Articles
- Page Path
- HOME > Acute Crit Care > Volume 34(4); 2019 > Article
-
Case Report
Infection A successful application of adult polymyxin B-immobilized fiber column hemoperfusion to a neonate with septic shock -
Young A Kim1
 , Hyungtae Kim2, Yu-Mi Kim3, Su Eun Park1
, Hyungtae Kim2, Yu-Mi Kim3, Su Eun Park1 -
Acute and Critical Care 2018;34(4):284-288.
DOI: https://doi.org/10.4266/acc.2017.00528
Published online: November 6, 2018
1Department of Pediatrics, Pusan National University Children’s Hospital, Yangsan, Korea
2Department of Thoracic and Cardiovascular Surgery, Pusan National University Yangsan Hospital, Yangsan, Korea
3Department of Artificial Kidney Unit, Pusan National University Yangsan Hospital, Yangsan, Korea
- Corresponding author Young A Kim Department of Pediatrics, Pusan National University Children’s Hospital, 20 Geumo-ro, Mulgeumeup, Yangsan 50612, Korea Tel: +82-55-360-3516 Fax: +82-55-360-2181 E-mail: youngflo@hanmail.net
• Received: October 15, 2017 • Revised: February 2, 2018 • Accepted: February 11, 2018
Copyright © 2019 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article has been corrected. See "A successful application of adult polymyxin B-immobilized fiber column hemoperfusion to a neonate with septic shock" in Volume 38 on page 515.
Abstract
- Direct hemoperfusion therapy with a polymyxin B-immobilized fiber column (PMX-HP) has been introduced as a therapeutic option for gram negative bacterial septic shock in adults. However, its use in neonates and children has not yet been established. We successfully performed hemoperfusion therapy using an adult polymyxin B-immobilized fiber column in a neonate with carbapenem resistant Acinetobacter baumannii septic shock. The application was technically feasible because the neonate was on extracorporeal membrane oxygenation (ECMO). Although it did not rescue the patient, there was significant short-lasting improvement in pulmonary oxygenation and hemodynamics, leading to wean the patient from ECMO. PMX-HP could be used as an adjunctive treatment for selected neonatal and pediatric patients with gram negative bacterial septic shock.
CASE REPORT
DISCUSSION
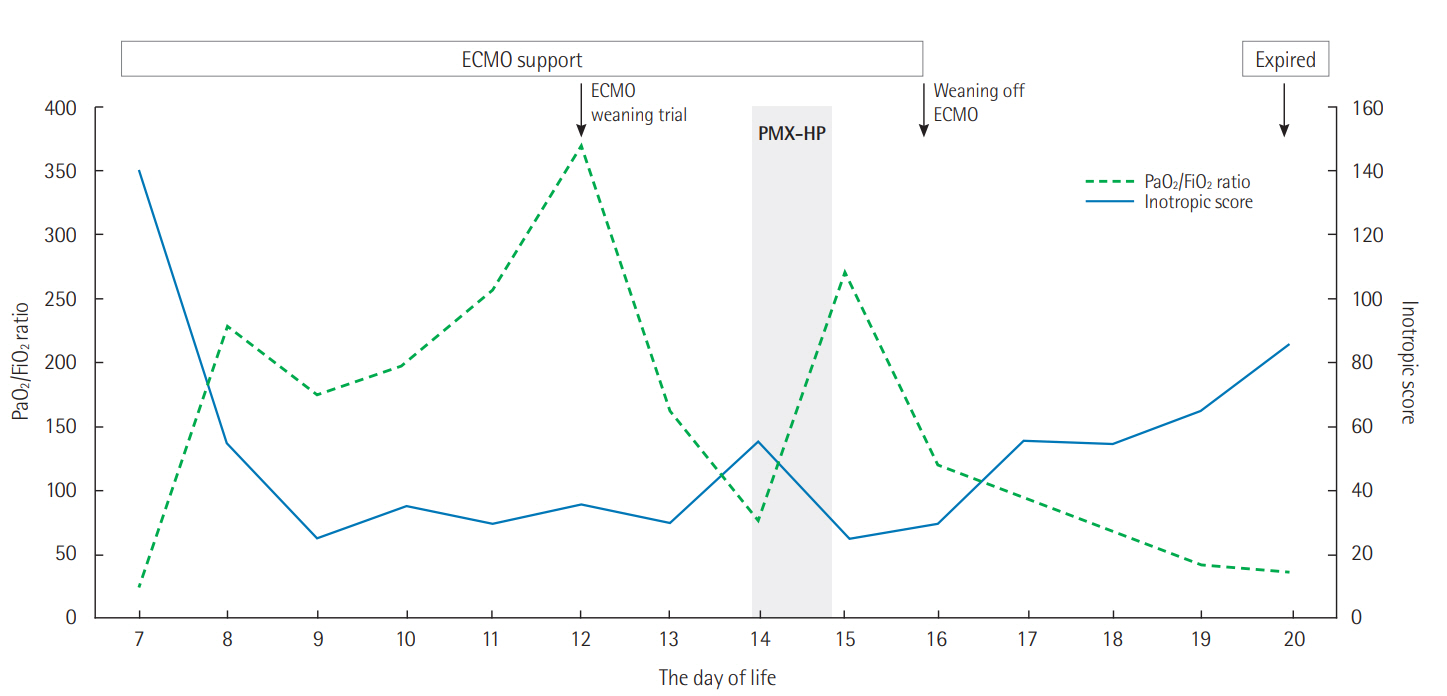
Figure 1.Clinical course and serial changes of PaO2/FiO2 ratio and inotropic score. ECMO was applied to a 7-day-old neonate with septic shock. After the application of PMX-HP, PaO2/FiO2 ratio was improved and inotropic score decreased, and the ECMO was discontinued. However, the patient’s condition deteriorated and the patient died on the 20th day of life. ECMO: extracorporeal membrane oxygenation; PMX-HP: hemoperfusion therapy with a polymyxin B-immobilized fiber column.
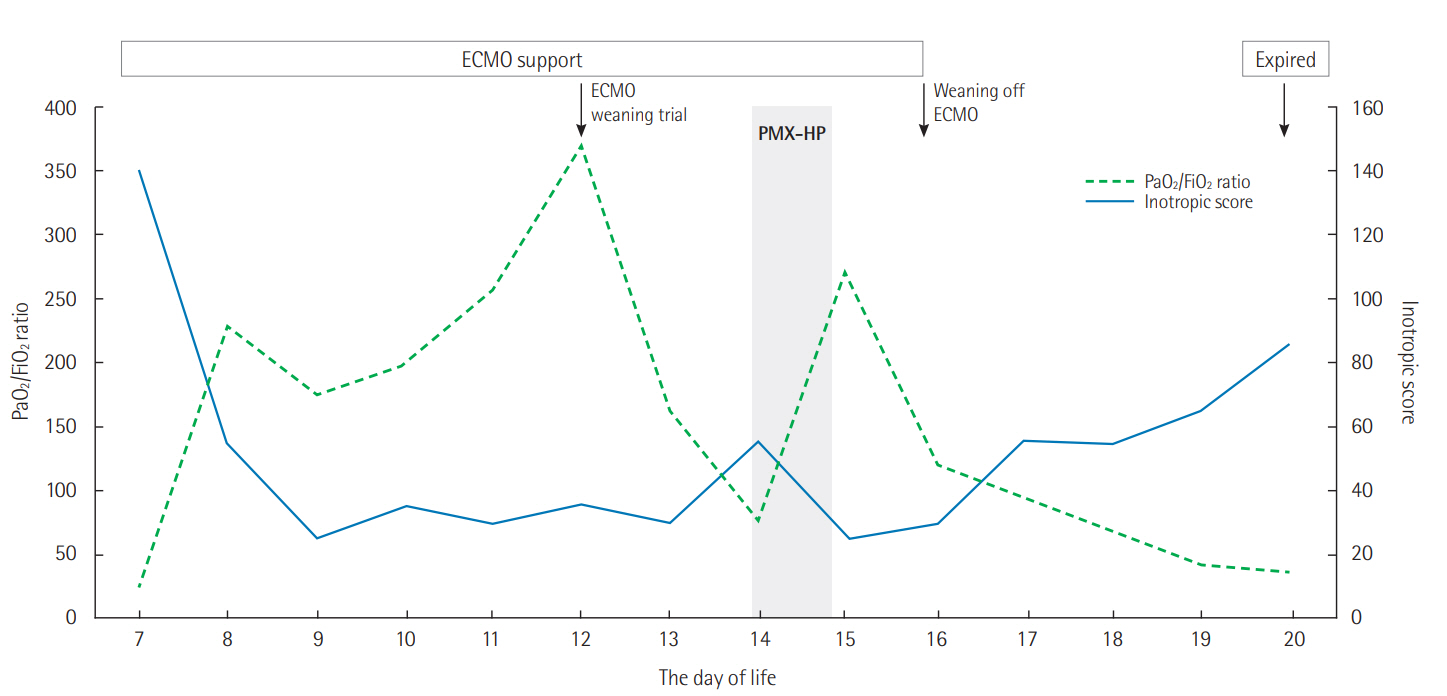
Figure 2.Pictures of devices. (A) An adult polymyxin B-immobilized fiber column (gray arrow) with a circuit and a hemofiltration set (white arrow) were placed on each device. (B) The access lines of the polymyxin B direct hemoperfusion device and continuous renal replacement therapy were simultaneously connected to the proximal drainage line of the extracorporeal membrane oxygenation circuit, their return lines were connected to the distal drainage line.

- 1. Cruz DN, Perazella MA, Bellomo R, de Cal M, Polanco N, Corradi V, et al. Effectiveness of polymyxin B-immobilized fiber column in sepsis: a systematic review. Crit Care 2007;11:R47. ArticlePubMedPMC
- 2. Cruz DN, Antonelli M, Fumagalli R, Foltran F, Brienza N, Donati A, et al. Early use of polymyxin B hemoperfusion in abdominal septic shock: the EUPHAS randomized controlled trial. JAMA 2009;301:2445-52.ArticlePubMed
- 3. Mitaka C, Tomita M. Polymyxin B-immobilized fiber column hemoperfusion therapy for septic shock. Shock 2011;36:332-8.ArticlePubMed
- 4. Shoji H, Tani T, Hanasawa K, Kodama M. Extracorporeal endotoxin removal by polymyxin B immobilized fiber cartridge: designing and antiendotoxin efficacy in the clinical application. Ther Apher 1998;2:3-12.ArticlePubMed
- 5. Machado JR, Soave DF, da Silva MV, de Menezes LB, Etchebehere RM, Monteiro ML, et al. Neonatal sepsis and inflammatory mediators. Mediators Inflamm 2014;2014:269681. ArticlePubMedPMCPDF
- 6. Hussein MH, Kato T, Sugiura T, Daoud GA, Suzuki S, Fukuda S, et al. Effect of hemoperfusion using polymyxin B-immobilized fiber on IL-6, HMGB-1, and IFN gamma in a neonatal sepsis model. Pediatr Res 2005;58:309-14.ArticlePubMed
- 7. Tani T, Hanasawa K, Kodama M, Imaizumi H, Yonekawa M, Saito M, et al. Correlation between plasma endotoxin, plasma cytokines, and plasminogen activator inhibitor-1 activities in septic patients. World J Surg 2001;25:660-8.ArticlePubMedPDF
- 8. Hirakawa E, Ibara S, Tokuhisa T, Hiwatashi S, Hayashida Y, Maede Y, et al. Septic neonate rescued by polymyxinB hemoperfusion. Pediatr Int 2013;55:e70-2.ArticlePubMed
- 9. Maede Y, Ibara S, Tokuhisa T, Ishihara C, Hirakawa E, Matsui T, et al. Polymyxin B-immobilized fiber column direct hemoperfusion and continuous hemodiafiltration in premature neonates with systemic inflammatory response syndrome. Pediatr Int 2016;58:1176-82.ArticlePubMed
- 10. Pollack MM, Patel KM, Ruttimann UE. PRISM III: an updated pediatric risk of mortality score. Crit Care Med 1996;24:743-52.ArticlePubMed
- 11. Wernovsky G, Wypij D, Jonas RA, Mayer JE Jr, Hanley FL, Hickey PR, et al. Postoperative course and hemodynamic profile after the arterial switch operation in neonates and infants: a comparison of lowflow cardiopulmonary bypass and circulatory arrest. Circulation 1995;92:2226-35.ArticlePubMed
- 12. Tani T, Shoji H, Guadagni G, Perego A. Extracorporeal removal of endotoxin: the polymyxin B-immobilized fiber cartridge. Contrib Nephrol 2010;167:35-44.ArticlePubMed
- 13. Ikeda T, Ikeda K, Nagura M, Taniuchi H, Matsushita M, Kiuchi S, et al. Clinical evaluation of PMX-DHP for hypercytokinemia caused by septic multiple organ failure. Ther Apher Dial 2004;8:293-8.ArticlePubMed
- 14. Takeyama N, Noguchi H, Hirakawa A, Kano H, Morino K, Obata T, et al. Time to initiation of treatment with polymyxin B cartridge hemoperfusion in septic shock patients. Blood Purif 2012;33:252-6.ArticlePubMed
- 15. Payen DM, Guilhot J, Launey Y, Lukaszewicz AC, Kaaki M, Veber B, et al. Early use of polymyxin B hemoperfusion in patients with septic shock due to peritonitis: a multicenter randomized control trial. Intensive Care Med 2015;41:975-84.ArticlePubMedPMCPDF
- 16. Iwagami M, Yasunaga H, Doi K, Horiguchi H, Fushimi K, Matsubara T, et al. Postoperative polymyxin B hemoperfusion and mortality in patients with abdominal septic shock: a propensity-matched analysis. Crit Care Med 2014;42:1187-93.ArticlePubMed
- 17. Fujii T, Ganeko R, Kataoka Y, Furukawa TA, Featherstone R, Doi K, et al. Polymyxin B-immobilized hemoperfusion and mortality in critically ill adult patients with sepsis/septic shock: a systematic review with meta-analysis and trial sequential analysis. Intensive Care Med 2018;44:167-78.ArticlePubMedPDF
References
Figure & Data
References
Citations
Citations to this article as recorded by 
- Polymyxin B Hemoperfusion in Pediatric Septic Shock: Single-Center Observational Case Series
Patcharin Saetang, Rujipat Samransamruajkit, Kanokwan Singjam, Tawatchai Deekajorndech
Pediatric Critical Care Medicine.2022; 23(8): e386. CrossRef - Controlling an Outbreak of Multidrug-resistant Acinetobacter baumannii in a Pediatric Intensive Care Unit: a Retrospective Analysis
Joung-Hee Byun, Su Eun Park, Minhae Seo, Jeungmi Jang, Mi Sun Hwang, Ju Yeoun Song, Chulhun L. Chang, Young A Kim
Journal of Korean Medical Science.2021;[Epub] CrossRef - Effects of continuous renal replacement therapy with the AN69ST membrane for septic shock and sepsis-induced AKI in an infant: a case report with literature review of cytokine/mediator removal therapy in children
Naoto Nishizaki, Riko Ueno, Yuki Nagayama, Hanako Abe, Akina Matsuda, Akira Mizutani, Kaoru Obinata, Tadaharu Okazaki, Toshiaki Shimizu
Renal Replacement Therapy.2020;[Epub] CrossRef - Suggestions and tips regarding polymyxin B-immobilized fiber column direct hemoperfusion of neonates with sepsis
Naoto Nishizaki
Acute and Critical Care.2020; 35(3): 226. CrossRef - Case Report: Successful Use of Extracorporeal Therapies After ECMO Resuscitation in a Pediatric Kidney Transplant Recipient
Andrey Rybalko, Anna Pytal, Mikhail Kaabak, Nadejda Rappoport, Anuar Bidzhiev, Vasilii Lastovka
Frontiers in Pediatrics.2020;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite