Diffuse Alveolar Hemorrhage Confirmed by Bronchoalveolar Lavage in a Patient with Hemoptysis after Sildenafil Use for Erectile Dysfunction
Article information

Abstract
A 81-year-old man was referred for respiratory failure by emergency medical technicians. He admitted at intensive care unit for ventilator treatment. Several hours before admission, he took sildenafil 100 mg for erectile dysfunction without prescription. The episodes of hemoptysis occurred several hours later. Computed tomography revealed multifocal diffuse ground-glass attenuation in both lungs. And the more we performed bronchoalveolar lavage, the more the color of it was turned into red. We treated him with empirical antibiotics and tranexamic acid, and hemoptysis was stopped in one day after admission. But in the 5th admission day, he died from sepsis combined with pneumonia caused by Acinetobacter baumannii abruptly.
Sildenafil has treated more than 20 million patients for erectile dysfunction (ED).[1] In the literature, there are rare cases of hemoptysis confirmed by bronchoscopy after sildenafil use for ED. Here we report a case of diffuse alveolar hemorrhage confirmed by bronchoalveolar lavage (BAL) in a patient with hemoptysis after sildenafil use for ED.
Case Report
A 81-year-old man was referred to the emergency department for respiratory failure. During detailed questioning, his relatives stated that he had taken sildenafil 100 mg for ED without any prescription several hours ago before admission. At presentation, His blood pressure was 112/71 mmHg, heart rate was 96 beats/min, respiration rate was 39 breaths/min and body temperature was 37.2°C. Coarse breath sounds were audible without wheezing on auscultation of the chest. A complete blood count showed white blood cells (WBC) count of 15,510/μL, hemoglobin of 16.7 g/dL and a platelet count of 219,000/μL. A prothrombin time/international normalized ratio was 14.4 sec/1.12. Creatine kinase and tronin-T were 2.33 ng/mL and 0.018 mg/mL, respectively. Echocardiogram revealed normal sized left ventricle (LV) and LV ejection fraction of 57%. Chest computed tomography revealed multifocal diffuse ground-glass attenuation and patchy consolidation in both lungs (Fig. 1).
Chest computed tomography shows multifocal diffuse ground-glass attenuation and patchy consolidation in both lungs.
The episode of hemoptysis occurred after admitting at intensive care unit (ICU) for ventilator treatment, so we performed bronchoscopy. BAL was done in the left lower lobe. The more we performed washing, the more the color of it turned red (Fig. 2). BAL fluid analysis showed an increase in (RBCs) (of 124,000/μL versus WBC of 250/μL). He was diagnosed as a diffuse alveolar hemorrhage (DAH) induced by sildenafil. We treated him with empirical antibiotics and tranexamic acid, and hemoptysis was stopped in one day after admission. In the 5th admission day, he was transferred to general ward. But in the 6th admission day, he had a fever (39°C). Though we changed antibiotics as broad-spectrum (teicoplaninn and meropenem), pneumonia deteriorated rapidly and he eventually expired due to sepsis. 2 days after his death, the results of the blood cultures followed as Acinetobacter baumannii susceptible to only colistin.
Bronchoalveolar lavage (BAL) was done in the left lower lobe. And we can find the progressive hemorrhagic BAL in the serial samples (Number 1 is the first BAL, number 2 is the second BAL, and number 3 is the third BAL.). BAL fluid analysis shows an increase in red blood cells.
Discussion
The frequent causes of hemoptysis are malignancies, bronchiectasis and tuberculosis.[2] In our report, he didn’t have any other associated disease except taking sildenafil 100 mg. Through detailed information of relatives, we knew that he took benzodiazepine 5 mg together. Judging from the clinical manifestations of hemoptysis, diffuse radiographic pulmonary infiltration, and hypoxemic respiratory failure, we hypothesized that DAH was induced by sildenafil.[2-4]
The histopathology of DAH includes the presence of intraalveolar RBCs and fibrin and accumulation of hemosiderin-laden macrophages.[3] He was treated with ventilator due to respiratory failure, so we could not perform a lung biopsy. However, we conducted bronchoscopy with a endotracheal intubation state to confirm the clinical diagnosis of DAH.[5] Judging from an increase in RBCs of BAL fluid analysis and more reddish color of BAL increasingly, he was confirmed as DAH.
Few cases of hemoptysis after sildenafil take for ED (Table 1) has been reported previously (Yuncu et al[2] Dixit et al[6] and Pereira e Silva and Marchiori[5]). According to the previous reports,[2,5,6] the dose of sildenafil was 50 mg, and DAH was diagnosed by only radiographic imaging of diffuse pulmonary infiltration without carrying out BAL, respectively.
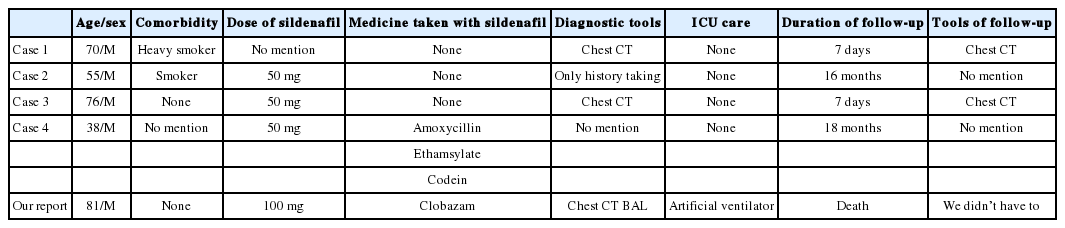
The comparison between previous reports and our report of diffuse alveolar hemorrhage after sildenafil use for erectile dysfunction
So, our report has the uniqueness compared to the previous reports.[2,5,6]
Firstly, the dose of sildenafil in our report was higher than the previous reports,[2,5,6] though the value of it was not checked directly.
In our report, he was older than reported patients[2,5,6] as 81-year-old, so we could expect the clearance of sildenafil was more decreased. And the dose of sildenafil was 100 mg in our report compared to 50 mg in previous reports.[2,5,6] The relative risk of sildenafil 100 mg related to almost adverse events is higher than 50 mg.[7] Additionally, because benzodiazepine and sildenafil are metabolized by using cytochrome3A4 enzymes, this can increase the sildenafil blood level.[8]
Secondly, the diagnosis of DAH was confirmed by not only chest computed tomography (CT) scans but also BAL. According to Lara et al[3] and Pereira e Silva and Marchiori,[ 5] the clinical diagnosis of alveolar hemorrhage is confirmed after sequential BAL reveals worsening RBC counts. In most of the previous studies[2,5,6], patients were diagnosed as DAH without BAL. But, we performed bronchoscopy to prove the clinical diagnosis of alveolar hemorrhage and we could find the progressive hemorrhagic BAL in serial samples (Fig. 2).
Common adverse effects are headache, dyspepsia, vision changes, and so on,[9] however we should consider hemoptysis in patients with sildenafil use after removing other risk factors. During taking the medical history, we should ask patients and acquaintances about all kinds and dose of medicine in detail. Especially, in cases of patients who are old age over 65-year-old, take high dose of sildenafil over 100 mg, accompany a coronary heart disease and take medicine together which elevates the sildenafil blood level, we should pay particular attention. Both the BAL and chest CT scan are more accurate diagnostic tools of DAH than the only chest CT scan to confirm the diagnosis of DAH. So we report the unique case of DAH confirmed by BAL in a patient with hemoptysis after sildenafil use for ED.
Notes
No potential conflict of interest relevant to this article was reported.