Effects of ketamine on the severity of depression and anxiety following postoperative mechanical ventilation: a single-blind randomized clinical trial in Iran
Article information

Abstract
Background
In this study, we compare the effects of ketamine and the combination of midazolam and morphine on the severity of depression and anxiety in mechanically ventilated patients after discharge from the intensive care unit (ICU).
Methods
This randomized single-blind clinical trial included 50 patients who were candidates for craniotomy and postoperative mechanical ventilation in the ICU of 5 Azar Teaching Hospital in Gorgan City, North Iran, from 2021 to 2022. Patients were allocated to two groups by quadruple block randomization. In group A, 0.5 mg/kg of ketamine was infused over 15 minutes after craniotomy and then continued at a dose of 5 µ/kg/min during mechanical ventilation. In group B, midazolam was infused at a dose of 2–3 mg/hr and morphine at a dose of 3–5 mg/hr. After patients were discharged from the ICU, if their Glasgow Coma Scale scores were ≥14, Beck’s anxiety and depression inventories were completed by a psychologist within 2 weeks, 2 months, and 6 months after discharge.
Results
The mean scores of depression at 2 months (P=0.01) and 6 months (P=0.03) after discharge were significantly lower in the ketamine group than in the midazolam and morphine group. The mean anxiety scores were significantly lower in the ketamine group 2 weeks (P=0.006) and 6 months (P=0.002) after discharge.
Conclusions
Ketamine is an effective drug for preventing and treating anxiety and depression over the long term in patients discharged from the ICU. However, further larger volume studies are required to validate these results.
INTRODUCTION
As intensive care unit (ICU) care can be accompanied by severe psychological stress in patients [1], millions of ICU survivors live with new-onset mental issues that have short- or long-term consequences leading to reductions in patients' quality of life [2]. Egerod et al. [3] reported that 23%–48% and 17%–43% of discharged ICU patients had symptoms of anxiety and depression, respectively. Wu et al. [4] also reported in 2018 that 10%–17% of discharged ICU patients experienced symptoms of depression, anxiety, and stress. Hatch conducted a large-scale prospective cohort study of 21,633 ICU patients hospitalized after trauma and reported that of the remaining 4,943 patients in the study, 46%, 40%, and 22% showed symptoms of anxiety, depression, and stress, respectively [5]. Intensivists have sought to improve the outcomes of such patients through interventions such as physiotherapy [6], post-ICU counseling clinics, and rehabilitation and cognitive therapy programs [7]. Unfortunately, despite extensive efforts, the rates of patient improvement have not been significant [8].
However, pharmacological approaches such as ketamine infusions are promising, but are not well evaluated. As an anesthetic induction drug with strong effects on the glutamate system of the central nervous system, ketamine effectively blocks the N-methyl-D-aspartate (NMDA) receptor and is a very strong pain killer [9]. In addition, this drug has rapid antidepressant effects and is used in the treatment of major and chronic depression [6].
As ketamine is simultaneously a strong pain controller and sedative, we predicted that its administration would reduce the use of additional analgesics and sedatives that are associated with worse clinical and mental outcomes. There are a few studies [10,11] about the positive effects of ketamine on postoperative depression and anxiety, but they focus mostly on short term effects. This study was conducted to compare the effects of ketamine on the severity of depression and anxiety with those of a combination of midazolam and morphine in mechanically ventilated post-craniotomy patients from treatment in the ICU until 6 months after discharge.
MATERIALS AND METHODS
This study was approved from the Ethics and Research Committee of Golestan University of Medical Sciences (No. IR.GOUMS.REC.1399.318). The study was a single-blind randomized clinical trial that entered the implementation stage after obtaining permission from the Ethics Committee of Golestan University of Medical Sciences and registration in the IRCT system (IRCT20170413033408N5). Before registration, all participants read and signed a written informed consent form. A copy of the signed consent form was given to each participant. The guidelines on research involving the use of human subjects (beneficence, non-maleficence, veracity, confidentiality, and voluntarism) were strictly adhered to in accordance with the Helsinki Declaration. Participants did not incur any cost by participating in this study and there was no financial inducement.
The study population included 18- to 60-year-old patients who were hospitalized for craniotomy to treat non-traumatic brain lesions (such as brain tumors, non-traumatic intracerebral hemorrhage, and hydrocephalus) in the neurosurgery department of 5 Azar Teaching Hospital, Gorgan City, North Iran. The exclusion criteria included people suffering from drug poisoning, patients with suicidal attempts, receiving cardiopulmonary resuscitation, with cerebral dementia and Alzheimer's, or with extensive cerebral hemorrhage. In addition, patients were required to have received at least 48 hours of mechanical ventilation after craniotomy in the ICU. We also excluded cases with confirmation of brain damage and encephalopathy, cardiac arrest, and CPR during hospitalization and treatment of the patient in the hospital, Glasgow Coma Scale (GCS) <14/15 at the time of discharge from the ICU, and withdrawal of consent from this study.
For included patients, an anesthesiologist visited each patient the day before surgery, fully explained the purpose of this study, and obtained written consent to participate in the study. The participants were assigned to either the ketamine group (intervention group) or the midazolam and morphine group (control group) using a four-way block randomization method. Allocation of groups was performed by the anesthesiologist. The anesthesiologist and medical staff who took care of the participants were not blinded to the assigned groups. However, the participants, the psychologist, and the test evaluator were blinded to group allocation.
The ketamine group received with intravenous ketamine (0.5 mg/kg) within 15 minutes after admission to the ICU while remaining intubated. Following the loading dose, ketamine was infused at a dose of 5 µ/kg/min continuously for at least 48 hours and at the most until extubation. In the midazolam and morphine group, an infusion of 2–3 mg/hr midazolam and 3–5 mg/hr morphine was used to sedate the participants while receiving mechanical ventilation. In both groups, a bolus of 10 to 20 mg propofol was used as a rescue sedative. After extubation and discharge of the patient from the ICU, if the GCS score was ≥14 and the patient was able cooperate by answering questions, she/he would be referred to the psychiatric clinic for an interview. The first interview was a face-to-face interview by a psychologist, 2 weeks after being discharged from the ICU. The second and third interviews were conducted by telephone 2 months and 6 months after discharge. While collecting each patient's demographic information, the duration of mechanical ventilation and the length of stay in the ICU were also collected in a checklist designed for this purpose.
Diagnosis of Mental Disorder
The severities of depression and anxiety were evaluated based on the Beck inventory. Both inventories have 21 questions, with total scores ranging from 0 to 63. In the depression questionnaire, scores of 0–9 indicate the absence of depression, scores of 10–18 indicate mild to moderate depression, scores of 19–29 indicate moderate to severe depression, and scores of 30–63 indicate severe depression. In the anxiety questionnaire, scores of 0–7 indicate no or very low anxiety, scores of 8–15 indicate mild anxiety, scores of 16–25 indicate moderate anxiety, and scores of 26–63 indicate severe anxiety [12]. Ghassemzadeh et al. [13] confirmed the validity and reliability of the Beck depression questionnaire in the Iranian context in a study in 2005, and Salari-Moghaddam confirmed the validity and reliability of the Beck anxiety questionnaire in Iran in a study in 2018 [14].
Statistical Analysis
The quantitative and qualitative data are presented as mean values (standard deviation) and frequency (percentage), respectively. Independent Student t-tests were used to compare the means in the two groups and analysis of variance was used for three or more groups. Repeated measures analysis of variance was used for simultaneous intra-group and inter-group inferences. P-values <0.05 were considered statistically significant. Stata version 12 (Stata Corp.) was used for all statistical analyses. Sample size was calculated with G*Power software version 3.1.9.4 using the mean and standard deviation of the results of Ionescu et al. [15]. Based on an effect size of d=0.821, a power of 80%, and a two-sided α risk of 5%, 56 patients were required (28 per arm) including dropouts.
RESULTS
In this study, 56 patients who underwent craniotomy at 5 Azar Teaching Hospital in Gorgan City, North Iran, were subjected to postoperative mechanical ventilation in the ICU (Figure 1). We included 25 patients in each group who were able to cooperate until the end of the study and whose data were subjected to statistical analysis. The demographic characteristics of the study participants are shown in Table 1. Most of the patients in the ketamine group (59%) and in the control group (68%) were male, and this difference was not statistically significant (P=0.37). The variables of height, weight, body mass index, underlying diseases, underlying psychiatric history, and type of surgery were not significantly different between the two groups. The length of stay in the ICU and the duration of mechanical ventilation received by the patients are shown in Table 1. Here, too, the differences between the two groups were not statistically significant.
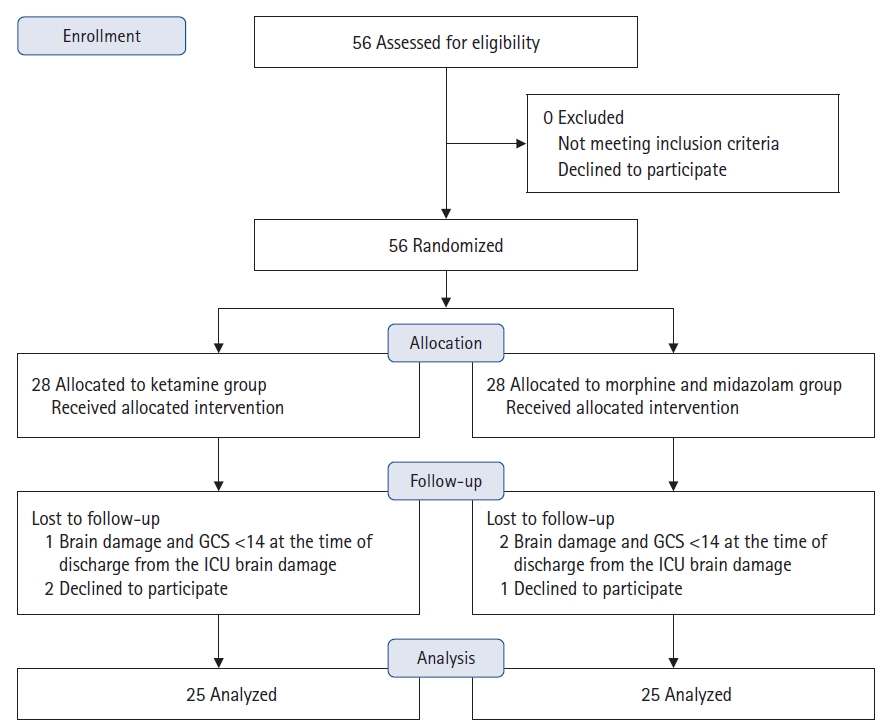
Consolidated Standards of Reporting Trials (CONSORT) diagram of patient recruitment. GCS: Glasgow Coma Scale; ICU: intensive care unit.

Demographic characteristics of participants
As shown in Table 2 and Figure 2, in patients who received ketamine, the mean scores for the depression severity test at 2 weeks, 2 months, and 6 months after discharge from the ICU were 22 vs. 25 (P=0.28), 16 vs. 20 (P=0.01), and 8 vs. 11 (P=0.03) and the control group, respectively. The mean anxiety scores of the two groups are shown in Table 3 and Figure 3. At 2 weeks, 2 months, and 6 months after discharge from the ICU, the scores were 23 vs. 31 (P=0.006), 21 vs. 23 (P=0.09), and 10 vs. 14 (P=0.002) in the ketamine group and the control group, respectively.

Comparison of the scores of depression of the two groups
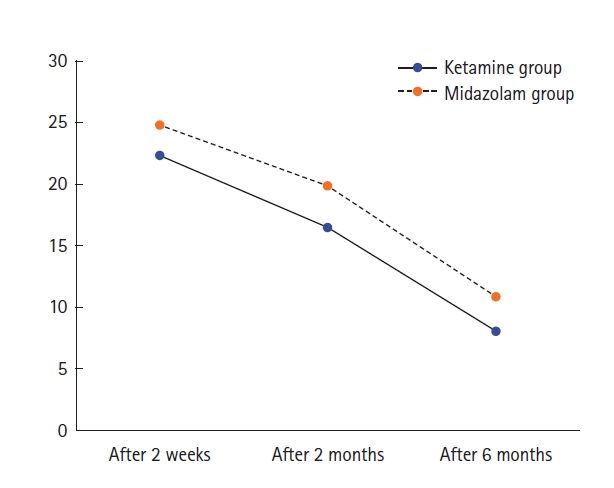
Changes in depression scores in the 6 months after discharge from the intensive care unit.

Comparison of the mean scores of anxiety of the two groups
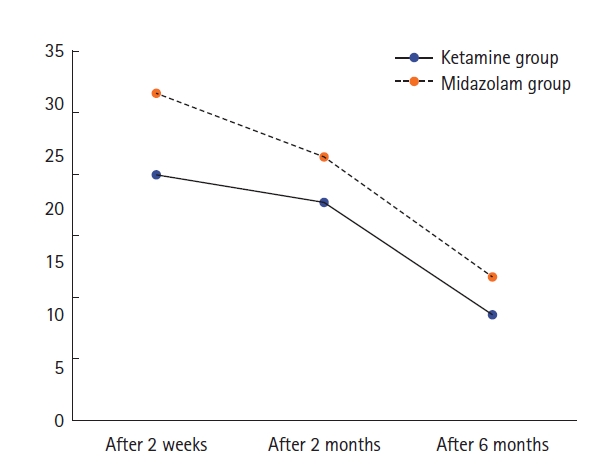
Changes in anxiety scores in the 6 months after discharge from the intensive care unit.
Repeated measures analysis of variance was used to evaluate the effect of time on the severity of depression and anxiety, as shown in Table 4. With the passage of time, the mean scores of anxiety and depression disorders in both groups of patients gradually decreased. Given that the prerequisite of sphericity was not met in this study (P=0.008), the Greenhouse Geisser method was used for analyses. The effect on the study group also became significant, indicating that depression and anxiety scores in the two groups receiving ketamine and a combination of midazolam and morphine were significantly different after controlling for the effect of time. The non-significance of the interaction coefficient between time and group type (P=0.71) for the variable of depression indicates that both the passage of time and the type of treatment had no significant effect on patients depression scores.
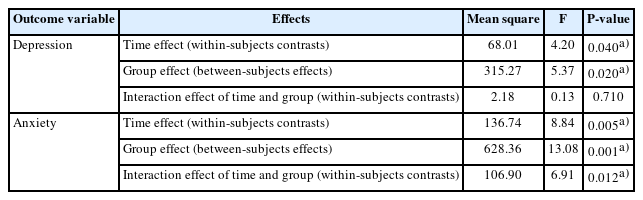
Results of analysis of variance for repeated measurements of depression and anxiety scores in participants
DISCUSSION
In this study, we found that the use of ketamine as the drug of choice for sedation of mechanically ventilated patients in the ICU is associated with promising results for the reduction of anxiety and depression. There are multiple hypotheses explaining the mechanism of action of ketamine as an antidepressant agent, including direct synaptic or extra-synaptic (GluN2B-selective) NMDAR inhibition, selective inhibition of NMDARs localized on GABAergic interneurons, and the role of α-amino-3-hydroxy-5-methyl-4-isoxazole-propionic acid receptor (AMPAR) activation [16,17]. Duman et al. [18] suggested that ketamine induces firing of GABA interneurons, resulting in glutamate bursts. Deyama and Duman [19] showed that ketamine rapidly increases brain-derived neurotrophic factor release and hippocampal neurogenesis. Zanos and Gould [16] found in 2018 that the proposed mechanisms of ketamine’s antidepressant actions are not mutually exclusive and may in fact complement each other to result in the unique antidepressant effects of the drug. Indeed, a net result of all these processes is a sustained potentiation of excitatory synapses in cortico-mesolimbic brain circuits involved in the maintenance of mood and stress-reactivity. There are additional mechanisms including ketamine’s effects on the monoaminergic systems, as well as its anti-inflammatory actions, which are postulated to be involved in the mechanisms underlying its antidepressant actions.
Previous studies have evaluated the effects of ketamine on prevention and treatment of patients with depression, with contradictory results observed. Zarate et al. observed that ketamine infusion could elicit a rapid and significant antidepressant response in patients with bipolar depression and rapidly improve suicidal thoughts in these patients [20]. However, Niciu et al. [21] found in 2013 that, at a subanesthetic dose, ketamine did not change mood in people with treatment-resistant major depression . In a study of 26 patients with major depression and suicidal thoughts, Ionescu et al. [15] observed that six infusions of 0.5 mg/kg ketamine over 45 minutes had no effect compared to placebo three months after treatment and did not reduce the symptoms of depression.
The primary objective of the present study is to evaluate the preventive effect of ketamine against depression and anxiety after craniotomy in patients without histories of depression or anxiety disorders. Several previous studies addressed the controversial effects of ketamine on postoperative depression. In 2023, Gan et al. [11] discussed the effect of esketamine on the occurrence of depressive symptoms in patients undergoing thoracoscopic lung cancer surgery. In that study, 156 patients received ketamine infusion during and 48 hours after surgery. Normal saline was administered to the control group and Beck's questionnaire was used to evaluate results. They found that depressive symptoms decreased 1 month after the operation [11]. In 2023, Zhang et al. [10] examined Crohn's patients undergoing intestinal resection treated with ketamine at a dose of 0.25 mg/kg as an intravenous drip and then with a dose of 0.12 mg/kg/hr. In the control group, 0.9% saline was used. In that study, low-dose ketamine reduced mild to moderate depressive symptoms without the risk of severe side effects [10].
In a review study, Pang et al. [22] evaluated 13 articles with 1,148 patients. According to their results, (R, S)-ketamine was no different from placebo in reducing depression after spinal and general anesthesia. On the other hand, in a meta-analysis of nine randomized clinical trials, Wang et al. [23] measured the effects of intravenous ketamine on depressive symptoms in 2,468 post-surgical patients, finding that ketamine had positive effects on reducing depressive symptoms despite the emergence of side effects. Similarly, in this study we used a 0.5 mg/kg ketamine bolus dose at the end of the operation, and 5 µ/kg/min infusion during at least 48 hours of postoperative mechanical ventilation. Based on our results, when administered in the form of a bolus and then an infusion, ketamine can reduce depression scores 2 and 6 months after treatment in patients discharged from the ICU compared to the control group. However, ketamine treatment was not successful in controlling depression 2 weeks after discharge or for controlling the occurrence of acute depression.
Fewer studies have been conducted evaluating the effects of ketamine on anxiety. In a systematic review in 2022, Tully et al. [24] showed that ketamine could be effective for improving anxiety, but the effect was temporary and after 2 weeks anxiety scores returned to the baseline level. In 2019, Glue et al. [25] investigated the effect of ketamine on patients with treatment-resistant generalized anxiety disorder and social anxiety disorder. Twelve patients were treated with increasing doses of ketamine (0.25, 0.5, 1 mg/kg) at weekly intervals. In the control group, midazolam was used at a dose of 0.01 mg/kg. The results of that survey indicated positive effects of ketamine for reducing anxiety symptoms [25].
There were a few limitations in the present study. First, the sedatives used in the control group were midazolam and lorazepam, which are the most commonly used benzodiazepines in ICU patients [26]. However, Hsu et al. [27] showed in 2015 that sedation with midazolam can lead to selective cognitive impairment or the prolongation of such impairment in patients. Therefore, the appropriate response of patients in this study to ketamine may be due to the lack of midazolam in these patients. In order to address this bias, we required that patients have a GCS score higher than 14 after being discharged from the ICU. Second, we were unable to obtain baseline depression and anxiety scores for patients. Therefore, we ensured that there were no between-group differences in psychiatric history. Third, this study was conducted in single center. Multiple randomized prospective trials worldwide are required to validate the results of this study.
In conclusion, in this study we found that ketamine was effective for reducing the severity of anxiety and depression, particularly in the long term, after ICU treatment. Our results suggest that ketamine is a treatment option for mental disorders in this patient population, but further research is needed to fully understand its short-term effects and confirm its efficacy. This study highlights the importance of timely intervention and appropriate drug therapy for addressing mental health issues in critically ill patients and emphasizes the need for continued research in this area.
KEY MESSAGES
▪ Ketamine can reduce the severity of anxiety disorders in patients undergoing mechanical ventilation, 2 weeks and 6 months after intensive care unit (ICU) discharge.
▪ Ketamine is effective to decrease depressive disorders in patients undergoing mechanical ventilation, 2 and 6 months after ICU discharge.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
This project was financially supported by the Deputy of Research and Technology of Golestan University of Medical Sciences in Iran.
AUTHOR CONTRIBUTIONS
Conceptualization: SM, FT. Data curation: SG, SM, HS. Formal analysis: FM. Methodology: SM, FT, SM, HS, RS. Project administration: SM. Visualization: SG. Writing–original draft: SM, FT, SG, FM. Writing–review & editing: all authors.
Acknowledgements
None.