, Mathew JP, Mackensen GB. The effect of blood pressure on cerebral outcome in a rat model of cerebral air embolism during cardiopulmonary bypass. J Thorac Cardiovasc Surg 2011;142:424-9.ArticlePubMed
- 22. Waterbury T, Clark TJ, Niles S, Farivar RS. Rat model of cardiopulmonary bypass for deep hypothermic circulatory arrest. J Thorac Cardiovasc Surg 2011;141:1549-51.ArticlePubMed
- 23. Mackensen GB, Sato Y, Nellgård B, Pineda J, Newman MF, Warner DS, et al. Cardiopulmonary bypass induces neurologic and neurocognitive dysfunction in the rat. Anesthesiology 2001;95:1485-91.ArticlePubMedPDF
- 24. Fujii Y, Shirai M, Inamori S, Shimouchi A, Sonobe T, Tsuchimochi H, et al. Insufflation of hydrogen gas restrains the inflammatory response of cardiopulmonary bypass in a rat model. Artif Organs 2013;37:136-41.ArticlePubMed
- 25. Fujii Y, Shirai M, Tsuchimochi H, Pearson JT, Takewa Y, Tatsumi E, et al. Hyperoxic condition promotes an inflammatory response during cardiopulmonary bypass in a rat model. Artif Organs 2013;37:1034-40.ArticlePubMed
- 26. Du Q, Shen Y, Yu J, Huang S, Pan S. Extracorporeal membrane oxygenation (EMCO) is an optimal method to cure the pneumonia caused by endotoxin in mice. Int J Clin Exp Pathol 2016;9:10796-802.
- 27. Madrahimov N, Boyle EC, Gueler F, Goecke T, Knöfel AK, Irkha V, et al. Novel mouse model of cardiopulmonary bypass. Eur J Cardiothorac Surg 2018;53:186-93.ArticlePubMed
- 28. Xie XJ, Tao KY, Tang ML, Du L, An Q, Lin K, et al. Establishment and evaluation of extracorporeal circulation model in rats. Sichuan Da Xue Xue Bao Yi Xue Ban 2012;43:770-4.PubMed
- 29. Natanov R, Khalikov A, Gueler F, Maus U, Boyle EC, Haverich A, et al. Four hours of veno-venous extracorporeal membrane oxygenation using bi-caval cannulation affects kidney function and induces moderate lung damage in a mouse model. Intensive Care Med Exp 2019;7:72. ArticlePubMedPMCPDF
- 30. Kayumov M, Kim D, Raman S, MacLaren G, Jeong IS, Cho HJ. Combined effects of sepsis and extracorporeal membrane oxygenation on left ventricular performance in a murine model. Sci Rep 2022;12:22181. ArticlePubMedPMCPDF
- 31. Madrahimov N, Natanov R, Boyle EC, Goecke T, Knöfel AK, Irkha V, et al. Cardiopulmonary bypass in a mouse model: a novel approach. J Vis Exp 2017;(127):56017. ArticlePubMedPMC
- 32. Riera J, Argudo E, Ruiz-Rodríguez JC, Ferrer R. Extracorporeal membrane oxygenation for adults with refractory septic shock. ASAIO J 2019;65:760-8.ArticlePubMed
- 33. Gaylor JD. Membrane oxygenators: current developments in design and application. J Biomed Eng 1988;10:541-7.ArticlePubMed
- 34. Clark RE, Beauchamp RA, Magrath RA, Brooks JD, Ferguson TB, Weldon CS. Comparison of bubble and membrane oxygenators in short and long perfusions. J Thorac Cardiovasc Surg 1979;78:655-66.ArticlePubMed
- 35. Berner M, Clément D, Stadelmann M, Kistler M, Boone Y, Carrel TP, et al. Development of an ultra mini-oxygenator for use in low-volume, buffer-perfused preparations. Int J Artif Organs 2012;35:308-15.ArticlePubMedPDF
- 36. Iwahashi H, Yuri K, Nosé Y. Development of the oxygenator: past, present, and future. J Artif Organs 2004;7:111-20.ArticlePubMedPDF
- 37. Obstals F, Vorobii M, Riedel T, de Los Santos Pereira A, Bruns M, Singh S, et al. Improving hemocompatibility of membranes for extracorporeal membrane oxygenators by grafting nonthrombogenic polymer brushes. Macromol Biosci 2018;18:1700359. ArticlePDF
- 38. Lebreton G, Tamion F, Bessou JP, Doguet F. Cardiopulmonary bypass model in the rat: a new minimal invasive model with a low flow volume. Interact Cardiovasc Thorac Surg 2012;14:642-4.ArticlePubMedPMC
References
Figure & Data
References
Citations
- Venoarterial Extracorporeal Membrane Oxygenation Implementation in Septic Shock Rat Model
Tianlong Wang, Mingru Zhang, Wenhao Dong, Jing Wang, Han Zhang, Yuefu Wang, Bingyang Ji
ASAIO Journal.2024;[Epub] CrossRef - Multiorgan recovery in a cadaver body using mild hypothermic ECMO treatment in a murine model
Nodir Madrahimov, Vitalii Mutsenko, Ruslan Natanov, Dejan Radaković, André Klapproth, Mohamed Hassan, Mathias Rosenfeldt, Florian Kleefeldt, Ivan Aleksic, Süleyman Ergün, Christoph Otto, Rainer G. Leyh, Constanze Bening
Intensive Care Medicine Experimental.2023;[Epub] CrossRef - Post-Mortem Extracorporeal Membrane Oxygenation Perfusion Rat Model: A Feasibility Study
Matthias Manfred Deininger, Carl-Friedrich Benner, Lasse Johannes Strudthoff, Steffen Leonhardt, Christian Simon Bruells, Gernot Marx, Christian Bleilevens, Thomas Breuer
Animals.2023; 13(22): 3532. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite