Abstract
-
Background
- Data on pulmonary hemodynamic parameters in patients with acute respiratory distress syndrome (ARDS) receiving extracorporeal membrane oxygenation (ECMO) are scarce.
-
Methods
- The associations between pulmonary artery catheter parameters for the first 7 days of ECMO, fluid balance, and hospital mortality were investigated in adult patients (aged ≥19 years) who received venovenous ECMO for refractory ARDS between 2015 and 2017.
-
Results
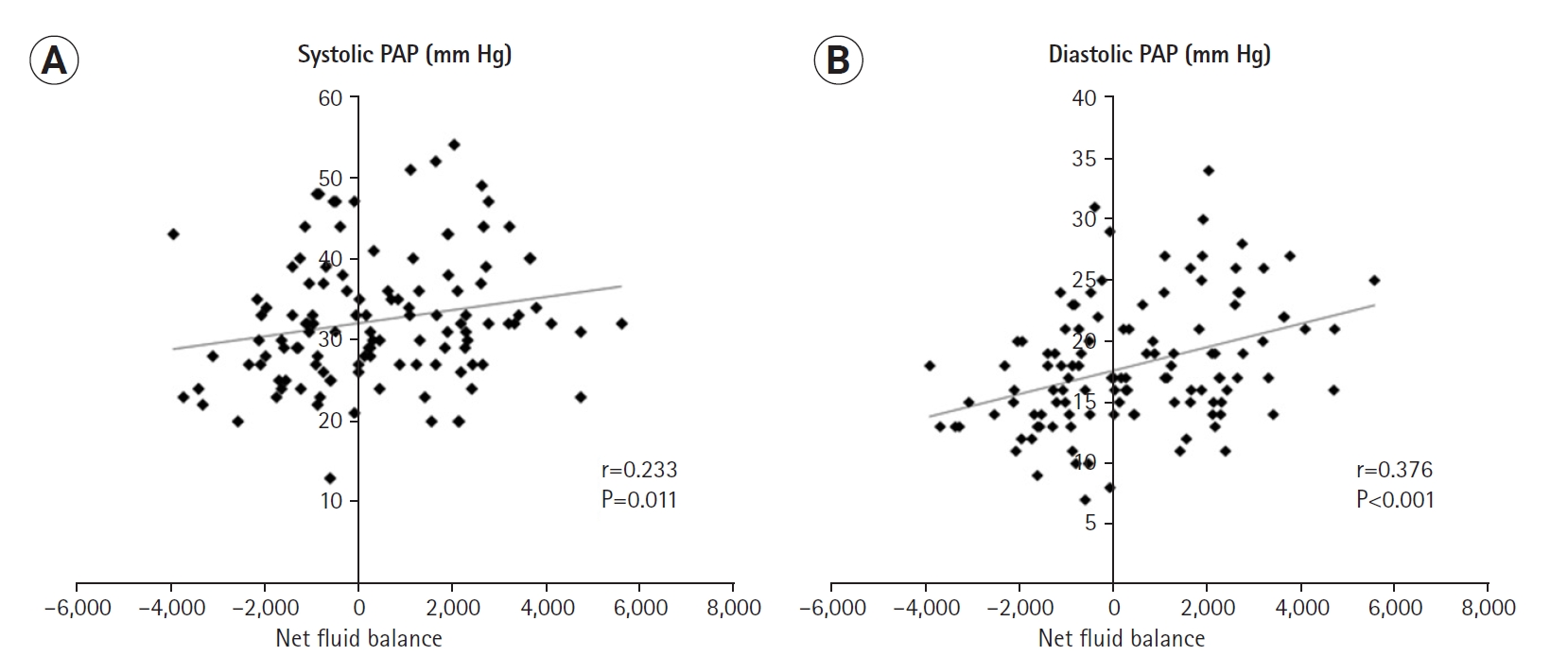
- Twenty patients were finally included in the analysis (median age, 56.0 years; interquartile range, 45.5–68.0 years; female, n=10). A total of 140 values were collected for each parameter (i.e., 7 days×20 patients). Net fluid balance was weakly but significantly correlated with systolic and diastolic pulmonary arterial pressures (PAPs; r=0.233 and P=0.011 r=0.376 and P<0.001, respectively). Among the mechanical ventilation parameters, above positive end-expiratory pressure was correlated with systolic PAP (r=0.191 and P=0.025), and static compliance was negatively correlated with diastolic PAP (r=−0.169 and P=0.048). Non-survivors had significantly higher systolic PAPs than in survivors. However, in multivariate analysis, there was no significant association between mean systolic PAP and hospital mortality (odds ratio, 1.500; 95% confidence interval, 0.937–2.404; P=0.091).
-
Conclusions
- Systolic PAP was weakly but significantly correlated with net fluid balance during the early ECMO period in patients with refractory ARDS receiving ECMO.
-
Keywords: body fluids; extracorporeal membrane oxygenation; pulmonary artery; respiratory distress syndrome
INTRODUCTION
Acute respiratory distress syndrome (ARDS) is frequently complicated by pulmonary hypertension [1,2], and many studies have documented the changes in pulmonary hemodynamic parameters in patients with ARDS. Some have reported that systolic pulmonary arterial pressure (PAP) or mean PAP is a significant indicator of patient outcome [3,4], whereas others did not find any associations or did not specifically evaluate the associations [2,5,6]. However, there is still uncertainty about the underlying pathophysiology between the degree of pulmonary hypertension (or pulmonary vascular dysfunction) and patient outcome.
Routine use of a pulmonary artery catheter (PAC) is not currently recommended because of the lack of clinical benefit and possible complications [7,8]. However, PACs provide unique and various information to intensivists and often change therapy, particularly regarding fluid management and vasopressor use in critically ill patients. In particular, fluid balance has been considered important in terms of patients’ outcomes [8-10].
Recently, extracorporeal membrane oxygenation (ECMO) has been widely used as salvage therapy for patients with severe ARDS. Many authors investigated mechanical ventilation (MV) parameters associated with patient outcomes [11-13]. However, data on pulmonary hemodynamic parameters are very scarce for these patients. Therefore, in this retrospective study, we investigated the association between PAP, fluid balance, and in-hospital mortality in patients in whom a PAC was inserted after initiating venovenous (W) ECMO for refractory ARDS.
MATERIALS AND METHODS
Study Population and Design
This was a retrospective study using data collected from adult patients (age ≥19 years) who received W ECMO for refractory ARDS between January 2015 and January 2017. This study was performed in a single center (tertiary hospital) where annual ECMO volume was 60 cases (W ECMO, 20 cases). During the study period, a PAC was inserted for hemodynamic monitoring in patients for whom written consent was obtained. The Berlin definition was used for diagnosing ARDS [14]. The indications for W ECMO were severe hypoxemia (e.g., PaO2/FiO2 <150) with a high positive end-expiratory pressure (PEEP >10 cm H2O), uncompensated severe hypercapnia (pH <7.20), or excessively high peak inspiratory pressure or plateau pressure, despite standard of care management with a MV [15-17]. The exclusion criteria were patients with cardiopulmonary resuscitation; do-not-resuscitate order; ECMO treatment for respiratory failure other than ARDS; incomplete data on PAC parameters; and those who were transferred to other hospitals during the ECMO treatment.
This study was approved by the Institutional Review Board of Hallym University (IRB No. 2020-06-22) and conducted in accordance with the Declaration of Helsinki. Informed consent was waived due to the retrospective nature of the study.
ECMO and MV Strategies
We used Capiox EBS (Terumo, Tokyo, Japan) or PLS (Maquet, Hirrlingen, Germany) equipment. Both femoral veins were percutaneously cannulated using the Seldinger technique under fluoroscopic guidance. The 17- to 19-Fr (for return) and 21-Fr (for drainage) cannulas were placed (DLP and Bio-Medicus, Medtronic, Minneapolis, MN, USA; RMI, Edward’s Life sciences, Irvine, CA, USA). After ECMO was initiated, the pump flow was adapted (3–5 L/min) to maintain adequate oxygen (SpO2 >88%), and the sweep gas flow was titrated to maintain a PaCO2 of 40 mm Hg (usually 1:1 to blood flow). During ECMO support, heparin was used for anticoagulation, with a target activated partial thromboplastin time of 1.5 times the normal range. MV settings were adjusted to enable lung-protective ventilation after the initiation of ECMO, according to general recommendations [18,19]: tidal volume <6 ml/kg predicted body weight, PEEP ≥5 cm H2O, and peak inspiratory pressure < 30 cm H2O. ECMO weaning was considered when the patient became hemodynamically stable and showed evidence of pulmonary improvement. The pump flow was first tapered to 2 L/min, and the sweep gas to 0 L/min; decannulation was indicated if the patient tolerated these settings [15-17]. ECMO weaning was considered successful when the patient remained stable for 24 hours without ECMO support. MV weaning was undertaken in accordance with the general recommendations [20].
PAC Insertion and Fluid Management
PACs (7.5-Fr; Edwards Lifesciences, Irvine, CA, USA) were inserted, using a balloon-flotation catheter in bedside, through the internal jugular vein within the first 2 hours following initiation of ECMO. Correct positioning of the catheter tip (i.e., in the pulmonary artery) was verified by chest radiography. Systolic and diastolic PAP was monitored continuously, and cardiac output was measured by the thermodilution method using 10 mL of injected cold saline. The cardiac output value was the mean of four cardiac output measurements without artifacts on the temperature curves; the cardiac index (CI) was the ratio of cardiac output to the patient’s body surface area. Daily PAC data were collected between 9–10 AM. However, in our cohort, pulmonary artery occlusion pressure (PAOP) was not measured for safety reasons; instead, we used diastolic PAP values (for PAOP) to calculate pulmonary vascular resistance (PVR). A stable relationship exists between diastolic PAP and PAOP [1,21]. We used a target diastolic PAP of <20 cm H2O for fluid management during ECMO treatment. Mean arterial pressure (MAP) was maintained at >65 mm Hg and urine output >0.5 ml/kg/hr; vasopressors were used if required. The decision to remove the PAC was at the discretion of the physician. The formulas for the PAC parameters were as follows:
Mean PAP=(systolic PAP+2×diastolic PAP)/3
PVR (i.e., modified PVR)=(mean PAP–diastolic PAP)×80/cardiac output
Systemic vascular resistance=(MAP–central venous pressure)×80/cardiac output
Data Collection and Analysis
The following data were obtained: demographic characteristics (age and sex); comorbidities; causes of ARDS; laboratory parameters and severity-of-illness scores (Sequential Organ Failure Assessment [SOFA]) before implementing ECMO; and data on MV parameters and fluid balance (input/output) during the first 7 days of ECMO. Systolic and diastolic PAPs, the CI, systemic vascular resistance, PVR (i.e., modified PVR), and central venous pressure were collected during the first 7 days of ECMO. The rates of successful weaning from ECMO and hospital death were investigated as patient outcomes. The primary outcome was the association between systolic and diastolic PAPs and hospital mortality, and the secondary outcomes were the associations between systolic and diastolic PAPs and daily net fluid balance (i.e., a total fluid balance during the early seven ECMO days).
Statistical Analysis
All results are presented as numbers with percentages for categorical variables, and as medians with interquartile ranges for continuous variables. The Mann-Whitney U-test was used to compare continuous variables, and the chi-square or Fisher’s exact test was employed to compare categorical variables. A multivariable logistic regression analysis, adjusted for age, SOFA, fluid balance, and tidal volume, was performed to investigate an independent association of a PAC parameter (i.e., systolic PAP) with hospital mortality. All probability values were two-sided and a P<0.05 was considered statistically significant. IBM SPSS ver. 25.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses.
RESULTS
Study Population
During the study period, 45 patients received ECMO for refractory ARDS; of these, 26 patients received a PAC (Figure 1). Twenty patients were finally included in the analysis. Their median age was 56.0 years (interquartile range [IQR], 45.5–68.0 years), and 10 patients were female. The median SOFA score was 9.5 (IQR, 7.0–11.0), and 16 (80.0%) of the patients had ARDS of pulmonary origin. Hypertension (20.0%) and heart diseases (20.0%) were the most common comorbidities (Table 1). One patient had a history of cor pulmonale, and pre-ECMO right systolic ventricular pressure was documented only in six patients (48.0 mm Hg; IQR, 46.0–55.0). The median systolic blood pressure, heart rate, and respiratory rates before initiating ECMO were 134.0 mm Hg (IQR, 117.3–148.3 mm Hg), 115.0 beats/min (IQR, 101.0–131.5 beats/min), and 26.0 breaths/min (IQR, 21.3–31.5 breaths/min), respectively. The median duration of MV before initiating ECMO was 1.0 days (IQR, 0.5–2.0 days). The initial PAC parameters (ECMO day 1) are presented in Supplementary Table 1; the mean PAP was 22.8 mm Hg (IQR, 20.1–27.8 mm Hg), and eight patients had pulmonary hypertension (i.e., mean PAP >25 mm Hg). None of the patients underwent prone positioning before and during ECMO treatment.
Treatments and Outcomes
The initial ECMO flow was 4.2 L/min (IQR, 3.9–4.5 L/min) with a sweep gas flow of 4.0 L/min (IQR, 4.0–4.0 L/min). The median numbers of packed red blood cells and platelets transfused were 12.5 units (IQR, 8.0–15.5 units) and 28.5 units (IQR, 0.0–63.5 units), respectively, with no difference between survivors and non-survivors (data not shown). The MV settings before initiating ECMO did not differ between the two groups (Table 1). Fourteen patients (70.0%) were successfully weaned from ECMO and 11 (55.0%) survived to discharge; the median ECMO duration was 18.5 days (IQR, 10.0–27.0 days). The lengths of the intensive care unit (ICU) and hospital stays were 32.0 days (IQR, 26.0–42.8 days) and 42.5 days (IQR, 28.5–53.8 days). None of the patients underwent lung transplantations.
Correlation Analyses
A total of 140 samples were collected per parameter (i.e., 7 days×20 patients). Net fluid balance was weakly but significantly correlated with systolic and diastolic PAPs (r=0.233 and P=0.011; r=0.376 and P<0.001, respectively) (Figure 2, Table 2) and was negatively correlated with the CI (r=−0.205 and P=0.025). Among the MV parameters, above PEEP was correlated with systolic PAP (r=0.191 and P=0.025) (Table 3), and static compliance (i.e., tidal volume/above PEEP in pressure-controlled ventilation mode) was negatively correlated with diastolic PAP (r=−0.169 and P=0.048).
Univariate and Multivariate Analyses
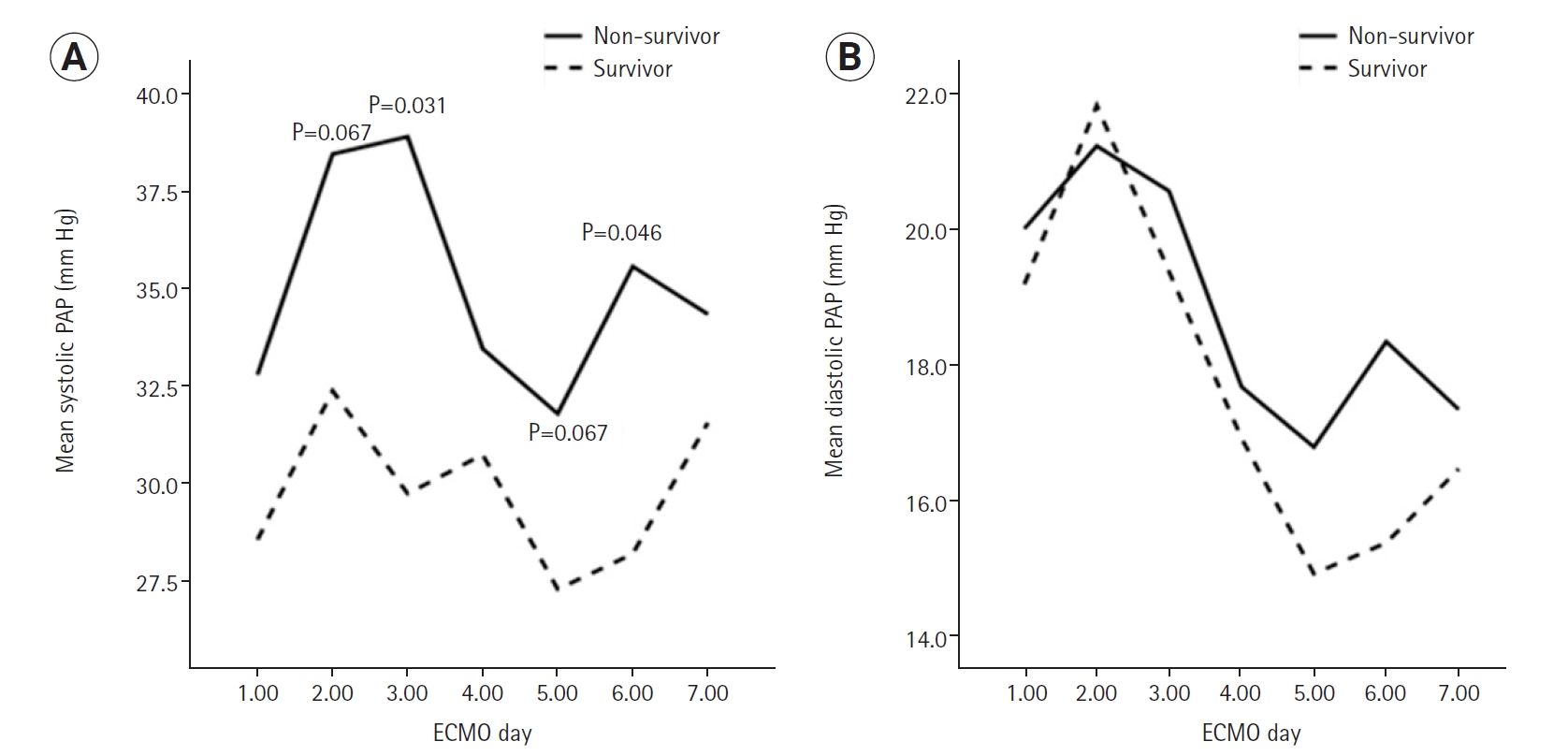
Among the PAC parameters, systolic PAP was significantly higher in non-survivors than in survivors (Table 4, Figure 3). However, no significant differences were observed in daily fluid balance (Supplementary Table 2) or MV parameters (Supplementary Table 3) between the two groups. In the multivariable model, five variables (age, SOFA, fluid balance, tidal volume, and systolic PAP) were included (Table 5), and mean systolic PAP was not significantly associated with hospital mortality (odds ratio, 1.500; 95% confidence interval, 0.937–2.404).
DISCUSSION
This retrospective study revealed that net fluid balance was weakly but significantly correlated with systolic and diastolic PAPs in patients receiving W ECMO for severe ARDS. Besides, systolic PAP was significantly higher in non-survivors than survivors. However, the mean systolic PAP value during the first 7 days of ECMO was not significantly associated with hospital mortality.
Previous large-scale randomized trials have demonstrated no survival benefit of PAC-guided therapy compared to standard care (in surgical patients) or central venous catheter-guided therapy in those with acute lung injury [7,22,23]. In particular, the PAC-guided therapy was associated with a two-fold risk of catheter-related complications compared to central venous catheter-guided therapy [7]. Since then, the routine use of PAC has not been recommended. However, our aim in this retrospective study was not to evaluate the usefulness of PAC but to investigate the therapeutic or prognostic role of PAP in patients receiving ECMO for refractory ARDS. We inserted PACs in patients undergoing W ECMO to monitor hemodynamics and guide conservative fluid management. A relatively large volume of fluid was given to patients during the early period (e.g., days 1–3) (Supplementary Table 2), but we tried to maintain a conservative strategy while monitoring diastolic PAP and using diuretics. Although we did not find any strong associations due to small sample size, PAP may reflect fluid balance, and a higher systolic PAP might be associated with higher mortality in patients receiving W ECMO for severe ARDS. These results are consistent with those reported previously [3,4].
As noted above, we did not inflate the balloon of the PAC to measure PAOP in our patients for safety reasons; occluding the proximal pulmonary artery may be associated with an increased risk of thromboembolism or rupture of the pulmonary artery in critically ill patients. Previous studies have reported that the incidence rates of catheter-related infections or embolization in patients with a PAC are 0%–4.6% or 1%–11%, respectively [22-24]. No case of thromboembolic complications was detected in our cohort, but one patient (5.0%) had PAC-related bacteremia; however, the duration of PAC indwelling was longer than that reported in previous studies [22].
ARDS elevates PAP and consequently increases right ventricular afterload, and this elevated pressure harms patient outcomes. Although data are still conflicting [2,5,6], some previous studies have reported the prognostic significance of PAP in patients with ARDS [1,3,4,25]. In a secondary analysis of 501 patients from the Fluid and Catheter Treatment Trial by the ARDS Network, the largest trial in the era of lung-protective ventilation, a high transpulmonary gradient or PVR was significantly associated with a poor outcome [1]; however, no difference was detected in PAP between survivors and non-survivors in the study. Of importance, PVR is affected mainly by factors that are intrinsic to the lung (e.g., lung injury in ARDS), whereas PAP is affected not only by factors that are intrinsic to the lung (e.g., PVR) but also by extrinsic factors (e.g., right ventricular function). This may have contributed to the different mortality results between the two parameters [2]. In our analysis, diastolic PAP was used instead of PAOP to calculate PVR. Although we cannot conclusively state that the PVR values in our study were correct, the PVRs were significantly higher in non-survivors than in survivors during the first 7 days of ECMO (Table 4), which is consistent with previous data [1,26]. However, the presence of pulmonary vascular dysfunction is likely to be a simple marker of lung injury severity. The causal relationship, as well as the exact mechanism, between pulmonary vascular dysfunction and patient outcomes remains unclear.
Previous studies have demonstrated that conservative fluid management is important to the outcomes of patients with ARDS, including those receiving ECMO [8,9]. In our cohort, net fluid balance did not differ during the early ECMO days between survivors and non-survivors. However, interestingly, systolic and diastolic PAPs were weakly but significantly correlated with net fluid balance (Table 2). These results suggest that if a new noninvasive method is validated in the future [27,28], systolic PAP could be a useful parameter for optimizing fluid management or predicting patient outcomes. However, systolic PAP did not show any correlations with oxygenation (initial PaO2/FiO2 ratio) and other outcomes (i.e., durations of ECMO and MV, and ICU and hospital length of stay).
Regarding ventilator settings, above PEEP was correlated with systolic PAP (Table 3). This implies that together with fluid balance, above PEEP may be a determining factor for PAP. However, notably, lung compliance was also correlated with diastolic PAP. When considering the association of diastolic PAP with fluid balance (Table 2), we may say that a negative (or less) fluid balance can induce an increase in lung compliance. However, contrary to a previous study [11], neither lung compliance nor diastolic PAP was associated with hospital mortality in our study population. More research is needed to clarify this point.
To date, data on PAC parameters in patients receiving ECMO for severe ARDS are very scarce. Hemmila et al. [6] reported no difference in pre-ECMO systolic and diastolic PAPs between survivors and non-survivors. In contrast, Lazzeri et al. [29] found that survival is significantly associated with lower pre-ECMO systolic PAP. We collected and analyzed PAC data obtained after initiating W ECMO (during the first 7 days of ECMO), which is one of the strengths of our study. Although our study was underpowered to verify a significant association between systolic PAP and hospital mortality due to its small sample size, the investigation of the role of PAPs seems reasonable in patients receiving ECMO, when considering many factors affecting pulmonary vascular function, such as volume overload, vasopressors, and MV.
This study had several limitations. First, because of the small sample size and retrospective nature of the study, the results may reflect unintended bias. In particular, half of the patients did not receive a PAC during the study period. Second, as aforementioned, we did not measure PAOP directly but used diastolic PAP to calculate PVR. Third, mean values for PAC parameters (for 7 days) were used in the present study. However, daily values might be more valuable in clinical practice. Fourth, although we followed the Extracorporeal Life Support Organization guidelines, ECMO management practices have not been standardized. Fifth, we did not investigate long-term outcomes including quality of life in our study population. However, this is the first study to show the potential usefulness of PAPs obtained during the early ECMO period for predicting outcomes in patients with severe ARDS. Therefore, despite several limitations, our results merit further consideration.
In conclusion, systolic PAP was weakly but significantly correlated with net fluid balance during the early ECMO period among patients with refractory ARDS. Despite no significant association in multivariable analysis, systolic PAP may be a potential parameter for optimizing fluid management or predicting patient outcomes.
KEY MESSAGES
▪ Net fluid balance was weakly but significantly correlated with systolic and diastolic pulmonary arterial pressure (PAP) in patients with refractory acute respiratory distress syndrome receiving extracorporeal membrane oxygenation.
▪ Systolic PAP was higher in non-survivors than in survivors, but was not associated with hospital mortality in multivariable analysis.
NOTES
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: THH, SP. Data curation: all authors. Formal analysis: all authors. Methodology: all authors. Project administration: SP. Visualization: THH, HSK. Writing–original draft: THH, SP. Writing–review & editing: all authors.
Acknowledgments
We would like to thank Dr. Seong-Sik Cho (Dong-A University Hospital) for his dedication to the statistical analyses in the study.
SUPPLEMENTARY MATERIALS
Supplementary materials can be found via https://doi.org/10.4266/acc.2021.00927.
Supplementary Table 2.
Input and output (L/day) between survivors and non-survivors during the early 7 days of ECMO
acc-2021-00927-suppl2.pdf
Supplementary Table 3.
Mechanical ventilation parameters between survivors and non-survivors during the early seven ECMO days
acc-2021-00927-suppl3.pdf
Figure 1.Flowchart of patients enrolment. W: venovenous; ECMO: extracorporeal membrane oxygenation; PAC: pulmonary arterial catheter; ARDS: acute respiratory distress syndrome.
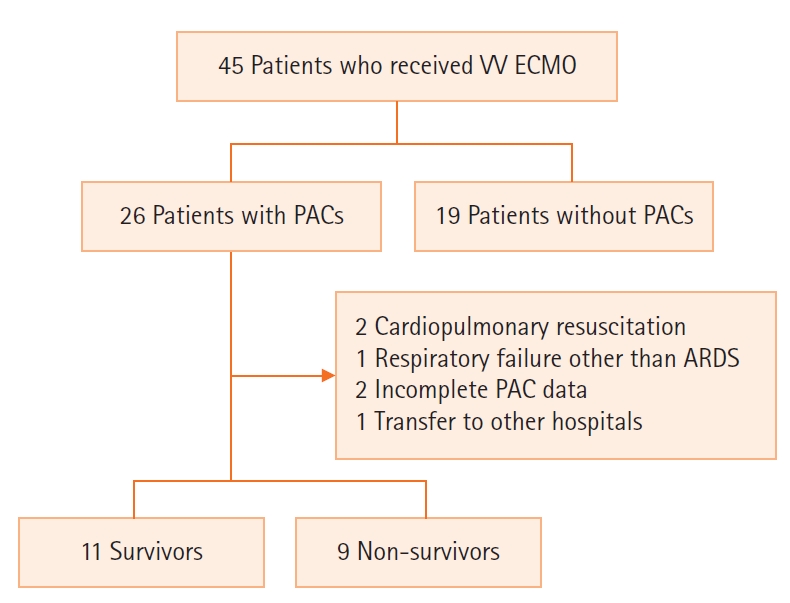
Figure 2.Correlation analyses between pulmonary arterial pressures (PAPs) and net fluid balance during the first 7 extracorporeal membrane oxygenation (ECMO) period. (A) Corrlation between systolic PAP and net fluid balance and (B) correlation between diastolic PAP and net fluid balance. Gray line indicates trend line.
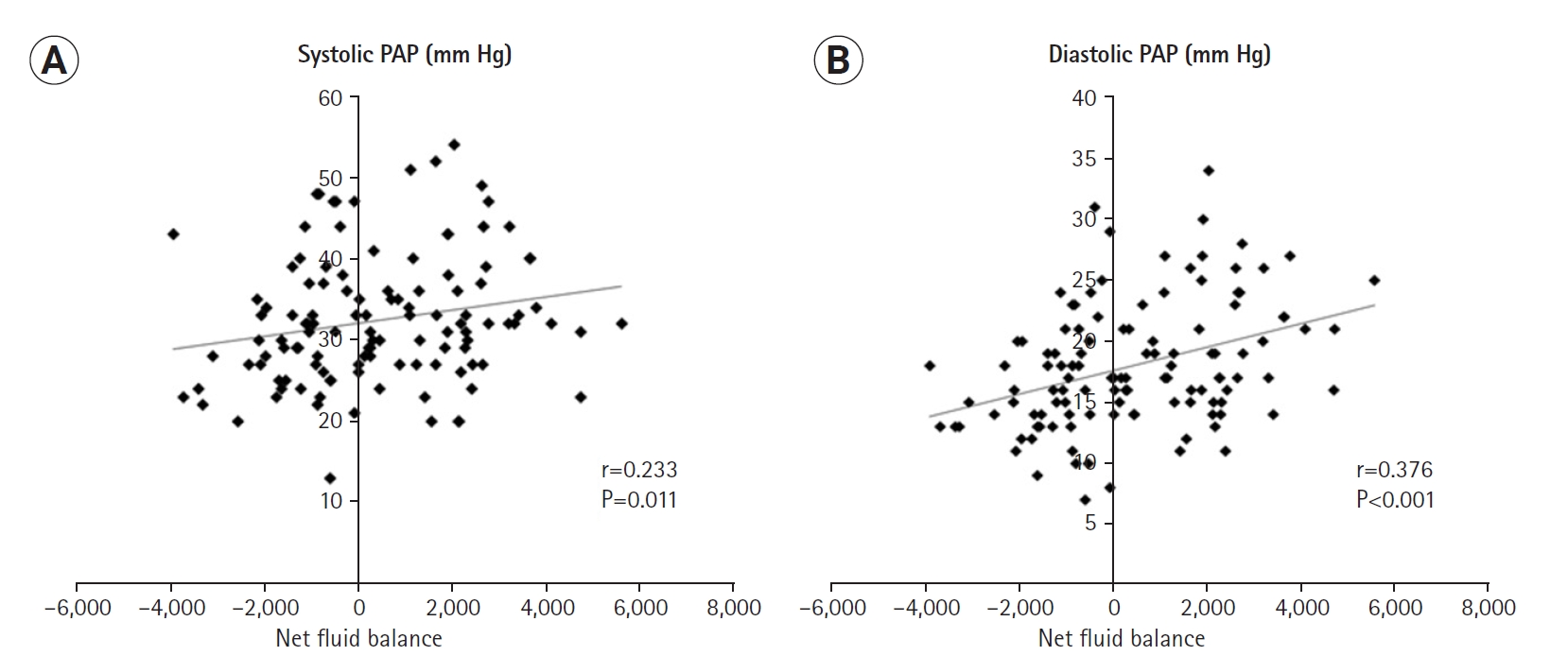
Figure 3.Comparison of mean (A) systolic and (B) diastolic pulmonary arterial pressures (PAPs) between survivors and non-survivors. ECMO: extracorporeal membrane oxygenation.
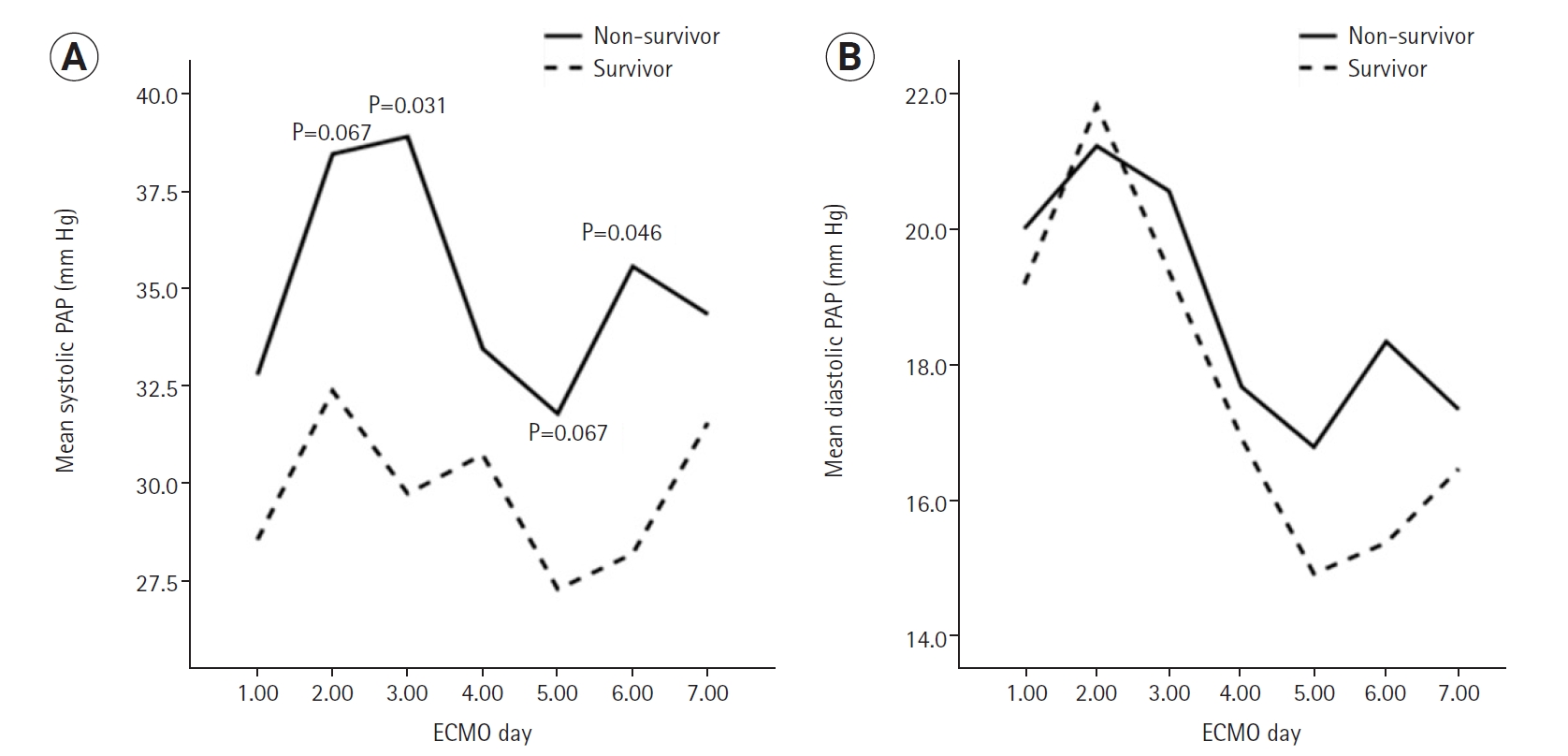
Table 1.Baseline characteristics before ECMO treatment
|
Variable |
Survivor (n=11) |
Non-survivor (n=9) |
P-value |
|
Age (yr) |
49.0 (45.0–61.0) |
68.0 (49.5–72.5) |
0.112 |
|
Sex (male:female) |
6:5 |
4:5 |
1.000 |
|
Comorbidity |
|
|
|
|
Diabetes |
2 (18.2) |
1 (11.1) |
1.000 |
|
Hypertension |
3 (27.3) |
1 (11.1) |
0.591 |
|
Heart disease |
1 (9.1) |
3 (33.3) |
0.285 |
|
Chronic kidney disease |
0 |
1 (11.1) |
0.450 |
|
Liver cirrhosis |
1 (9.1) |
0 |
1.000 |
|
Cancer |
0 |
1 (11.1) |
0.450 |
|
Reason for ECMO |
|
|
|
|
Pulmonary origin |
8 |
8 |
0.591 |
|
Non-pulmonary origin |
3 |
1 |
|
SOFA score at admission |
10.0 (8.0–14.0) |
8.0 (7.0–10.0) |
0.084 |
|
Respiratory SOFA score |
4.0 (4.0–4.0) |
4.0 (4.0–4.0) |
0.668 |
|
PaO2/FiO2 ratio |
85.6 (77.7–98.9) |
98.9 (82.8–99.0) |
0.208 |
|
White blood cell counts (103/µl) |
13.2 (9.0–21.0) |
16.7 (9.5–17.9) |
0.882 |
|
Hemoglobin (g/dl) |
11.9 (9.8–13.8) |
11.0 (9.9–12.4) |
0.503 |
|
Platelet (103/µl) |
109.0 (59.0–163.0) |
256.0 (147.5–281.0) |
0.007 |
|
Bilirubin (mg/dl) |
1.5 (0.3–2.8) |
0.2 (0.2–1.1) |
0.020 |
|
Albumin (g/dl) |
3.0 (2.8–3.5) |
2.8 (2.5–3.0) |
0.131 |
|
Creatinine (mg/dl) |
1.2 (0.8–1.3) |
0.8 (0.5–1.3) |
0.370 |
|
C-reactive protein (mg/L) |
191.6 (160.4–292.3) |
196.9 (108.1–209.5) |
0.331 |
|
Brain natriuretic peptide (pg/ml) |
342.0 (22.9–2898.0) |
235.8 (61.6–489.7) |
0.551 |
|
Vasopressor use |
9 (81.8) |
2 (22.2) |
0.024 |
|
Ejection fraction (%) |
60.0 (60.0–66.0) |
60.0 (55.0–65.5) |
0.969 |
|
MV setting before ECMO |
|
|
|
|
Above PEEP (cm H2O) |
15.0 (12.0–20.0) |
18.0 (14.0–19.0) |
0.878 |
|
PEEP (cm H2O) |
10.0 (6.0–12.0) |
14.0 (12.0–15.0) |
0.083 |
|
Respiratory rate (breaths/min) |
18.0 (12.0–26.0) |
20.0 (18.0–28.0) |
0.180 |
Table 2.Correlation of net fluid balance with PAC parameters during the early 7 ECMO days
|
Net fluid balance |
Cardiac index |
Systolic PAP |
Diastolic PAP |
PVR |
SVR |
CVP |
|
r |
–0.205 |
0.233 |
0.376 |
0.038 |
0.048 |
0.213 |
|
P-value |
0.025 |
0.011 |
<0.001 |
0.684 |
0.599 |
0.020 |
Table 3.Correlation of mechanical ventilation with PAC parameters during the early seven ECMO days
|
Variable |
Above PEEP |
PEEP |
Tidal volume |
Static compliance |
|
Systolic PAP |
|
|
|
|
|
r |
0.191 |
–0.042 |
–0.038 |
–0.120 |
|
P-value |
0.025 |
0.622 |
0.655 |
0.161 |
|
Diastolic PAP |
|
|
|
|
|
r |
0.162 |
0.162 |
–0.079 |
–0.169 |
|
P-value |
0.058 |
0.058 |
0.356 |
0.048 |
|
Mean PAP |
|
|
|
|
|
r |
0.175 |
0.095 |
–0.061 |
–0.153 |
|
P-value |
0.041 |
0.266 |
0.473 |
0.073 |
|
PVR |
|
|
|
|
|
r |
0.049 |
–0.123 |
–0.110 |
–0.040 |
|
P-value |
0.568 |
0.152 |
0.194 |
0.645 |
|
SVR |
|
|
|
|
|
r |
–0.111 |
0.155 |
–0.324 |
–0.171 |
|
P-value |
0.195 |
0.070 |
<0.001 |
0.044 |
|
Cardiac index |
|
|
|
|
|
r |
–0.013 |
–0.139 |
–0.021 |
–0.006 |
|
P-value |
0.884 |
0.105 |
0.806 |
0.946 |
Table 4.PAC parameters between survivors and non-survivors during the early 7 days of ECMO (140 samples for each variable per group)
|
Variable |
Survivor
|
Non-survivor
|
P-valuea
|
|
Median (IQR) |
Mean±SD |
Median (IQR) |
Mean±SD |
|
Cardiac index (L/min/m2) |
5.5 (4.1–6.8) |
5.7±2.3 |
4.9 (4.0–5.9) |
5.5±2.5 |
0.344 |
|
Systolic PAP (mm Hg) |
29.0 (25.0–33.5) |
29.8±7.2 |
33.0 (30.0–40.0) |
35.0±7.8 |
<0.001 |
|
Diastolic PAP (mm Hg) |
17.0 (14.5–20.5) |
17.7±4.8 |
19.0 (14.0–23.0) |
18.8±5.8 |
0.221 |
|
PVR (dyn∙sec/cm5) |
55.0 (44.0–74.0) |
58.7±27.3 |
65.0 (55.0–98.0) |
73,4±34,4 |
0.006 |
|
SVR (dyn∙sec/cm5) |
985.0 (790.0–1152.5) |
1,007.3±320.5 |
838.0 (551.0–1183.0) |
887.9±363.3 |
0.034 |
|
CVP (mm Hg) |
10.0 (8.0–13.0) |
10.6±3.4 |
10.0 (7.0–15.0) |
10.7±4.9 |
0.875 |
Table 5.Univariable and multivariable analysis for hospital deatha
|
Variable |
Univariable analysis
|
Multivariable analysis
|
|
OR |
95% CI |
P-value |
OR |
95% CI |
P-value |
|
Age |
1.506 |
0.978–1.140 |
0.167 |
1.053 |
0.914– 1.214 |
0.475 |
|
SOFA |
0.710 |
0.481–1.047 |
0.084 |
0.585 |
0.294–1.164 |
0.126 |
|
Fluid balanceb
|
1.122 |
0.999–1.260 |
0.051 |
1.000 |
1.000–1.000 |
0.222 |
|
Tidal volume |
1.000 |
1.000–1.000 |
0.106 |
0.986 |
0.949–1.025 |
0.481 |
|
Systolic PAPc
|
1.234 |
0.992–1.536 |
0.060 |
1.500 |
0.937–2.404 |
0.091 |
References
- 1. Bull TM, Clark B, McFann K, Moss M, National Institutes of Health/National Heart, Lung, and Blood Institute ARDS Network. Pulmonary vascular dysfunction is associated with poor outcomes in patients with acute lung injury. Am J Respir Crit Care Med 2010;182:1123-8.ArticlePubMedPMC
- 2. Ryan D, Frohlich S, McLoughlin P. Pulmonary vascular dysfunction in ARDS. Ann Intensive Care 2014;4:28. ArticlePubMedPMC
- 3. Osman D, Monnet X, Castelain V, Anguel N, Warszawski J, Teboul JL, et al. Incidence and prognostic value of right ventricular failure in acute respiratory distress syndrome. Intensive Care Med 2009;35:69-76.ArticlePubMed
- 4. Squara P, Dhainaut JF, Artigas A, Carlet J. Hemodynamic profile in severe ARDS: results of the European Collaborative ARDS Study. Intensive Care Med 1998;24:1018-28.ArticlePubMed
- 5. Cepkova M, Kapur V, Ren X, Quinn T, Zhuo H, Foster E, et al. Pulmonary dead space fraction and pulmonary artery systolic pressure as early predictors of clinical outcome in acute lung injury. Chest 2007;132:836-42.ArticlePubMed
- 6. Hemmila MR, Rowe SA, Boules TN, Miskulin J, McGillicuddy JW, Schuerer DJ, et al. Extracorporeal life support for severe acute respiratory distress syndrome in adults. Ann Surg 2004;240:595-607.ArticlePubMedPMC
- 7. National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wheeler AP, Bernard GR, Thompson BT, Schoenfeld D, Wiedemann HP, et al. Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med 2006;354:2213-24.ArticlePubMed
- 8. National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006;354:2564-75.ArticlePubMed
- 9. Schmidt M, Bailey M, Kelly J, Hodgson C, Cooper DJ, Scheinkestel C, et al. Impact of fluid balance on outcome of adult patients treated with extracorporeal membrane oxygenation. Intensive Care Med 2014;40:1256-66.ArticlePubMedPMC
- 10. Temmesfeld-Wollbrück B, Walmrath D, Grimminger F, Seeger W. Prevention and therapy of the adult respiratory distress syndrome. Lung 1995;173:139-64.ArticlePubMed
- 11. Kim HS, Kim JH, Chung CR, Hong SB, Cho WH, Cho YJ, et al. Lung compliance and outcomes in patients with acute respiratory distress syndrome receiving ECMO. Ann Thorac Surg 2019;108:176-82.ArticlePubMed
- 12. Schmidt M, Pham T, Arcadipane A, Agerstrand C, Ohshimo S, Pellegrino V, et al. Mechanical ventilation management during extracorporeal membrane oxygenation for acute respiratory distress syndrome: an international multicenter prospective cohort. Am J Respir Crit Care Med 2019;200:1002-12.ArticlePubMed
- 13. Shigemura N. Extracorporeal lung support for advanced lung failure: a new era in thoracic surgery and translational science. Gen Thorac Cardiovasc Surg 2018;66:130-6.ArticlePubMed
- 14. ARDS Definition Task Force; Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA 2012;307:2526-33.PubMed
- 15. ELSO Guideline for Adult Respiratory Failure Managed with Venovenous ECMO [Internet]. Ann Arbor (MI), Extracorporeal Life Support Organization. 2021;[cited 2021 May 1]. Available from: https://www.elso.org/ecmo-resources/elso-ecmo-guidelines.aspx.
- 16. Tonna JE, Abrams D, Brodie D, Greenwood JC, Rubio Mateo-Sidron JA, Usman A, et al. Management of adult patients supported with venovenous extracorporeal membrane oxygenation (VV ECMO): guideline from the Extracorporeal Life Support Organization (ELSO). ASAIO J 2021;67:601-10.ArticlePubMedPMC
- 17. Brodie D, Bacchetta M. Extracorporeal membrane oxygenation for ARDS in adults. N Engl J Med 2011;365:1905-14.ArticlePubMed
- 18. Sevransky JE, Levy MM, Marini JJ. Mechanical ventilation in sepsis-induced acute lung injury/acute respiratory distress syndrome: an evidence-based review. Crit Care Med 2004;32(11 Suppl):S548-53.ArticlePubMed
- 19. Stephens RS, Shah AS, Whitman GJ. Lung injury and acute respiratory distress syndrome after cardiac surgery. Ann Thorac Surg 2013;95:1122-9.ArticlePubMed
- 20. McConville JF, Kress JP. Weaning patients from the ventilator. N Engl J Med 2013;368:1068-9.Article
- 21. Chemla D, Lau EM, Papelier Y, Attal P, Hervé P. Pulmonary vascular resistance and compliance relationship in pulmonary hypertension. Eur Respir J 2015;46:1178-89.ArticlePubMed
- 22. Richard C, Warszawski J, Anguel N, Deye N, Combes A, Barnoud D, et al. Early use of the pulmonary artery catheter and outcomes in patients with shock and acute respiratory distress syndrome: a randomized controlled trial. JAMA 2003;290:2713-20.ArticlePubMed
- 23. Sandham JD, Hull RD, Brant RF, Knox L, Pineo GF, Doig CJ, et al. A randomized, controlled trial of the use of pulmonary-artery catheters in high-risk surgical patients. N Engl J Med 2003;348:5-14.ArticlePubMed
- 24. Mermel LA, Maki DG. Infectious complications of Swan-Ganz pulmonary artery catheters: pathogenesis, epidemiology, prevention, and management. Am J Respir Crit Care Med 1994;149(4 Pt 1):1020-36.ArticlePubMed
- 25. Beiderlinden M, Eikermann M, Boes T, Breitfeld C, Peters J. Treatment of severe acute respiratory distress syndrome: role of extracorporeal gas exchange. Intensive Care Med 2006;32:1627-31.ArticlePubMed
- 26. Villar J, Blazquez MA, Lubillo S, Quintana J, Manzano JL. Pulmonary hypertension in acute respiratory failure. Crit Care Med 1989;17:523-6.ArticlePubMed
- 27. Proenca M, Braun F, Muntane E, Sola J, Adler A, Lemay M, et al. Non-invasive monitoring of pulmonary artery pressure at the bedside. Annu Int Conf IEEE Eng Med Biol Soc 2016;2016:4236-9.ArticlePubMed
- 28. Sanders M, Servaas S, Slagt C. Accuracy and precision of non-invasive cardiac output monitoring by electrical cardiometry: a systematic review and meta-analysis. J Clin Monit Comput 2020;34:433-60.ArticlePubMed
- 29. Lazzeri C, Cianchi G, Bonizzoli M, Batacchi S, Terenzi P, Bernardo P, et al. Pulmonary vascular dysfunction in refractory acute respiratory distress syndrome before veno-venous extracorporeal membrane oxygenation. Acta Anaesthesiol Scand 2016;60:485-91.ArticlePubMed
Citations
Citations to this article as recorded by


 , Hyoung Soo Kim2
, Hyoung Soo Kim2

 PubReader
PubReader ePub Link
ePub Link Cite
Cite