
Articles
- Page Path
- HOME > Acute Crit Care > Volume 38(4); 2023 > Article
-
Image in Critical Care
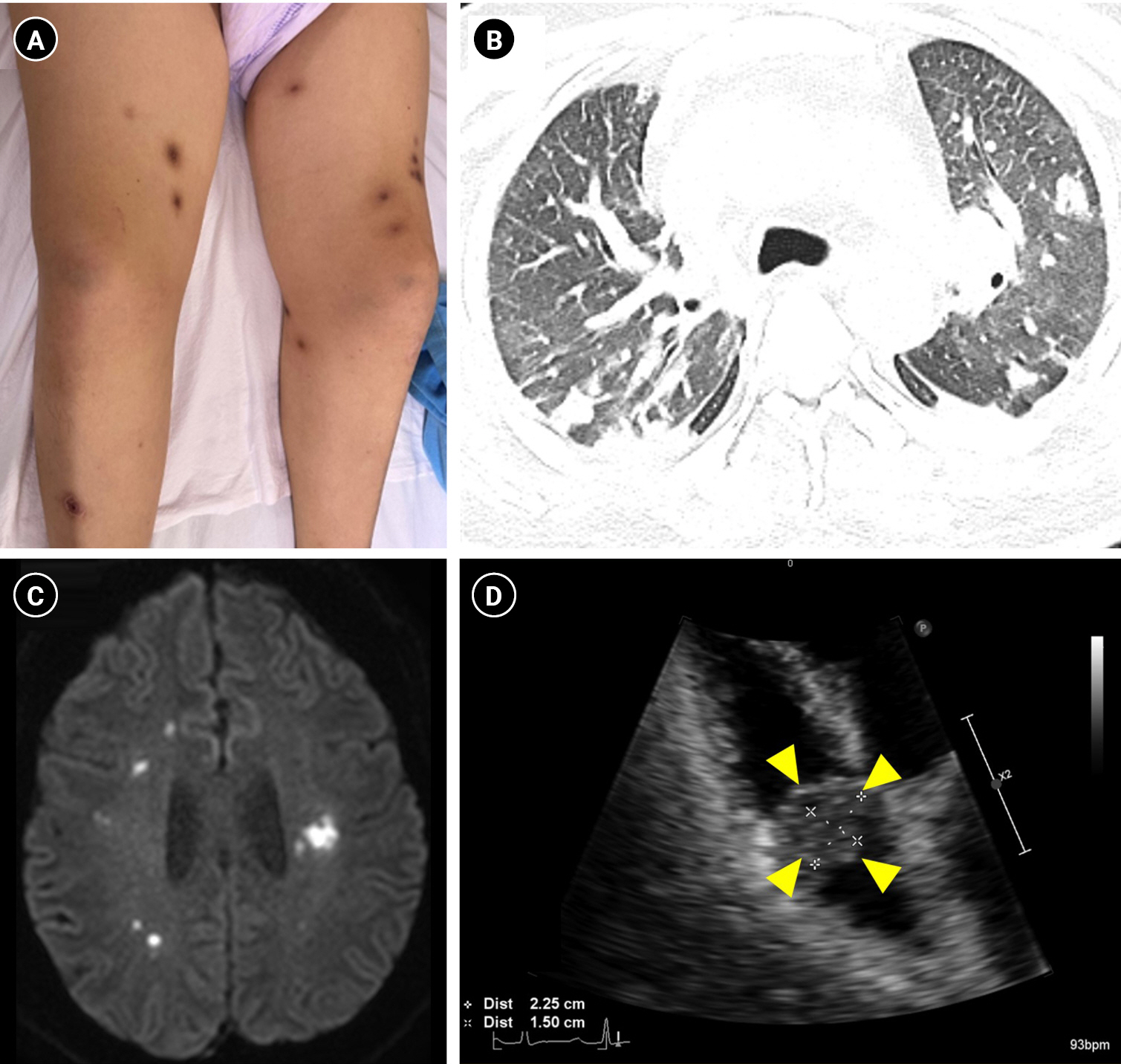
Infection Right-sided infective endocarditis of a native valve with multiple embolus lesions -
Miyeon Kim
 , Ki Yung Boo, Jeong Rae Yoo
, Ki Yung Boo, Jeong Rae Yoo -
Acute and Critical Care 2023;38(4):513-514.
DOI: https://doi.org/10.4266/acc.2023.01228
Published online: November 24, 2023
Department of Internal Medicine, Jeju National University College of Medicine, Jeju, Korea
- Corresponding author: Jeong Rae Yoo Division of Infectious Disease, Department of Internal Medicine, Jeju National University College of Medicine, 102 Jejudaehang-ro, Jeju 54987, Korea Tel: +82-64-717-2286, Fax: +82-64-717-2286 Email: mdyoojr@gmail.com
Copyright © 2023 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,023 Views
- 33 Download
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: JRY. Data curation: JRY, KYB. Formal analysis: JRY. Methodology: JRY, MK. Project administration: JRY. Visualization: JRY. Writing–original draft: MK. Writing–review & editing: JRY.
NOTES
Acknowledgments
SUPPLEMENTARY MATERIALS
Supplementary Video 1.
- 1. Shmueli H, Thomas F, Flint N, Setia G, Janjic A, Siegel RJ. Right-sided infective endocarditis 2020: challenges and updates in diagnosis and treatment. J Am Heart Assoc 2020;9:e017293. ArticlePubMedPMC
- 2. Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al, ESC Scientific Document Group. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 2015;36:3075-128.ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite

