Extracorporeal Membrane Oxygenation Cannula Malposition in the Azygos Vein in a Neonate with Right-Sided Congenital Diaphragmatic Hernia
Article information
Abstract
Malposition of the extracorporeal membrane oxygenation (ECMO) venous cannula in the azygos vein is not frequently reported. We hereby present such a case, which occurred in a neonate with right-sided congenital diaphragmatic hernia. Despite ECMO application, neither adequate flow nor sufficient oxygenation was achieved. On the cross-table lateral chest radiograph, the cannula tip was identified posterior to the heart silhouette, which implied malposition of the cannula in the azygos vein. After repositioning the cannula, the target flow and oxygenation were successfully achieved. When sufficient venous flow is not achieved, as in our case, clinicians should be alerted so they can identify the cannula tip location on lateral chest radiograph and confirm whether malposition in the azygos vein is the cause of the ineffective ECMO.
Right-sided congenital diaphragmatic hernia (CDH) is less prevalent than left-sided CDH, but more cases require extracorporeal membrane oxygenation (ECMO) application.[1,2] Upon applying ECMO, optimal positioning of the cannula is crucial. There have been few case reports concerning cannulation of the azygos vein in neonates with right-sided CDH.[3] We present a case of azygos vein cannulation in a neonate with right-sided CDH that was confirmed by lateral chest radiograph.
Case Report
A male neonate with a gestational age of 37+3 weeks and birth weight of 3,000 grams was delivered via cesarean section. Right-sided CDH had been diagnosed on antenatal ultrasound. 1-minute and 5-minute Apgar scores were 5 and 6, respectively. The infant was intubated immediately after birth and transported to the neonatal intensive care unit (NICU) for high frequency ventilation. On the chest radiograph, bowel gas was observed on the right lung field, with the heart and mediastinum deviated to the left lung field (Fig. 1). The arterial blood gas analysis on NICU admission was as follows: pH: 6.94, pCO2 > 115 mmHg, pO2: 34 mmHg, HCO3: 26 mmEq/L and lactate: 3.0 mmol/L. Despite application of high frequency oscillatory ventilation and inhaled nitric oxide, hypoxemia and hypercarbia worsened. Initiation of veno-arterial ECMO support was decided, and the neonate was transferred to the pediatric intensive care unit (PICU) for ECMO application at 10 hours after birth.

Antero-posterior chest radiograph after admission. Typical findings of right-sided CDH is noticed – bowel gas is present on the right lung field, and the heart and mediastinum are deviated to the left. CDH: congenital diaphragmatic hernia.
An 8-French arterial and a 12-French venous cannula (DLP, Medtronic, Minneapolis, MN, USA) were placed into the right carotid artery and right internal jugular vein by an experienced cardiac surgical team. However, even after repeated manipulation of the venous cannula and volume expansion through intravenous fluid boluses, negative venous pressure was aggravated, leading to failure to achieve an adequate flow of 100 mL/kg/min and fluctuation of SaO2 from 80-100%. Chest radiographs were taken to confirm the venous cannula location, and although the cannula seemed to be appropriately placed on antero-posterior view (Fig. 2), the cannula tip could not be visualized on echocardiograph. Inappropriate ECMO flow and suboptimal oxygenation continued; thus lateral chest radiograph was taken. The cannula tip was identified posterior to the cardiac silhouette on lateral view which implied cannulation into the azygos vein (Fig. 3A). Therefore the cardiac surgical team partially removed and reinserted the cannula, thereby adjusting it to be placed anteriorly to the heart, which was confirmed by subsequent lateral chest radiograph (Fig. 3B). After the adjustment, the ECMO flow reached 100 mL/kg/min and effective oxygenation was achieved.

Antero-posterior chest radiograph after ECMO cannulation. Total lung haziness is noticed due to ARDS and combined heart failure, thereby obliterating the cardiac silhouette. ECMO: extracorporeal membrane oxygenation; ARDS: acute respiratory distress syndrome; VC: venous cannula; AC: arterial cannula.
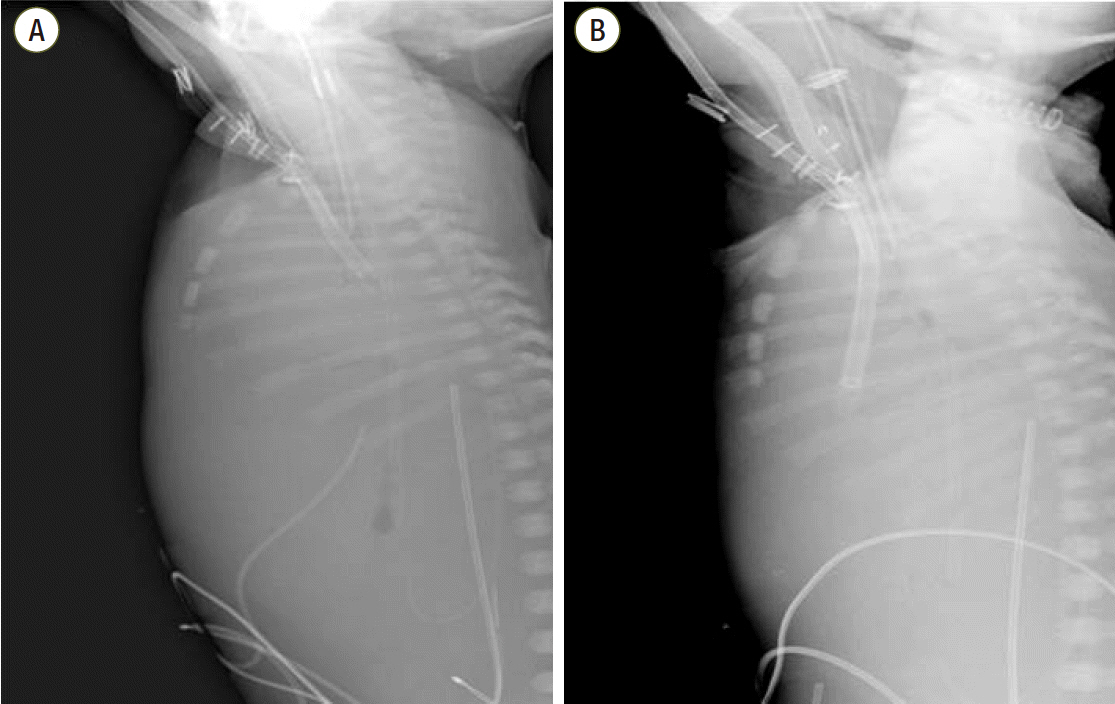
Cross-table lateral chest radiographs showing the cannula tip positioned posterior to the cardiac silhouette (A), and anterior in the superior vena cava after adjustment (B).
The infant underwent CDH repair operation on hospital day 4, was weaned from ECMO without cannula change and ventilator on hospital day 42 and 65, respectively. However, on hospital day 87, sepsis due to Escherichia coli developed, leading to demise on hospital day 92.
Discussion
We describe a case of inadvertent azygos vein cannulation during ECMO application in a neonate with right-sided CDH. In order to clarify the cause of ineffective ECMO flow, lateral chest radiograph was taken, on which azygos vein cannulation was suspected, hence achieving adequate flow and oxygenation by cannula adjustment.
Fisher et al.[3] mentioned two causes of inadvertent azygos vein cannulation in right-sided CDH neonates: (1) blunting of the caval-azygos junction due to mediastinal shift to the left and (2) compression of the inferior vena cava and dilatation of the azygos vein due to liver herniation. The neonate in our case also presented mediastinal shift along with liver and small bowel herniation. Byrnes et al.[4] also reported a case of accidental azygos vein extracorporeal membrane oxygenation cannulation in a neonate with premature closure of the ductus arteriosus. The inadvertent cannulation was identified by lateral chest radiograph. In a case report by Balmaks et al.,[5] there was no remarkable finding on antero-posterior chest radiograph; nevertheless, cannulation into the azygos vein was confirmed by autopsy of the deceased infant. We did not find anything particular concerning cannula location on anterior chest radiograph, which was overturned by lateral chest radiograph. Our case is consistent with the literature, that cross-table lateral chest radiograph is useful in evaluating appropriate placement of cervical ECMO cannula in infants or children.[6]
Echocardiography is another modality to confirm the cannula placement in pediatric patients who need ECMO support. Use of echocardiography for such purpose is said to decrease morbidity associated with circulatory support. [7] In our unit, echocardiography is the routine modality to identify the location of the cannula tip. However, at times only limited information can be obtained from echocardiography due to defective views, failing to capture a clear view of the cannula tip location. Further, echocardiography may not be available at all times. In such circumstances, lateral chest radiograph would be a useful tool to discover an inadvertent cannulation without delay.
In conclusion, azygos vein cannulation is not encountered often, but when venous drainage is not adequate, the cannula location must be identified either by echocardiography or lateral chest radiograph.
Notes
No potential conflict of interest relevant to this article was reported.