Evaluating the use of the respiratory rate-oxygenation index as a predictor of high-flow nasal cannula oxygen failure in COVID-19
Article information

Abstract
Background
It can be challenging for clinicians to predict which patients with respiratory failure secondary to coronavirus disease 2019 (COVID-19) will fail on high-flow nasal cannula (HFNC) oxygen and require escalation of therapy. This study set out to evaluate the association between the respiratory rate-oxygenation index (ROX) and HFNC failure in such patients and to assess whether ROX trajectory correlates with treatment failure.
Methods
This was a single-centre, retrospective, observational study of patients with COVID-19 requiring HFNC, conducted over a 3-month period. ROX was calculated as "pulse-oximetry oxygen saturation (SpO2) over the fractional inspired oxygen concentration (FiO2)/respiratory rate" for each patient at 2, 4, and 12 hours from starting HFNC. HFNC failure was defined as escalation to continuous positive airway pressure ventilation or invasive mechanical ventilation (IMV). Time-to-event analyses were performed to account for the longitudinal data set and time-dependent variables.
Results
We included 146 patients. Ninety-three (63.7%) experienced HFNC failure, with 53 (36.3%) requiring IMV. Higher ROX values were associated with a lower subhazard of HFNC failure on time-to-HFNC failure analysis (subhazard ratio, 0.29; 95% confidence interval [CI], 0.18–0.46; P<0.001). This remained true after controlling for informative censoring. Median ROX values changed differentially over time, increasing in the HFNC success group (0.06 per hour; 95% CI, 0.05–0.08; P<0.001) but not in the HFNC failure group (0.004 per hour; 95% CI, –0.05 to 0.08; P=0.890).
Conclusions
A higher ROX is associated with a lower risk of HFNC failure. Monitoring ROX trajectory over time may help identify patients at risk of treatment failure. This has potential clinical applications; however, future prospective studies are required.
INTRODUCTION
Since the emergence of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in 2019, healthcare facilities worldwide have experienced a marked increase in the number of patients presenting with de novo acute hypoxemic respiratory failure (AHRF) [1,2]. During the early phase of the coronavirus disease 2019 (COVID-19) pandemic there was a preference for early endotracheal intubation and invasive mechanical ventilation (IMV) [3]; however, over time there has been increased use of non-invasive oxygenation strategies [4,5].
High-flow nasal cannula (HFNC) is an oxygen delivery system that has been widely used in the management of AHRF in the pre-COVID-19 era. It is associated with improved respiratory physiology and reduced need for IMV [6,7]. The effectiveness of HFNC in COVID-19 has been demonstrated in multiple studies [8-11]; however, previous data caution that use of HFNC may delay inevitable intubations, resulting in overall worse patient outcomes [12]. Early identification of patients with COVID-19 who are not improving on HFNC remains a challenge for clinicians.
The respiratory rate-oxygenation index (ROX) was developed and validated by Roca et al. [13] in patients with community-acquired or hospital-acquired pneumonia. It uses a simplified oxygenation index (pulse-oximetry oxygen saturation [SpO2] over the fractional inspired oxygen concentration [FiO2]) divided by the respiratory rate to predict HFNC failure and the need for IMV [13,14].
Several authors have evaluated the use of ROX in patients with AHRF secondary to COVID-19, but the findings have been extremely variable [11,15-23], likely due to significant differences in study settings and patient populations. A single meta-analysis found that ROX was effective at predicting HFNC failure, however significant unexplained heterogeneity was observed [24]. The current literature is also limited by the statistical methods used. Most studies to date have utilised area under the curve analyses to identify a cut-off ROX value at a chosen time point that best predicts HFNC failure or success [16-20,23,25,26]. This approach, however, may be misleading, as the included patient population changes over time due to failure or censoring. Additionally, a snapshot ROX value gives no indication of overall trajectory, which itself is informative and affects decision-making.
We conducted a retrospective observational study to evaluate ROX in patients with AHRF secondary to COVID-19 pneumonitis whilst addressing the above issues. The primary aim was to identify whether a lower ROX was associated with a higher hazard of HFNC failure. The secondary aim was to evaluate whether the trajectory of ROX was associated with HFNC failure.
MATERIALS AND METHODS
Study Design and Setting
This was a retrospective cohort study of patients with AHRF secondary to COVID-19 who were treated with HFNC at a major tertiary referral centre in the United Kingdom, over a 3-month period during the delta variant wave of the pandemic (December 2020 to March 2021). Institutional Review Board assessment (21/03/2021 KCC21032021ETU) waived the need for ethics committee review and informed patient consent, as this study used solely anonymised and routinely measured data.
At our institution, HFNC can be initiated and managed in a critical care unit containing level 2 and level 3 beds, in the emergency department or on any ward. Use of HFNC outside of a critical care unit is overseen by the critical care outreach team, a team of senior critical care doctors and nurses operating 24 hours a day, 7 days a week.
Population
All consecutive patients treated at our centre during the study period were screened for inclusion. We included patients who met all of the following criteria: age above 18 years, COVID-19 infection, diagnosis of AHRF, and use of HFNC for more than 2 hours consecutively. COVID-19 infection was defined as reverse transcription polymerase chain reaction nasopharyngeal swab positivity for SARS-CoV-2 on admission or during admission. Patients with both community- and nosocomially acquired COVID-19 infections were included. AHRF was defined as an SpO2 to FiO2 ratio (S/F ratio) of <235. Previous studies in acute respiratory distress syndrome provide evidence that S/F ratio correlates with ratio of arterial oxygen partial pressure (PaO2) to FiO2 (P/F ratio), with a quoted S/F ratio of 235–285 corresponding to a P/F ratio of 26.7 kPa (200 mm Hg) [27,28].
We excluded patients who received less than 2 hours of HFNC, used HFNC as a resting modality between sessions of non-invasive continuous positive airway pressure (CPAP) ventilation, received HFNC immediately on extubation after a period of IMV or had a treatment escalation plan (TEP) instituted prior to HFNC initiation that precluded escalation to CPAP or to IMV (TEP level 1). IMV was defined as endotracheal intubation and mechanical positive pressure ventilation. All patients received COVID-19 treatments as guided by local protocols and multi-disciplinary team decisions. This included the co-administration of medications such as dexamethasone, other steroids, remdesivir, and tocilizumab.
Equipment
The HFNC system used was the Fisher and Paykel Optiflow circuit, which makes use of an MR850 respiratory humidifier with an MR290 chamber, RT241 heated delivery tubing, and an RT033 or RT044 small- or wide-bore nasal cannula (Fisher and Paykel Healthcare). The initial flow was set to 60 L/min unless a patient was unable to tolerate this, and initial FiO2 was titrated to a target SpO2 ≥92%.
Data Collection
Patient demographics were recorded along with comorbidities broadly divided into four main clinically relevant categories. At the point of HFNC initiation vital signs, laboratory data, and baseline severity scores (Sequential Organ Failure Assessment [SOFA] scores and 4C mortality scores [29]) were noted.
We calculated ROX at 2, 4, and 12 hours after starting HFNC using the formula (SpO2/FiO2)/respiratory rate. Our outcome was HFNC failure, initially defined as one or more of the following: escalation to CPAP, escalation to IMV, or death due to respiratory failure prior to CPAP or IMV. The decision to escalate to CPAP or IMV was at the discretion of the treating critical care clinician, with local protocols available for guidance. TEP level 1 (not for CPAP or IMV) established after starting HFNC or death due to other reasons were treated as competing risks. Outcomes were recorded at two, four, 12, 24, 48, and 96 hours after HFNC initiation.
As a sensitivity analysis, the whole analysis was repeated with a narrower definition of HFNC failure, which included only IMV or death due to respiratory failure prior to IMV. This was done to exclude the possibility that the results were predominantly driven by progression to CPAP, which is a significantly clinician dependent decision. TEP level 1 or level 2 (for CPAP but not for IMV) or death due to any other reason were treated as competing risks.
Statistical Analysis
Descriptive analyses are presented as median (interquartile range [IQR]) or number (%). For the primary aim, we confirmed the proportional hazards assumption and conducted a semi-parametric Fine and Gray time-to-event analysis [30] for HFNC failure, treating ROX as a time-varying covariate and accounting for competing risks. The association between ROX and HFNC failure was quantified by calculating adjusted subhazard ratios (SHR) with 95% confidence intervals (95% CI) and the association was visualised using cumulative incidence function curves.
For the secondary aim, we initially used multilevel mixed-effects linear regression to model the trajectory of ROX values over time. We subsequently used joint modelling of longitudinal and time-to-event data in order to incorporate ROX trajectory with time-to-HFNC failure while accounting for ROX measurement error and informative censoring [31]. This model combines linear mixed effects modelling of ROX with a parametric model for time-to-HFNC failure analysis and has been used previously in joint modelling of biomarker levels and the time to an event [32].
Covariate inclusion, selection of a functional form, and model selection followed a structured approach based on likelihood ratio tests and the Akaike Information Criterion. Statistical tests were 2-sided, with an α-level of 0.05 for statistical significance. We did not impute any missing data. Analyses were performed using Stata/MP ver. 17 (StataCorp.). Details regarding the statistical approach are provided in the Appendix.
RESULTS
During the study period, 176 patients with COVID-19 were identified as having received HFNC. Of those, 146 met the inclusion criteria and formed our patient cohort (Figure 1). Ninety-three patients (63.7%) met the outcome of failing on HFNC. Demographics are shown in Table 1. Baseline clinical variables, laboratory data and severity scores are shown in Table 2, along with the COVID-19 treatments each group received. Patients in the HFNC failure group had a lower S/F ratio before starting HFNC compared to those in the HFNC success group (97.89 [IQR, 94.74–101.05] vs. 100.00 [IQR, 96.84–146.67], P=0.001) and had a lower baseline median ROX. SOFA scores were comparable between groups, but patients in the HFNC failure group had a higher median 4C mortality score (11 [IQR, 9–13] vs. 9 [IQR, 7–11], P=0.01). Most of the cohort started HFNC either in the emergency department or on the ward. Only four patients had their treatment initiated in a critical care unit; three were in the HFNC failure group, and one was in the HFNC success group.
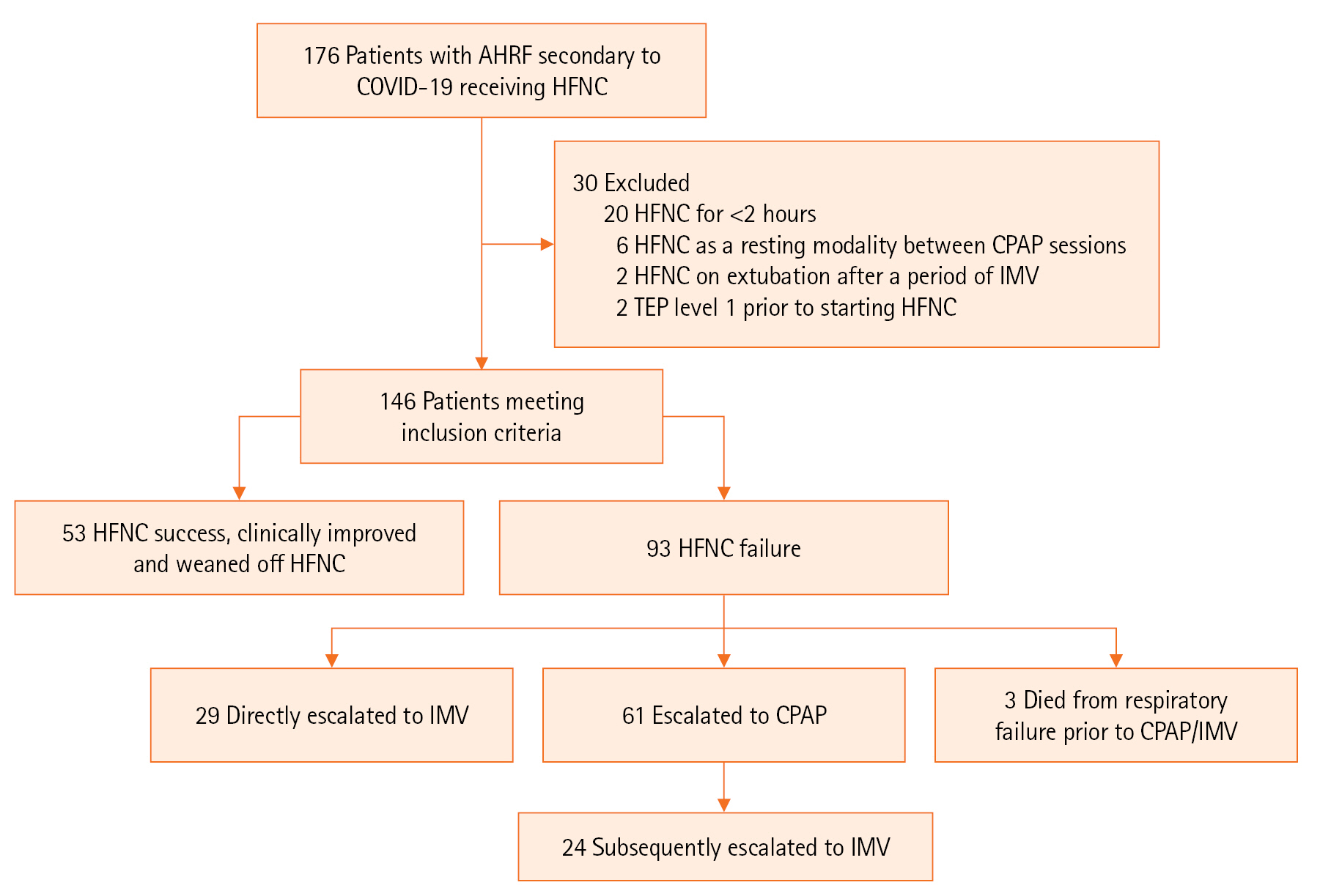
Flowchart of the study cohort. AHRF: acute hypoxemic respiratory failure; COVID-19: coronavirus disease 2019; HFNC: high-flow nasal cannula; CRAP: continuous positive airway pressure; IMV: invasive mechanical ventilation; TEP: treatment escalation plan.

Baseline characteristics of the included patients

Baseline clinical variables, laboratory data, severity scores, and treatments administered
Table 3 shows patient variables and outcomes after starting HFNC. Of the 93 patients who failed HFNC, 61 (65.6%) were escalated to CPAP and 53 (57.0%) underwent IMV, with 24 (25.8%) escalating in a stepwise manner first to CPAP and then to IMV. The total mortality for the cohort was 43 patients (29.5%). Seven patients were in the HFNC success group, and the remaining 36 were in the HFNC failure group (P=0.001). Patients who suffered HFNC failure had consistently lower ROX at all time points compared to those in the HFNC success group. ROX appeared to improve over time in the HFNC success group but remained relatively static in the failure group. The median time spent only on HFNC was significantly shorter in the HFNC failure group compared to the HFNC success group, suggestive of differential or informative censoring (15.58 hours [IQR, 7.53–38.07] vs. 115.28 [IQR, 68.20–156.73], P<0.001).
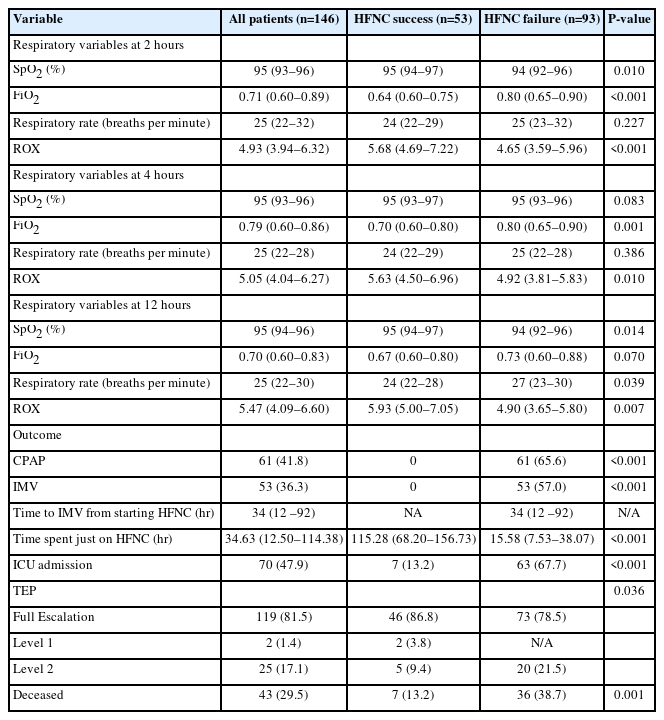
Response to HFNC therapy
In the competing risks, semiparametric time-to-HFNC failure analysis, higher ROX values were associated with a lower subhazard of HFNC failure (SHR, 0.29; 95% CI, 0.18–0.46; P<0.001). No other included covariates were independently associated with a lower subhazard for HFNC failure (Figure 2). The cumulative incidence function curve for three different indicative ROX values is shown in Figure 3. This demonstrates that a higher ROX at any time point was associated with fewer episodes of HFNC failure. The conclusions were unchanged when a narrower outcome definition (IMV or death due to respiratory failure) was used, and the results of the sensitivity analysis are presented in the Supplementary Figures 1 and 2.
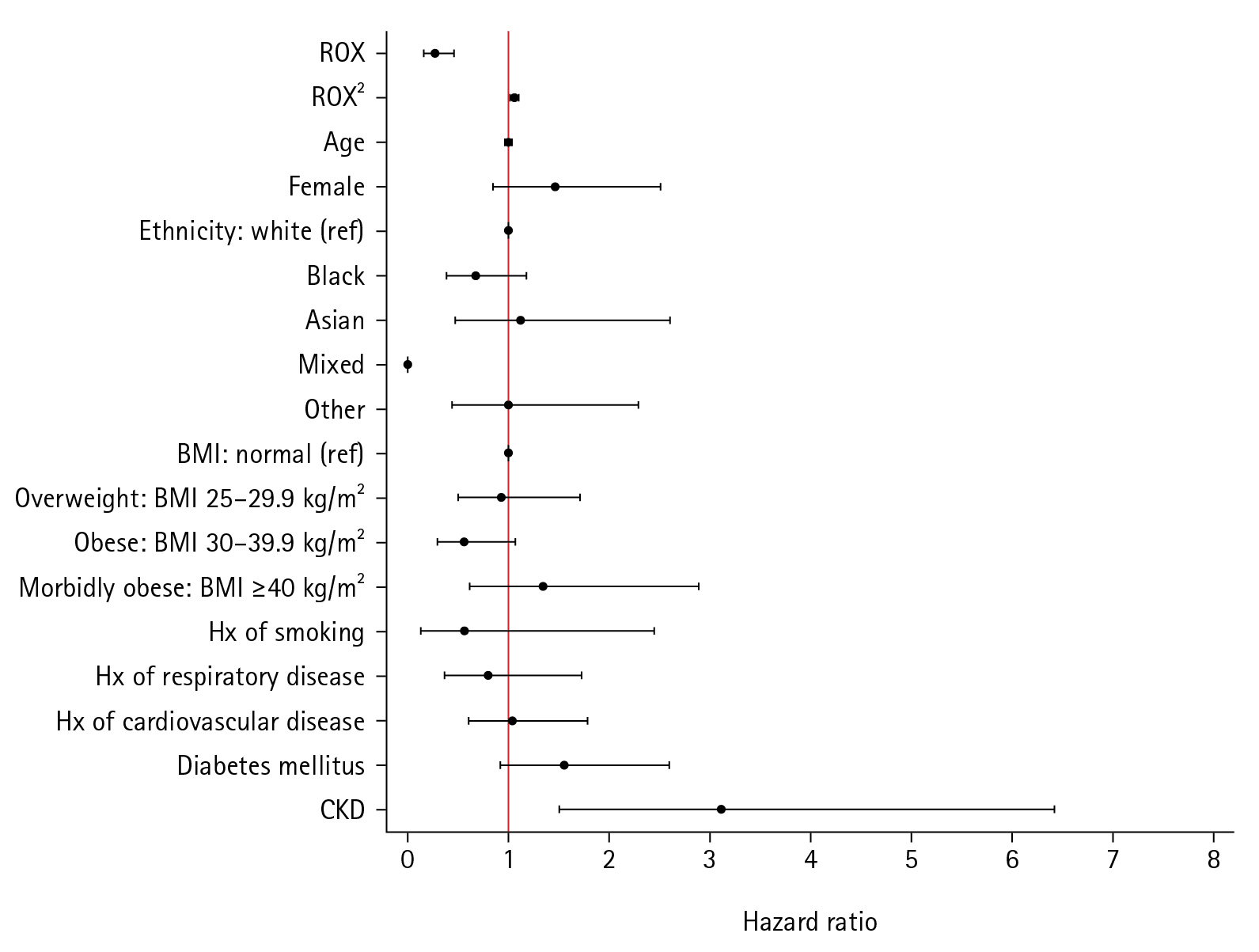
Coefficient plot for competing risks semiparametric time-to-high-flow nasal cannula failure analysis. ROX: respiratory rate-oxygenation index; ref: reference; BMI: body mass index; Hx: history; CKD: chronic kidney disease.

Cumulative incidence function curve for competing risks semiparametric time-to-high-flow nasal cannula (HFNC) failure analysis. ROX: respiratory rate-oxygenation index.
In initial exploratory trajectory analyses (Supplementary Figures 3 and 4), we confirmed that ROX indeed changed over time and led to differential censoring between the two groups. In the mixed-effects linear model, median ROX values increased over time in the HFNC success group (0.06 per hour; 95% CI, 0.05–0.08; P<0.001) but not in the group with HFNC failure (0.004 per hour; 95% CI, –0.05 to 0.08; P=0.890) (Figure 4). This finding was unchanged in the sensitivity analysis (Supplementary Figure 5).
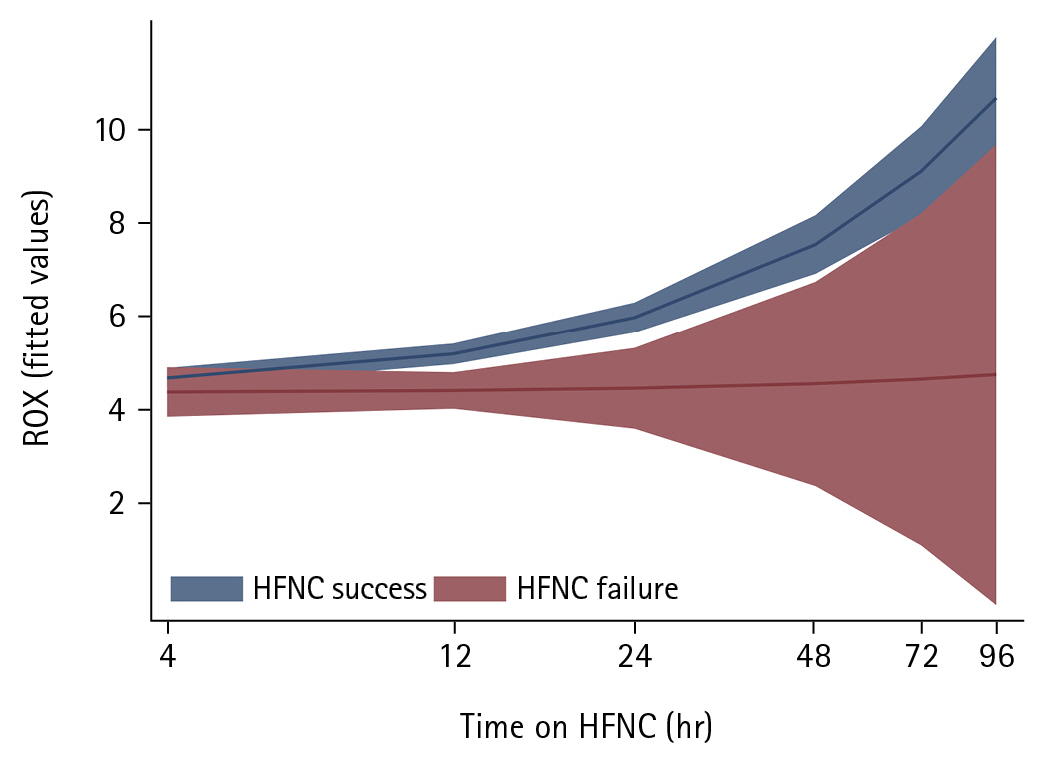
Modelled change over time of respiratory rate-oxygenation index (ROX) values in patients with and without high-flow nasal cannula (HFNC) failure.
In joint modelling of ROX and time-to-HFNC failure, which accounted for informative censoring, ROX increased over time (0.09 per hour; 95% CI, 0.06–0.11), and higher values were again associated with a lower hazard for HFNC failure (HR, 0.33; 95% CI, 0.20–0.54; P<0.001). Further information regarding the association between serial ROX values and HFNC failure is presented in Supplementary Table 1).
DISCUSSION
This study provides a novel analysis of the association between ROX and HFNC failure in patients with AHRF secondary to COVID-19. In our cohort of 146 patients, we demonstrated that a higher ROX is associated with a significantly lower risk of HFNC failure at any time point and that ROX trajectory is informative.
A large proportion of our patients (63.0%) met the outcome and required escalation of ventilatory support. This figure is higher than in other studies [15,20] but is likely attributable to our broad definition of HFNC failure, which included escalation to CPAP. Our observation that 36.3% of our total cohort required IMV is comparable to the 39.7% [17] and 31.7% [22] intubation rates seen in two North American multicentre studies of 272 [17] and 1,847 [22] patients with COVID-19 receiving HFNC. While some authors claim that HFNC is non-inferior to non-invasive ventilation [33], we considered moving to CPAP as HFNC failure since this implies that the treating clinician felt the patient was deteriorating and required another oxygenation strategy. The mortality observed in our study (29.5%) mirrors the 27.7% seen in the large retrospective analysis of 1,847 patients by Myers et al. [22].
Our finding that a higher ROX is associated with a lower risk of HFNC failure is in accordance with existing published data [16,17,21,24]. Previous studies have sought to identify a single ROX cut-off value at a certain time point that predicts HFNC failure or success. This has commonly been attempted by sequentially calculating ROX for patients in a cohort at serial time points [16-20,23,25,26] and then applying area under the curve analyses to identify the ROX value giving maximal sensitivity and specificity for the outcome. There is, however, no consensus on either this specific ROX value or the optimal time point. Furthermore, this method overlooks several important concepts. Firstly, it neither accounts for the interdependence resulting from consecutive measurements in the same patients, nor does it address the longitudinal nature of the generated data. Secondly, the impact of time on both ROX and the outcome is largely ignored. As we have shown, ROX is a time-dependent variable; its effect on the outcome changes over time. Although HFNC failure itself is intrinsically important, the time to this event is also relevant and should be analysed, as this influences clinical decision-making and exposes patients to competing risks. The strategy of repeatedly calculating ROX at set time intervals also leads to the comparison of slightly different patient populations over time. This is due to the continuous stream of patients experiencing the outcome of HFNC failure, experiencing a competing event, or censoring. Censoring due to clinical improvement and cessation of HFNC must also be recognised as informative, as this corresponds to the select cohort of patients with higher and improving ROX. A major strength of our study lies in the acknowledgment of all of these issues, which we have addressed by using appropriate statistical methods, including time-to-event and joint modelling analyses, to control for competing risks and informative censoring. After taking these into account, higher ROX was still associated with less risk of HFNC failure.
Our results interestingly found that ROX changed differentially over time, with the HFNC success group demonstrating an increase in median ROX by 0.06 per hour, whereas minimal change in ROX was observed in the HFNC failure group. This may have important clinical implications. Rather than using a single ROX value at a specific time point to predict HFNC success or failure, as is suggested by the current literature [11,15,17,20-24], we provide evidence that the trajectory of ROX may be used to identify the patients at risk of needing advanced respiratory support. As ROX can be easily calculated at the bedside or incorporated into electronic records [22], serial measurements can be readily performed to track trends. This can highlight patients with relatively static sequential ROX values who may be at risk of HFNC failure. Using ROX in this manner is far more in line with clinical practice, where serial review of an acutely unwell patient can provide insight into their disease course. It should be noted, however, that as the increment in ROX per hour seen in the HFNC success group was small, sufficient time on HFNC would be required to allow for a pattern in ROX to be observed. This preselects a patient population that is not rapidly deteriorating but may be more borderline or have greater physiological reserve. It is in such a group wherein a decision aid can prove most useful.
There are several limitations to this study. Most notably, the retrospective nature inherently risks introducing selection bias. Despite the existence of institutional guidance, both the selection of patients for HFNC and the decision to escalate from HFNC to CPAP or IMV were ultimately at the discretion of the treating critical care clinician. It is therefore possible that both processes could have been affected by retrospectively unidentifiable factors. Due to high rates of HFNC failure, ROX recording was limited to 12 hours, however we recognise that more time points could have further improved the accuracy of our predictions. Our centre has the ability to provide HFNC on any ward, as well as in a critical care unit. In our study, the majority of patients had HFNC initiated in the emergency department or on the ward due to the high number of intubated patients occupying critical care beds during the study period. Although the overall physiologic principles are extrapolatable, we did not perform subgroup analyses, and it is possible that the outcomes may vary depending on the treatment setting. As a result, our conclusions may not be generalisable to institutions using HFNC exclusively in specially designed units or in critical care areas.
Despite an overall increased global consensus in managing COVID-19, it remains a challenge for clinicians to predict which patients will fail on HFNC. We have demonstrated that a higher ROX at any time point is associated with a lower risk of HFNC failure and that monitoring ROX trajectory over time may highlight patients at a higher risk of failure. With an ongoing high number of COVID-19 cases globally there is a need for future prospective studies to investigate ROX trajectory further, as this may have significant clinical application in preventing delays in the escalation of respiratory support. There is also scope to include the non-COVID-19 population in any future work, in order to explore the impact of ROX trajectory in patients with AHRF of any cause.
HIGHLIGHTS
▪ A higher respiratory rate-oxygenation index (ROX) is associated with a lower risk of high-flow nasal cannula (HFNC) oxygen and require escalation of therapy.
▪ Patients with a static ROX over time may be at higher risk of HFNC failure.
▪ The use of ROX may have a clinical application in preventing delays in the escalation of respiratory therapy in patients with coronavirus disease 2019 (COVID-19).
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualisation: SW, SV, VM. Data curation: SW, AB, NBJ, LM, ARB. Formal analysis: SV. Writing–original draft: SW, SV, VM. Writing–review & editing: SW, SV, VM. Writing–final revision and approval of manuscript: all authors.
Acknowledgements
We thank Heira Lansangan for her assistance with data collection. We also thank all King’s College Hospital staff for their care of the patients involved in this study.
SUPPLEMENTARY MATERIALS
Supplementary materials can be found via https://doi.org/10.4266/acc.2022.01081.
Coefficient plot (sensitivity analysis). Respiratory-rate oxygenation index (ROX) remains associated with a lower subhazard for high-flow nasal cannula oxygen (HFNC) failure. Each variable point estimate is slightly different to the original analysis. BMI: body mass index; Hx: history of; CKD: chronic kidney disease.
acc-2022-01081-Supplementary-Figure-1.pdfCumulative incidence function curve (sensitivity analysis). Comparison of regular time-to event analysis vs. Fine-Gray analysis. In the regular time-to-event analysis (without competing risks) the subhazard ratio for respiratory-rate oxygenation index (ROX) was 0.18 (95% confidence interval,0.12–0.27; P<0.001) which is an overestimation, given the results of the Fine-Gray analysis.
acc-2022-01081-Supplementary-Figure-2.pdfExploratory trajectory plot of respiratory-rate oxygenation index (ROX) values in patients with and without high-flow nasal cannula oxygen (HFNC) failure.
acc-2022-01081-Supplementary-Figure-3.pdfExploratory trajectory plot of respiratory-rate oxygenation index (ROX) values in patients with and without high-flow nasal cannula oxygen (HFNC) failure (sensitivity analysis).
acc-2022-01081-Supplementary-Figure-4.pdfModelled change over time of respiratory-rate oxygenation index (ROX) values in patients with and without high-flow nasal cannula oxygen (HFNC) failure (sensitivity analysis).
acc-2022-01081-Supplementary-Figure-5.pdfResults from the primary and sensitivity analysis of joint longitudinal and survival outcomes for the association between serial ROX values and HFNC failure
acc-2022-01081-Supplementary-Table-1.pdf