Clinical Characteristics of Respiratory Extracorporeal Life Support in Elderly Patients with Severe Acute Respiratory Distress Syndrome
Article information
Abstract
Background
Extracorporeal membrane oxygenation (ECMO) strategy is proposed to reduce the ventilator-induced lung injury in acute respiratory distress syndrome (ARDS). As ECMO use has increased, a number of studies on prognostic factors have been published. Age is estimated to be an important prognostic factor. However, clinical evidences about ECMO use in elderly patients are limited. Therefore, we investigated clinical courses and outcomes of ECMO in elderly patients with ARDS.
Methods
We reviewed medical records of patients with severe ARDS who required ECMO support. Study patients were classified into an elderly group (≥ 65 years) and a non-elderly group (< 65 years). Baseline characteristics, ECMO related outcomes and associated factors were retrospectively analyzed according to group.
Results
From February 2011 to June 2013, a total of 31 patients with severe ARDS were treated with ECMO. Overall, 14 (45.2%) were weaned from ECMO, 9 (29.0%) survived to the general ward and 7 (22.6%) survived to discharge. Among the 18 elderly group patients, 7 (38.9%) were weaned from ECMO, 4 (22.2%) were survived to the general ward and 2 (11.1%) were survived to discharge. Overall intensive care unit survival was inversely correlated with concomitant acute kidney injury or septic shock.
Conclusions
In this study, ECMO outcome was poor in severe ARDS patients aged over 65 years. Therefore, the routine use of ECMO in elderly patients with severe ARDS is not warranted except in highly selective cases.
Introduction
Extracoporeal membrane oxygenation (ECMO) provides respiratory support to patients with severe acute respiratory distress syndrome (ARDS). Recent studies showed that transfer to an ECMO-capable hospital led to better outcomes in patients with severe ARDS.[1,2] However, most studies that supported efficacy of ECMO are the cohort studies of patients with H1N1 virus infection.[2–4] These results however are not enough to ensure the efficacy of ECMO in a general ARDS population. Nonetheless, the use of ECMO has sharply increased,[5] and this temporary life support system is expected to further rise of use. Increased use of ECMO has resulted in the findings of prognostic indicators for patients undergoing ECMO, promoting further studies to identify useful prognostic indicators. Among reported prognostic markers, age is regarded important predictive variable, and a retrospective study reported a negative correlation between age and the efficacy of ECMO.[6] However, the mean age of subjects was the middle age (40s) in the above- mentioned study, making it difficult to apply its results to the group of elderly aged 65 or over. The incidence of ARDS increases with age, showing a sharp increase in elderly aged 65 or over,[7] and the role of ECMO in elderly patients with severe ARDS is quite worth exploring. This study was aimed to identify clinical characteristics and prognostic indicators in severe ARDS patients aged 65 years or older who underwent ECMO in a tertiary-care hospital.
Materials and Methods
1) Subjects
We conducted a retrospective analysis of clinical data from patients who presented with severe ARDS from February 2011 to June 2013 and underwent ECMO because their PaO2/FiO2 ratio remained less than 100 despite maximum setting of mechanical ventilation (MV). ARDS were defined according to the Berlin definition,[8] and the cases of pretransplant ECMO were excluded from the analysis.
2) A protocol for extracoporeal membrane oxygenation placement
Extracoporeal membrane oxygenation equipment
To perform venovenous ECMO, poly (4-methyl-2-pentyne) membrane materials and a centrifugal pump (QUADROX PLS OXYGENATOR & ROTAFLOW pump, Maquet, Germany) were used along with the 17–24Fr. cannulae inserted via the femoral and jugular veins. For extracorporeal CO2 removal, the pumpless arteriovenous ECMO (iLA; Novalung, Talheim, Germany) was applied using Seldinger technique for the femoral arterial and venous cannulation. Ultrasound was used to detect any blood vessel abnormality and assess the arterial and venous diameters before cannulation.
Mechanical ventilation strategy during extracorporeal membrane oxygenation
Once ECMO was established, the ventilator was adjusted based on the arterial blood gas analysis (ABG) to keep an inspiratory plateau pressure below 28 cmH2O, initial tidal volumes at 6 ml/kg predicted body weight, positive end-expiratory pressure (PEEP) between 8 and 10 cmH2O, respiratory rate between 12 and 20 breaths/min, and FiO2 below 60%.
Sedation strategy
Analgesia-based regimen was used in combination with sedative drugs to reach a Ramsay score of 3, and further sedative drugs including neuromuscular blocker were given for deeper sedation.
Anti-coagulant strategy
Heparin was given with the goal of achieving an aPTT greater than 1.5 times control. Nafamostat (Futhan) was used as a substitute for heparin based on the platelet count, coagulation test results and the presence of hemorrhagic complications.
3) Methods
The patients were divided into two groups: an elderly group (age ≥ 65) and a non-elderly group (age < 65), and baseline clinical characteristics, variables associated with MV and outcome were investigated.
Baseline clinical characteristics
Patient characteristics were evaluated before and after ECMO using age, sex, height, weight, Acute Physiology and Chronic Health Evaluation (APACHE) II, Sequential Organ Failure Assessment (SOFA) scores, Murray score, the primary cause of ARDS and the presence or absence of acute kidney injury and sepsis. Acute kidney injury can be described as urine output of less than 0.5 ml/kg/h for 12 hours.
Baseline variables related to mechanical ventilation
Variables related to pre-ECMO ventilation included duration of MV, initial ventilator setting, arterial blood gas interpretation and the application of adjunctive therapies of ARDS.
Outcome variables
Outcome variables were evaluated using hospital and intensive care unit (ICU) length of stay, rate of successful weaning, ICU and hospital mortality rates and the presence or absence of ECMO-related complications. The incidence of complications of ECMO was evaluated based on bleeding, thrombosis, hemolysis and the frequency of hospital-acquired infection.
4) Data analysis
Collected data were analyzed using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA). Statistics tests used in this study included descriptive statistics and chi-square test. Cox proportional hazard model was also used to determine the relative risk of ICU mortality.
Results
A total of 31 ARDS patients underwent ECMO from February 2011 to June 2013. Of those, 14 (45.2%) were weaned off ECMO, 9 (29.0%) were sucessfully discharged from ICU and 7 (22.6%) were successfully discharged from hospital. The ICU and hospital mean lengths of stay were 22.7 ± 14.8 days and 35.1 ± 31.4 days, respectively.
1) Age-related differences in baseline characteristics
The mean APACHE II and SOFA scores of total patients were 19.3 ± 5.5 and 11.2 ± 4.9, respectively, and the mean Murray score was 3.0 ± 0.4. The mean duration of MV was 4.2 ± 5.6 days before ECMO, and the mean duration of ECMO was 11.8 ± 8.6 days. Of 31 patients, 13 (41.9%) had septic shock and 19 (61.3%) presented with acute kidney injury. Among the patients with acute kidney injury, 14 (73.7%) required renal replacement therapy. Age-related differences in baseline clinical characteristics are presented in Table 1. The mean height was smaller, and the mean APACHE II score was lower in the elderly group than those in the non-elderly group. However, there were no significant differences between the two groups with respect to other clinical features.
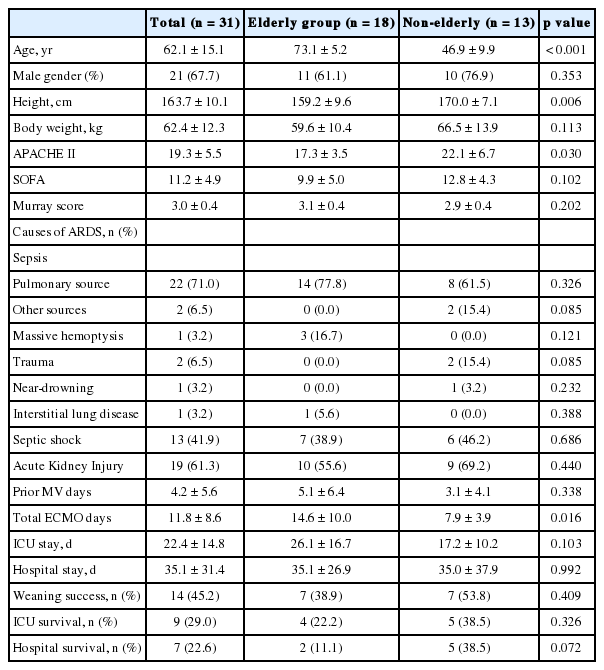
Baseline demographic feature and outcome of the study population
2) Age-related differences in baseline ventilation settings
In total patients, baseline ventilation settings showed PaO2/FiO2 of 76.3 ± 21.9, PEEP of 11.1 ± 3.6 cmH2O, tidal volume of 370.6 ± 96.6 ml and plateau pressure of 28.8 ± 4.8 cmH2O. However, no statistically significant differences in baseline ABG analysis, MV settings and the frequency of applied adjunctive therapies between the two groups (Table 2).
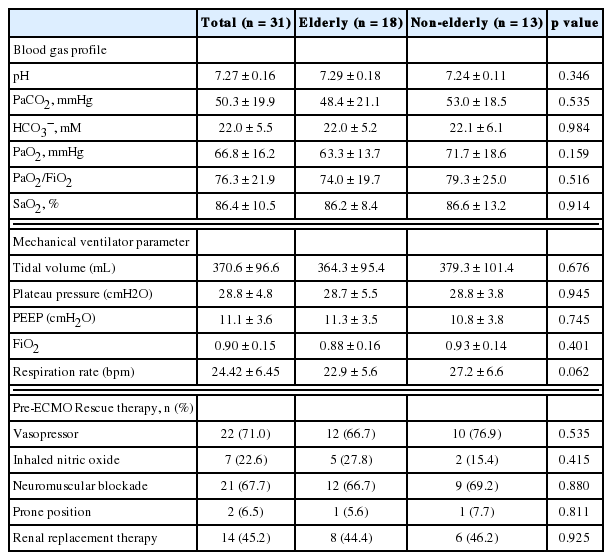
Baseline parameter and variables before application of ECMO by age group for ARDS
3) Age-related differences in outcomes
There were no statically significant differences in successful weaning rate, ICU and hospital survival rates between the two groups (Table 1). Multivariate analysis revealed that ICU survival rate were affected by baseline septic shock or acute kidney injury, showing a significantly lower ICU survival rate among patients with septic shock or acute kidney injury at baseline (Table 3). By group, 5 of 7 patients who were successfully weaned off ECMO were successfully discharged to home in the non-elderly group, whereas only 2 of 7 successfully weaned patients were discharged to home in the elderly group. In the elderly group, the cause of death after weaning ECMO included ventilator-associated pneumonia in 3 patients, acute exacerbation of interstitial pneumonia in one patient and barotrauma in one patient. In the non-elderly group patient, multiorgan dysfunction syndrome was the single cause of death in 2 patients.

Factors associated with intensive care unit mortality
4) Age-related differences in extracorporeal membrane oxygenation complications
Bleeding was the most common complication of ECMO because it occurred in 20 (64.5%) of total patients, whereas catheter thrombosis occurred in 3 patients (6.5%). Hospital-acquired infection occurred in 7 (22.6%) of 31 patients, and all of them are in the older age group. Of those, 4 (16.1%) suffered from ventilator-associated pneumonia, showing the largest number of infections.
Discussion
This study showed a lower hospital survival rate after ECMO in severe ARDS patients aged 65 or older than that in the younger age group. Septic shock and acute kidney injury constituted the significant risk factors of ICU mortality in total patients. Among complications developed after ECMO, ventilator-associated pneumonia were significantly evident in the elderly group, and pneumonia led to repeated aggravation even after successful ECMO weaning.
ECMO was widely used as a therapeutic strategy for severe ARDS during the 2009 HINI pandemic. Since then, the use of ECMO has sharply increased in the international clinical context.[5] Increased ECMO experiences led to the improvement in patient outcome.[1–4] Despite increasing cases of ECMO in Korea, a national ECMO registry has not been established and studies that explored the application of ECMO for ARDS are limited. The incidence of ARDS increases with age, meaning that the sudden demand for ECMO support increases in the elderly population. However, clinical criteria or guidance for the use of ECMO are not yet fully developed. Given the circumstances, we addressed ECMO implemented at a tertiary-care hospital for severe ARDS patients and investigated clinical characteristics of severe ARDS patients aged 65 or older.
This study found the mean ICU and hospital survival rates at 29.0% and 22.6%, respectively, which are lower than the survival rates reported in the extracorporeal life support organization (ELSO) registry.[6] The lower survival rates found in this study can be explained by various variables including age of subjects. The subjects of this study has a poor prognostic factors identified in a previous report, such as age, weight and Asian race.[6] The proportion of aged subjects is higher in this study, compared with previous studies of ECMO. Recent studies claimed age as an important prognostic indicator in patients receiving ECMO. Schmidt et al.[9] reported the outcomes of ECMO were unfavorable in patients aged 45 or older. In this study, the mean age was 46.9 years in the non-elderly group, and their survival-to-discharge rate was 38.5% on average, which is close the survival rate reported to the previous studies.[3–5] However, the mean age of the elderly group was 73.1 and their survival-to-discharge rate was very low at 11.1%, thereby indicating a possible association between age and unfavorable overall outcomes among total patients. It was not possible to verify this assumption due to the small sample size, requiring well-designed, prospective studies.
The low hospital survival rate in this study was also explained by high frequency of baseline septic shock (41.9%) and renal failure that required renal replacement therapy (45.2%). These two variables served as independent risk factors of ICU mortality according to multivariate analysis (Table 4). In ARDS patients, multiple organ failure and sepsis are associated with unfavorable outcome.[10] In particular, the association of renal impairment with unfavorable outcome has been discussed in several studies.[11–16]

ECMO related complications
As mentioned earlier, the survival rate of the elderly group was much lower than that reported in the ELSO registry, suggesting the possibility of a high frequency of reaggravations even after successful ECMO weaning. In other words, repeated aggravation resulted in a low survival-to-discharge rate (11.1%) in the elderly group whereas successful ECMO weaning was translated into a higher survival-to-discharge rate (38.5%) in the non-elderly group. Ventilator-associated pneumonia (3 cases), barotrauma (1 case) and deteriorated interstitial pneumonia (1 case) were major causes of repeated exacerbation. The first two variables were also associated with prolonged MV after ECMO removal. The need for prolonged ventilation after ECMO is supported by the claims that pulmonary dysfunction can continue in elderly patients who recovered from ARDS[15] and that an old age of over 70 is itself an unfavorable prognostic indicator in patients with severe ARDS.[16] That is, a slow recovery in the older age group druing ECMO lengthens the duration of ECMO (Table 1), increasing the duration of ventilation and the risk of developing pneumonia as a result. This finding suggests the importance of giving thorough consideration to the reversibility of elderly patients with severe ARDS when using ECMO.[17]
This study has several limitations, including a small number of subjects selected within a particular institution and a retrospective analysis. This study contain the result of initial period of ECMO program in our hospital. Therefore, the caution is needed to interpret our results. However, study provides insights into the current ECMO practices for severe ARDS patients in Korea. Also, given the consistency between the results of this study and retrospective studies based on data from the ELSO registry, the results of this study can be useful when employing ECMO. The low ICU survival rate in the elderly group signifies a need to consider reversibility and apply ECMO selectively in this population.
Recently, assessment tools for predicting the outcome of ECMO have been developing.[18,19] To improve outcome in patients with severe ARDS who require ECMO, early outcome predictors tailored for Korean patients should be developed by analyzing prognosis and associated variables. In conclusion, a national ECMO registry is definitely required for data collection.
Acknowledgements
This work was supported by a 2-Year Research Grant of Pusan National University.
Notes
No potential conflict of interest relevant to this article was reported.