Articles
- Page Path
- HOME > Acute Crit Care > Volume 38(1); 2023 > Article
-
Original Article
Nursing Theoretical definition of nurse–conscious mechanically ventilated patient communication: a scoping review with qualitative content analysis -
Arezoo Mohamadkhani Ghiasvand1
 , Meimanat Hosseini2, Foroozan Atashzadeh-Shoorideh3
, Meimanat Hosseini2, Foroozan Atashzadeh-Shoorideh3 -
Acute and Critical Care 2023;38(1):8-20.
DOI: https://doi.org/10.4266/acc.2022.01039
Published online: February 27, 2023
1Student Research Committee, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Department of Community Health Nursing, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3Department of Psychiatric Nursing and Management, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
- Corresponding author: Meimanat Hosseini Department of Community Health Nursing, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Vali Asr Ave, Niayesh Cross Rd, Niayesh Complex, Tehran 1985717443, Iran Tel: +98-21-88655366 Fax: +98-21-88655363 Email: m_hoseini@sbmu.ac.ir
Copyright © 2023 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,045 Views
- 184 Download
- 2 Crossref
Abstract
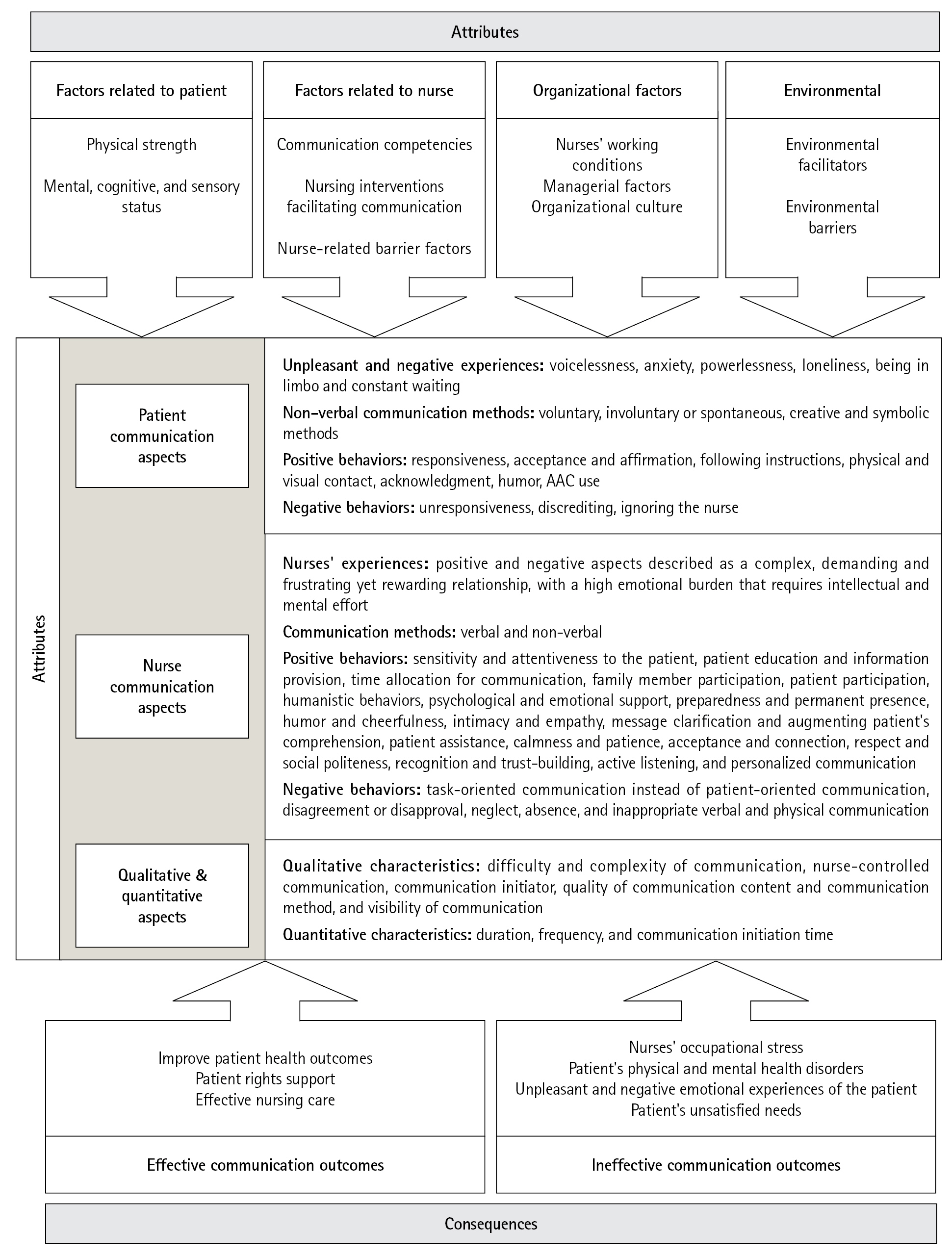
- Providing critical nursing care for conscious mechanically ventilated patients is mediated via effective communication. This study aimed to identify and map the antecedents, attributes, consequences, and definition of nurse–conscious mechanically ventilated patient communication (N-CMVPC). This scoping review was conducted by searching the Cochrane Library and the CINAHL, Embase, PubMed, Web of Science, and Scopus databases, between 2001 and 2021. The keywords queried included "nurses," "mechanically ventilated patients," "mechanical ventilation," "intubated patients," "communication," "interaction," "relationships," "nurse–patient communication," "nurse–patient relations," "intensive care units," and "critical care." Studies related to communication with healthcare personnel or family members were excluded. The results indicated that N-CMVPC manifests as a set of attributes in communication experiences, emotions, methods, and behaviors of the nurse and the patient and is classified into three main themes, nurse communication, patient communication, and quantitative-qualitative aspects. N-CMVPC is a complex, multidimensional, and multi-factor concept. It is often nurse-controlled and can express itself as questions, sentences, or commands in the context of experiences, feelings, and positive or negative behaviors involving the nurse and the patient.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
Patient communication
Nurse communication
Qualitative and quantitative aspects
DISCUSSION
STRENGTHS AND LIMITATIONS OF THE STUDY
IMPLICATIONS AND RECOMMENDATIONS FOR PRACTICE
CONCLUSIONS
KEY MESSAGES
SUPPLEMENTARY MATERIALS
Supplementary Table 1.
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Methodology: MH, FA. Writing–original draft: AM. Writing–review & editing: AM, FA.
NOTES
Acknowledgments


| Study | Country | Design | Aim of study |
|---|---|---|---|
| Holm et al. (2020) [12] | Denmark | Umbrella review | To describe the interaction between ICU patients and the ICU environment |
| Gorzin et al. (2020) [39] | Iran | Quasi‑experimental study with pretest-posttest design | To evaluate the effect of education on function and communication skills of nurses with IMV patients |
| Bayog et al. (2020) [30] | Philippines | Cross-sectional, choice-based conjoint analysis | To explicate the communication preferences of registered nurses towards IMV patients |
| Momennasab et al. (2019) [31] | Iran | Observational study | To describe the quality of the relationship between nurses and IMV patients |
| Wallander Karlsen et al. (2019) [26] | Norway | Observational study | To explore the interaction between IMV patients and healthcare personnel |
| Karlsen et al. (2019) [25] | Norway | Scoping review | To examine previous knowledge about interaction between health care personnel and conscious IMV patients |
| Noguchi et al. (2019) [38] | Japan | Mixed method | To examine changes in the practice of nurses who received an intervention designed to increase their awareness of endotracheally intubated, lightly sedated IMV patients’ intent to communicate |
| Salem and Ahmad (2018) [29] | Jordan | Integrative review | To assess available evidence about existing skills, knowledge, and perceptions and barriers for IMV patients to communicate |
| Carruthers et al. (2017) [9] | UK | Systematic review | To assess the effectiveness of AAC strategies to enable IMV patients to communicate |
| Dithole et al. (2017) [36] | South Africa | Qualitative study | To describe nurses’ experience of a communication skills training intervention |
| Dithole et al. (2016) [6] | South Africa | Structured review | To identify communication challenges existing between nurses and IMV patients |
| Dithole et al. (2016) [14] | South Africa | A retrospective descriptive and explorative research design with a quantitative approach | To determine the existing knowledge and skills of intensive care nurses working with MV patients |
| Ten Hoorn et al. (2016) [34] | Netherlands | Systematic review | To summarize the current evidence regarding communication methods with IMV patients |
| Foà et al. (2016) [7] | Italy | Qualitative study | To investigate how the ICU nurses manages communications and relationships |
| Tembo et al. (2015) [24] | Australia | Qualitative, phenomenological | Describe the lived experiences of people who experienced critical ill patients in the ICU and how it affects the participants' continued existence beyond ICU and hospitalization |
| hermeneutical research | |||
| Happ et al. (2014) [37] | USA | Quasi-experimental design | To assess the effect of two levels of intervention on communication ease, quality, frequency, and success between nurses and IMV patients |
| Nilsen et al. (2014) [17] | USA | Descriptive correlational design | To describe interaction behaviors between nurses and IMV patients and factors which could affect communication |
| To assess relationship between interaction behaviors and nursing care quality | |||
| Nilsen et al. (2013) [32] | USA | Secondary analysis of data from a quasi-experimental study | To examine the association between nurse and patient characteristics, and duration of nurse talk |
| Meriläinen et al. (2013) [28] | Finland | Mixed method study | To describe the interaction between IMV patients and the ICU environment from the perspective of the patients’ memories |
| Karlsson et al. (2012) [4] | Sweden | Qualitative, phenomenological | To observe, interpret, and describe nurses’ communication with conscious IMV patients |
| hermeneutical research | |||
| Happ et al. (2011) [27] | USA | Quantitative (descriptive study) | To describe communication interactions, methods, and assistive techniques between nurses and nonspeaking patients in the ICU |
| Khalaila et al. (2011) [33] | Israel | Cross-sectional study | To investigate the relationship between communication characteristics and psycho-emotional distress among IMV patients, and identify factors predictive of psychological outcomes |
| Grossbach et al. (2011) [35] | Minneapolis | Review article | To review various strategies to promote effective communication between IMV patients, health care staff, and patients’ family members |
| Theme | Category | Subcategory |
|---|---|---|
| Factor related to patient | Physical strength | ▪ Physical condition [12,28,32,34] |
| ▪ Clinical condition [6,12,27,28] | ||
| Mental, cognitive and sensory status | ▪ Mental and cognitive status [6,12,34] | |
| ▪ Level of consciousness [6,12,27,32] | ||
| ▪ Patients' sensory status [12,34] | ||
| Factor related to nurse | Communication competency | ▪ Nurses' skills in controlling and directing communication [6,36] |
| ▪ Nurses' skills in communication methods [6,36] | ||
| ▪ Nurses' skills in communicating with accuracy, sensitivity, and attention [6,36] | ||
| ▪ Nurses' commitment, knowledge and communication experiences [6,36] | ||
| Nursing interventions facilitating communication | ▪ Paying attention to the communication duration [6,32,35] | |
| ▪ Maintaining a proper distance from the patient [6,14,35] | ||
| ▪ Paying attention to the patient needs [7,35] | ||
| ▪ Considering nurses' preferences to communicate [30] | ||
| ▪ Use of para-verbal communication [6,7,14,35] | ||
| ▪ Evaluate the patient's conditions, needs and communication barriers [6,12,14,35] | ||
| Nurse-related barrier factor | ▪ Inadequate knowledge [34] | |
| ▪ Task-oriented communication [6] | ||
| ▪ Communication at an inappropriate time [6,14] | ||
| Organizational factor | Nurses’ working condition | ▪ Work load pressure [7] |
| ▪ Lack of time [7] | ||
| Managerial factor | ▪ Development of communication tools and AAC technologies [29,36] | |
| ▪ Recruiting helpful human resources specialized in communication [7,29,37] | ||
| ▪ Development, application and evaluation of communication standards, tools, and algorithms [12,14,34] | ||
| ▪ Developing nursing education and training [7,12,14,29,35-38] | ||
| ▪ Evaluating and developing nurses' communication skills [36] | ||
| ▪ Improving communication documentation [12,34] | ||
| Organizational culture | ▪ Team work [25,35] | |
| ▪ Inter-professional participation [29,35] | ||
| ▪ Sharing experiences [7] | ||
| Environmental factor | Environmental facilitator | ▪ Appropriate physical environment [7] |
| ▪ Friendly and comfortable communication environment [7,35] | ||
| Environmental barrier | ▪ Unfamiliar environment [7,28] | |
| ▪ Noisy environment [6,35] |
| Theme | Category | Subcategory |
|---|---|---|
| Effective communication outcomes | Improving the patients' health outcomes | ▪ Promoting the patient's health and recovery [25,29] |
| ▪ Promoting the patient comfort and convenience [29,37] | ||
| ▪ Prevent adverse medical outcomes [17,25,30] | ||
| Supporting patient rights | ▪ Patient satisfaction [38] | |
| ▪ Patient participation [25-27,29] | ||
| ▪ Patient respect ▪ Patient satisfaction [38] | ||
| ▪ Improving the quality of medical decisions [7,25,28] | ||
| Effective nursing care | ▪ Development of individual care quality [28,29] | |
| ▪ Identifying and meet the patient needs [7,29] | ||
| ▪ Improving patient abilities and safety [25,29] | ||
| Ineffective communication outcomes | Nurse's occupational stress | ▪ Nurse's frustration and dissatisfaction [7,31] |
| ▪ Nurse's feeling of failure and role inadequacy [7] | ||
| Patient's physical and mental health disorders | ▪ Incidence of anxiety disorders in the patient [9,14,25] | |
| ▪ Patient emotional instability [12,24,27] | ||
| ▪ Patient's body image disturbance [24,27] | ||
| ▪ Impaired patient's health and recovery [14,27,28,30] | ||
| Unpleasant and negative emotional experiences of the patient | ▪ Feeling of dependency and vulnerability [12] | |
| ▪ Patient's experience of being in a bad situation between life and death [12,24] | ||
| ▪ Patient's sense of captivity [12] | ||
| ▪ Patient's feeling of despair and dissatisfaction [9,12,25,31] | ||
| ▪ Patient's feeling of suffering and disorientation due to unmet needs[12] | ||
| Patient's unsatisfied needs | ▪ Unmet patient's needs [12] | |
| ▪ Unknown patient's needs [12] | ||
| ▪ Unevaluated patient's needs [30] |
- 1. He Q, Wang W, Zhu S, Wang M, Kang Y, Zhang R, et al. The epidemiology and clinical outcomes of ventilator-associated events among 20,769 mechanically ventilated patients at intensive care units: an observational study. Crit Care 2021;25:44. ArticlePubMedPMCPDF
- 2. Namadian M, Taran Z. The effect of sedation protocol on sedation level and pharmacological and non-pharmacological interventions on mechanically ventilated patients. Iran J Nurs Midwifery Res 2021;26:316-23.ArticlePubMedPMC
- 3. Zisk-Rony RY, Weissman C, Weiss YG. Mechanical ventilation patterns and trends over 20 years in an Israeli hospital system: policy ramifications. Isr J Health Policy Res 2019;8:20. ArticlePubMedPMCPDF
- 4. Karlsson V, Forsberg A, Bergbom I. Communication when patients are conscious during respirator treatment: a hermeneutic observation study. Intensive Crit Care Nurs 2012;28:197-207.ArticlePubMed
- 5. Blackstone SW, Pressman H. Patient communication in health care settings: new opportunities for augmentative and alternative communication. Augment Altern Commun 2016;32:69-79.ArticlePubMed
- 6. Dithole K, Sibanda S, Moleki MM, Thupayagale-Tshweneagae G. Exploring communication challenges between nurses and mechanically ventilated patients in the intensive care unit: a structured review. Worldviews Evid Based Nurs 2016;13:197-206.ArticlePubMedPDF
- 7. Foà C, Cavalli L, Maltoni A, Tosello N, Sangilles C, Maron I, et al. Communications and relationships between patient and nurse in intensive care unit: knowledge, knowledge of the work, knowledge of the emotional state. Acta Biomed 2016;87:71-82.PubMed
- 8. Martinho CI, Rodrigues IT. Communication of mechanically ventilated patients in intensive care units. Rev Bras Ter Intensiva 2016;28:132-40.ArticlePubMedPMC
- 9. Carruthers H, Astin F, Munro W. Which alternative communication methods are effective for voiceless patients in intensive care units? A systematic review. Intensive Crit Care Nurs 2017;42:88-96.ArticlePubMed
- 10. Burkhart LJ. What is AAC? [Internet]. International Society for Augmentative and Alternative Communication; 2018 [cited 2022 Dec 1]. Available from: https://www.isaac-online.org/english/what-is-AAC.
- 11. Leung CC, Pun J, Lock G, Slade D, Gomersall CD, Wong WT, et al. Exploring the scope of communication content of mechanically ventilated patients. J Crit Care 2018;44:136-41.ArticlePubMed
- 12. Holm A, Viftrup A, Karlsson V, Nikolajsen L, Dreyer P. Nurses' communication with mechanically ventilated patients in the intensive care unit: umbrella review. J Adv Nurs 2020;76:2909-20.ArticlePubMedPDF
- 13. Holm A, Dreyer P. Intensive care unit patients' experience of being conscious during endotracheal intubation and mechanical ventilation. Nurs Crit Care 2017;22:81-8.ArticlePubMedPDF
- 14. Dithole KS, Sibanda S, Moleki MM, Thupayagale-Tshweneagae G. Nurses' communication with patients who are mechanically ventilated in intensive care: the Botswana experience. Int Nurs Rev 2016;63:415-21.ArticlePubMedPDF
- 15. Happ MB. Giving voice: nurse-patient communication in the intensive care unit. Am J Crit Care 2021;30:256-65.ArticlePubMedPDF
- 16. Fleischer S, Berg A, Zimmermann M, Wüste K, Behrens J. Nurse-patient interaction and communication: A systematic literature review. J Pub Health 2009;17:339-53.ArticlePDF
- 17. Nilsen ML, Sereika SM, Hoffman LA, Barnato A, Donovan H, Happ MB. Nurse and patient interaction behaviors' effects on nursing care quality for mechanically ventilated older adults in the ICU. Res Gerontol Nurs 2014;7:113-25.ArticlePubMedPMC
- 18. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol 2005;8:19-32.Article
- 19. Peters MD, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc 2015;13:141-6.ArticlePubMed
- 20. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 2018;169:467-73.ArticlePubMed
- 21. Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci 2010;5:69. ArticlePubMedPMCPDF
- 22. Page MJ, Shamseer L, Tricco AC. Registration of systematic reviews in PROSPERO: 30,000 records and counting. Syst Rev 2018;7:32. ArticlePubMedPMCPDF
- 23. Graneheim UH, Lindgren BM, Lundman B. Methodological challenges in qualitative content analysis: a discussion paper. Nurse Educ Today 2017;56:29-34.ArticlePubMed
- 24. Tembo AC, Higgins I, Parker V. The experience of communication difficulties in critically ill patients in and beyond intensive care: findings from a larger phenomenological study. Intensive Crit Care Nurs 2015;31:171-8.ArticlePubMed
- 25. Karlsen MW, Ølnes MA, Heyn LG. Communication with patients in intensive care units: a scoping review. Nurs Crit Care 2019;24:115-31.ArticlePubMedPDF
- 26. Wallander Karlsen MM, Heggdal K, Finset A, Heyn LG. Attention-seeking actions by patients on mechanical ventilation in intensive care units: a phenomenological-hermeneutical study. J Clin Nurs 2019;28:66-79.ArticlePubMedPDF
- 27. Happ MB, Garrett K, Thomas DD, Tate J, George E, Houze M, et al. Nurse-patient communication interactions in the intensive care unit. Am J Crit Care 2011;20:e28-40.ArticlePubMedPMC
- 28. Meriläinen M, Kyngäs H, Ala-Kokko T. Patients' interactions in an intensive care unit and their memories of intensive care: a mixed method study. Intensive Crit Care Nurs 2013;29:78-87.ArticlePubMed
- 29. Salem A, Ahmad MM. Communication with invasive mechanically ventilated patients and the use of alternative devices: integrative review. J Res Nurs 2018;23:614-30.ArticlePubMedPMCPDF
- 30. Bayog KM, Bello DM, Benabaye JM, Benegas TM, Benito AL, Berioso MA, et al. A conjoint analysis of the communication preferences of registered nurses towards mechanically ventilated patients. Int J Nurs Pract 2020;26:e12809.ArticlePubMedPDF
- 31. Momennasab M, Ardakani MS, Rad FD, Dokoohaki R, Dakhesh R, Jaberi A. Quality of nurses' communication with mechanically ventilated patients in a cardiac surgery intensive care unit. Invest Educ Enferm 2019;37:e02.ArticlePDF
- 32. Nilsen ML, Sereika S, Happ MB. Nurse and patient characteristics associated with duration of nurse talk during patient encounters in ICU. Heart Lung 2013;42:5-12.ArticlePubMedPMC
- 33. Khalaila R, Zbidat W, Anwar K, Bayya A, Linton DM, Sviri S. Communication difficulties and psychoemotional distress in patients receiving mechanical ventilation. Am J Crit Care 2011;20:470-9.ArticlePubMedPDF
- 34. Ten Hoorn S, Elbers PW, Girbes AR, Tuinman PR. Communicating with conscious and mechanically ventilated critically ill patients: a systematic review. Crit Care 2016;20:333. ArticlePubMedPMCPDF
- 35. Grossbach I, Stranberg S, Chlan L. Promoting effective communication for patients receiving mechanical ventilation. Crit Care Nurse 2011;31:46-60.ArticlePDF
- 36. Dithole KS, Thupayagale-Tshweneagae G, Akpor OA, Moleki MM. Communication skills intervention: promoting effective communication between nurses and mechanically ventilated patients. BMC Nurs 2017;16:74. ArticlePubMedPMCPDF
- 37. Happ MB, Garrett KL, Tate JA, DiVirgilio D, Houze MP, Demirci JR, et al. Effect of a multi-level intervention on nurse-patient communication in the intensive care unit: results of the SPEACS trial. Heart Lung 2014;43:89-98.ArticlePubMedPMC
- 38. Noguchi A, Inoue T, Yokota I. Promoting a nursing team's ability to notice intent to communicate in lightly sedated mechanically ventilated patients in an intensive care unit: an action research study. Intensive Crit Care Nurs 2019;51:64-72.ArticlePubMed
- 39. Gorzin K, Sanagoo A, Jouybari L, Pahlavanzadeh B, Jesmi AA. The effect of education on function and communication skill of nurse with intubated patient in intensive care unit. J Nurs Midwifery Sci 2020;7:84-7.Article
- 40. Walker LO, Avant KC. Strategies for theory construction in nursing. Pearson. 2005.
- 41. Wanko Keutchafo EL, Kerr J, Jarvis MA. Evidence of nonverbal communication between nurses and older adults: a scoping review. BMC Nurs 2020;19:53. ArticlePubMedPMCPDF
- 42. Abdolrahimi M, Ghiyasvandian S, Zakerimoghadam M, Ebadi A. Therapeutic communication in nursing students: a Walker & Avant concept analysis. Electron Physician 2017;9:4968-77.ArticlePubMedPMC
- 43. Xue W, Heffernan C. Therapeutic communication within the nurse-patient relationship: a concept analysis. Int J Nurs Pract 2021;27:e12938.ArticlePubMedPDF
- 44. Guttormson JL, Bremer KL, Jones RM. "Not being able to talk was horrid": a descriptive, correlational study of communication during mechanical ventilation. Intensive Crit Care Nurs 2015;31:179-86.ArticlePubMedPMC
References
Figure & Data
References
Citations
- A Study on Nurses' Communication Experiences with Intubation Patients
Ye Rim Kim, Hye Ree Park, Mee Kyung Shin
The Korean Journal of Rehabilitation Nursing.2023; 26(1): 28. CrossRef - The Application of Augmentative and Alternative Communication in Intubated Patients in the Intensive Care Unit: A Scoping Review
Mee-Kyung Shin, Hyejin Jeon
The Korean Journal of Rehabilitation Nursing.2023; 26(2): 97. CrossRef
 PubReader
PubReader Cite
Cite