Clinical Outcome and Prognosis of Patients Admitted to the Surgical ICU after Abdomen Surgery
Article information

Abstract
Background
Postoperative admission to the surgical intensive care unit (S-ICU) is commonly planned to prevent and treat complications, unnecessary admission to the S-ICU increases medical costs and length of hospital stay. This study aimed evaluated outcome and the predictive factors for mortality in patients admitted to the S-ICU after abdominal surgery.
Methods
The 168 patients admitted to the S-ICU immediately after abdominal surgery were reviewed retrospectively from January to December 2011.
Results
The mortality rate of patients admitted to the S-ICU after abdominal surgery was 8.9% (15 of 168). Two preoperative factors (body mass index [BMI] < 18.5 kg/m2 [p < 0.001] and serum albumin < 3.0 g/dL [p = 0.018]), two operative factors (the need for transfusion [p = 0.008] or vasopressors [p = 0.013] during surgery), and three postoperative variables (mechanical ventilation immediately following surgery [p < 0.001], sequential organ failure assessment [p = 0.001] and SAPS II [p = 0.001] score) were associated with mortality in univariate analysis. After adjusting for age, gender, and SAPS II by a Cox regression, which revealed that BMI < 18.5 kg/m2 (p < 0.001, hazard ratio [HR] 9.690, 95% confidence interval [CI] 2.990-25.258) and the use of mechanical ventilation on admission to S-ICU (p < 0.001, HR 34.671, 95% CI 6.440-186.649) were independent prognostic factors.
Conclusions
In patients in S-ICU after abdominal surgery, low BMI and postsurgical mechanical ventilation should be considered important predictors of mortality.
Introduction
Postoperative admission to the surgical intensive care unit (S-ICU) is commonly planned to prevent and treat complications, as postoperative complications are an important cause of surgery-related mortality and morbidity.[1] However, treatment of patients in the intensive care unit (ICU) increases medical costs and length of hospital stay, and many patients suffer from unfamiliar circumstances and excessive procedures in the ICU.[1-4] Thus, evaluation of predictive factors related to poor outcomes is required to ensure facilitate decision making regarding patient admission to the ICU after surgery.
Abdominal surgery causes various postoperative complications due to the presence of the gastrointestinal bacterial flora and long postoperative fasting periods.[5-9] In particular, pulmonary complications occur frequently in abdominal and thoracic surgery because of the decline in lung volume and respiratory depression due to pain during respiration and the effects of anesthesia.[5-9] Therefore many patients are admitted to the S-ICU after abdominal surgery, there are few studies for the outcome of patients in the S-ICU after abdominal surgery.
This study aimed to evaluated the clinical outcomes of patients in the ICU after abdominal surgery, and identify the prognostic factors contributing to mortality in these patients.
Materials and Methods
1) Setting and subjects
The study was performed in an 857-bed referral hospital in Seoul, Korea. It contains five ICUs including medical ICU (15 beds), surgical ICU (14 beds), cardiac ICU (seven beds), neurological ICU (18 beds), and neonatal ICU (12 beds).
We selected patients ≥18 years of age who were admitted to the ICU after abdominal surgery from January 2011 through December 2011. We excluded patients who underwent non-invasive procedures, such as abdominal wound dressing in the operating room and those who underwent urological, abdominal vascular and gynecological procedures. Malignancy was confirmed by surgical pathologic findings. Finally, 168 patients were evaluated retrospectively. The retrospective study was approved by the Institutional Review Board of Ewha Medical Center (IRB Number: ECT 12-10-02).
2) Variables
The analyzed preoperative variables included patient demographics, comorbidities, laboratory findings, smoking history. A low body mass index (BMI) was defined as ≤18.5 kg/m2 according to the World Health Organization criteria for BMI.[10] All patients were classified according to the American Society of Anesthesiologists (ASA) classification. Operative factors were evaluated by surgical site, duration of surgery, treatment during operation, whether the surgery was related to cancer, and the emergency state. We also analyzed the use of mechanical ventilation. Mechanical ventilation was started on admission to the ICU. The duration of ICU stay, Simplified Acute Physiology Score (SAPS) II, sequential organ failure assessment (SOFA), and laboratory findings were the postoperative variables.
3) Statistics
Statistical analysis was performed using the SPSS-PC software for Windows version 17.0 (SPSS Inc, Chicago, IL, USA). Descriptive data are expressed as medians with range and frequencies, which are expressed as numbers (%). Median value was used for the groups of SAPS II and SOFA scores. To identify the prognostic factors contributing to mortality, Cox proportional hazards models were used. The factors that were significantly associated with the mortality at a p value of <0.05 were included in the multivariate model. Age, sex, and SAPS II were also adjusted in the multivariate model. Hazard ratios (HRs) with 95% confidence intervals (CIs) were used to report the results. Cumulative survival probabilities were estimated by Kaplan Meier methods, and the log-rank test was applied to compare survival curves among patients according to BMI and use of mechanical ventilation.
Results
1) Clinical characteristics and outcome of ICU patients after abdominal surgery
The characteristics of the 168 patients are summarized in Table 1. The median age was 72 years (range, 18-90 years); 94 patients (56%) were male. The median BMI was 23.0 kg/m2 (range, 15.6-32.9 kg/m2). Some patients had combined morbidities including hypertension (50%), diabetes (20%), ischemic heart disease (12%), and cerebral disease (10%). Emergency and malignancy related operations were performed in 58 (35%) and 93 (55%) patients. Most patients (79, 47%) had an ASA classification of 2. Lower gastrointestinal and hepatobiliary operations were performed in 64 (38%) and 58 (35%) patients, respectively.

Clinical characteristics of patients in intensive care unit after abdominal surgery (n = 168)
The median duration of surgery was 207 min (range, 40-645 min). Sixty-four patients (28%) received transfusions during the operation and the median blood loss was 300 mL (range, 100-680 mL). During the operation, 21 patients (13%) were administered a vasopressor. The median hospital and ICU stays were 19 days (range, 1-72 days) and 2 days (range, 1-27 days). Most patients (121, 72%) were admitted to the ICU for simple monitoring after surgery; cardiovascular (22%) and respiratory events (2%) were the next most common reasons for admission to the ICU. The median SAPS II and SOFA scores upon admission to the ICU were 21 (range, 3-71) and 2 (range, 0-15). ICU mortality was 9 % (15 patients). Seven patients died of sepsis and three of pneumonia. Other causes of death were cerebral hemorrhage, gastric ulcer bleeding, cancer aggravation, and ischemic colitis. One patient died of cardiac arrest due to an unknown cause.
2) Prognostic factors of ICU patients after abdominal surgery
In univariate analysis, two preoperative factors (BMI <18.5 kg/m2 [p < 0.001] and a serum albumin <3.0 g/dL [p = 0.0092]), two operative factors including the need for transfusion (p = 0.008) and vasopressor (p = 0.013) during surgery), and three postoperative variables (acute respiratory failure requiring mechanical ventilation immediately following surgery [p < 0.001], SOFA score [p = 0.001] and SAPS II score [p = 0.001]) were associated with mortality. However old age, comorbid disease, cancer related operations, emergency operations, and longer operation times were not associated with mortality of patients admitted to the ICU after abdominal surgery (Table 2).
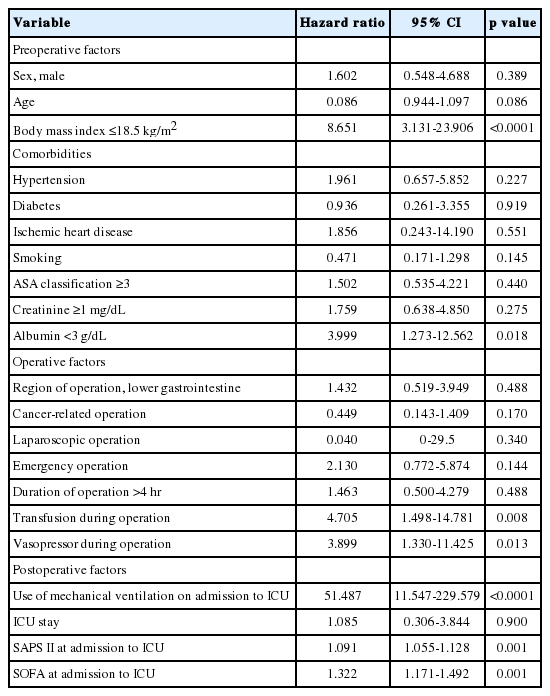
Univariate analysis of factors related to mortality of patients in the intensive care unit after abdominal surgery (n = 168)
The Cox regression hazard model adjust for age, sex, and SAPS II, revealed that a BMI < 18.5 kg/m2 (p < 0.001, HR 8.690, 95% CI 2.990-25.258) and mechanical ventilation after surgery (p < 0.001, HR 34.671, 95% CI 6.440-186.649) were independent predictive factors for mortality. The Kaplan-Meier survival curve showed that patients with a lower BMI and who required mechanical ventilation displayed higher mortality (Table 3 and Fig. 1).

Adjusted predictors related to mortality of patients in the intensive care unit after abdominal surgery
Survival curve according to BMI and mechanical ventilation for 168 patients admitted to the surgical intensive care unit after abdominal surgery. BMI: body mass index; ICU: intensive care unit.
Discussion
The data revealed that low BMI and postsurgical mechanical ventilation are associated with ICU mortality and poor prognosis of abdominal surgery patients.
Mortality of patients admitted to the ICU remains high, and the estimated mean overall ICU mortality in some studies is approximately 15%.[11] In the present study, the ICU mortality of patients after abdominal surgery was 9 %, higher than that of patients in the surgical ICU in other studies (2.4%-7.6%),[12,13] these values are however lower than the overall mortality in the general ICU or medical ICU. [11,14,15] Studies of post surgical complication and mortality have shown higher mortality rates for patients after thoracic and abdominal surgery or patients with other forms of surgery.[1,12] Mortality rates in our study were higher than mortality rates in other studies of the surgical ICU because our study only analyzed data on abdominal surgery, excluding other surgeries. The discrepancy between the mortality of patients in the ICU after abdominal surgery and that in the medical or overall ICU results from admission to the ICU after surgery for simple monitoring. This study showed that all 21 post-laparoscopy ICU patients who underwent relatively minor abdominal surgery survived. These patients were admitted to the ICU for simple postoperative monitoring due to old age, comorbid conditions or other reasons. ICU settings are expensive and have limited resources, and ICU patients suffer from unfamiliar circumstances and excessive procedures.[1-4] Thus, the decision to admit a patient to the ICU after abdominal surgery should be undertaken cautiously, taking into consideration the effective use of limited resources and the comfort of patients.
In our study, a low BMI was associated with higher mortality of ICU patients after abdominal surgery. Obesity of patients was risk factors for postoperative complications after heart,[16] uro-system,[17] and gynecologic[18] surgeries. However, other studies have found that BMI is not significantly correlated with severe postoperative morbidity or mortality with the exception of minor postoperative complications such as wound infection.[19-21] In patients with intra-abdominal cancer surgery, obesity was not elevated risk for postoperative complication and mortality, however, lower weight patients have increased risk of postoperative mortality about five fold.[9] Excessive subcutaneous fat and oxygen demands of tissue with relatively low blood flow and insufficient antibiotic levels in the tissues of obese patients result in increased risk of wound infection.[22] Whereas obese patients have adequate nutritional reserves, patients with a low BMI are in an insufficient nutritional state, and are relatively unprepared for the hyper-metabolic state and oxidative stress that occur after surgery.[9] In particular, abdominal surgery requires a longer fasting period than other operations. These factors seem to result in the high mortality of patients with a low BMI in the ICU after abdominal surgery.
In studies of BMI and mortality in Asian and Korean,[23-25] underweight and overweight person had higher rates of death than person of normal weight. The association of BMI with death varied according to the cause of death and was affected by age, sex, and smoking history.[23] Low BMI can be an indicator of certain other chronic medical conditions or of poor health or a low standard of living, which may contribute to such conditions as undernutrition and may increase the risk of premature death.[24] A trend of graded inverse association between BMI and hospital mortality was found in critically ill patients in Korean cohort study.[25] Although BMI did not have a significant influence on ICU mortality in Korean study,[26] BMI at ICU admission was a determinant of survival of 30 days and 12 months in other study.[27] Obesity was not associated with adverse outcomes.[27] These studies suggested that obesity in contrast to low BMI provides a nutritional reserve that, in times of stress and increased metabolic demand, helps to prevent the long-term complications associated with critical illness. In our study, the longer fasting time associated with abdominal surgery might have resulted in the association between prognosis and low BMI.
The postoperative use of a mechanical ventilator was associated with a poor outcome. This appears to be due to respiration failure after the operation, indicating hemodynamic, respiratory, and consciousness compromise. Postsurgical mechanical ventilation due to respiratory failure and pulmonary complications result in increasing hospital stays, morbidity, and mortality.[28] Thus, non-invasive ventilation may be considered a prophylactic and therapeutic tool for improving gas exchange in postoperative patients.[28] Insufficient deep breathing or sputum expectoration due to pain and diaphragm dysfunction leads to increased pulmonary complications after abdominal surgery, particularly for upper abdominal surgery including the stomach or hepato-biliary tract, which are closer to the diaphragm.[6] However, we did not find differences in the use of mechanical ventilation between upper-abdominal surgery and that at other sites in this study.
This study has a number of limitations. The most important is the small number of subjects. Second, we selected subjects retrospectively in a single medical center. However, a significant correlation was found between low BMI and mortality using a Cox proportional hazards model. Future, large, prospective cohort studies should be performed.
In conclusion, patients with a poor prognosis should be stratified to ensure effective use of the ICU. If patients have minor risk factor including old age, comorbid conditions or other reasons, physicians should cautiously decide whether ICU admission is necessary for simple postoperative monitoring. In patients ICU admission immediately after abdominal surgery, it should be considerable as important predictors which were low BMI and postsurgical mechanical ventilation.
Notes
No potential conflict of interest relevant to this article was reported.