Risk factors for hospital mortality in intensive care unit survivors: a retrospective cohort study
Article information

Abstract
Background
Deaths can occur after a patient has survived treatment for a serious illness in an intensive care unit (ICU). Mortality rates after leaving the ICU can be considered indicators of health care quality. This study aims to describe risk factors and mortality of surviving patients discharged from an ICU in a university hospital.
Methods
Retrospective cohort study carried out from January 2017 to December 2018. Data on age, sex, length of hospital stay, diagnosis on admission to the ICU, hospital discharge outcome, presence of infection, and Simplified Acute Physiology Score (SAPS) III prognostic score were collected. Infected patients were considered as those being treated for an infection on discharge from the ICU. Patients were divided into survivors and non-survivors on leaving the hospital. The association between the studied variables was performed using the logistic regression model.
Results
A total of 1,025 patients who survived hospitalization in the ICU were analyzed, of which 212 (20.7%) died after leaving the ICU. When separating the groups of survivors and non-survivors according to hospital outcome, the median age was higher among non-survivors. Longer hospital stays and higher SAPS III values were observed among non-survivors. In the logistic regression, the variables age, length of hospital stay, SAPS III, presence of infection, and readmission to the ICU were associated with hospital mortality.
Conclusions
Infection on ICU discharge, ICU readmission, age, length of hospital stay, and SAPS III score increased risk of death in ICU survivors.
INTRODUCTION
Despite advances in the quality of health care, deaths can occur after a patient has survived treatment for a serious illness in an intensive care unit (ICU). Post-ICU mortality rates described in the literature can range from 5% to 27% [1-5]. Mortality rates after leaving the ICU can be considered indicators of health care quality. Several factors have been described associated with death in the short-term after ICU discharge. Most of these risk factors are associated with age, disease severity, and length of stay in the ICU, in addition to infections and the need for unplanned readmissions [6-8]. Health care-associated infections (HAIs) are worrisome complications during an intensive care stay and may be associated with increased mortality in ICU survivors [7,9]. Another risk factor that is associated with mortality after an intensive care stay is readmission to the ICU, which can increase intra-hospital mortality by ten times [8]. It is estimated that for every 100 patients discharged from the ICU, 4 to 6 will be readmitted to this sector, noting that between 3 and 7 of these patients will die before hospital discharge, thus demonstrating the high risk in this transition of care [10]. It is estimated that the hospital mortality rate for patients who require readmission to the ICU is 34.3% [9].
Decisions to discharge patients from the ICU should take into consideraticon possible risk factors for hospital mortality present at that moment, to allow safer transition of care. Prognostic scores are widely used, and these tools can contribute as an indicator of the performance of care provided by the units and hospitals through severity-adjusted mortality rates. A prognostic score that is widely used and with good performance is the Simplified Acute Physiology Score (SAPS) III, which corresponds to the clinical analysis of the patient on admission, and is scored according to demographic, clinical, and physiological variables [11,12]. The current study aims to describe the hospital mortality rate and assess risk factors for death in surviving patients discharged from an ICU at a university hospital.
MATERIALS AND METHODS
Research Ethics
This study was performed according to the Helsinki Declaration and approved by the local Research Ethics Committee (CAAE 85685418.7.0000.5231; Opinion 2,568,527) of the institution where the experiment was performed. Written informed consent was waived.
A retrospective cohort study, carried out with adult surviving patients admitted to a mixed clinical-surgical ICU of a University Hospital from January 2017 to December 2018. When a patient was readmitted, only the discharge from the ICU on the first admission was used for data collection and the patient was followed up until the hospital outcome. Patients under 18 years of age or those with incomplete medical records were excluded. This is a 20 bed ICU that provides care for adult patients in a University Hospital with 300 beds. The ICU's occupancy rate was above 95% for entire the study period. All patients who leave the ICU are transferred to the same level of care in the hospital wards. There is no intermediate care facility in the institution. There is a 24-hour rapid response team on duty lead by an intensivist.
Information was collected on age, sex, length of hospital stay, diagnosis in patients with ICU survivor, readmission to the ICU, hospital discharge outcome, presence of infection, microorganisms isolated, and the SAPS III in patients with ICU survivor. The main outcome of the study was death or discharge from the hospital.
An infected patient was defined as those who were being treated with antimicrobials agents for an infection diagnosis on discharge from the ICU. Treatment for infections were revised by an infectologist according to the stewardship program to ensure adequate treatment. Infected patients were divided according to the identification of the etiological agent into unidentified microorganisms, sensitive microorganisms, multidrug-resistant microorganisms (MDR), extensively drug-resistant (XDR), and pandrug-resistant microorganisms (PDR). The definitions of antimicrobial resistance followed the recommendations of the task force of the European Centre for Diseases Prevention and Control and Centers for Disease Control and Prevention, as follows: MDR was defined as acquired non-susceptibility to at least one agent in three or more antimicrobial categories, XDR was defined as non-susceptibility to at least one agent in all but two or fewer antimicrobial categories (i.e. bacterial isolates remain susceptible to only one or two categories) and PDR was defined as non-susceptibility to all agents in all antimicrobial categories [13]. Readmission to the ICU was considered if there was a new unscheduled admission after discharge from the ICU in the same hospital stay.
Statistical Analysis
After applying the Shapiro-Wilk test, continuous variables were summarized as median and interquartile range (IQR) for not assuming normality. Categorical variables are reported as absolute and relative frequencies and their 95% confidence intervals (CIs), expressed in tables and figures. For comparisons of groups, the Mann-Whitney test or chi-square test was used. The association between the studied variables was performed by the logistic regression model and presented as odds ratio (OR) and 95% CI. Additionally, Kaplan-Meier analysis was performed to estimate the probability of survival after ICU discharge at various time intervals. Significant differences were established by P<0.05. IBM ver. 21 software (IBM Corp.) was used for analysis.
RESULTS
During the study period, 1,596 patients were admitted to the ICU and of these, 537 patients died in this unit. Of the 1,059 surviving ICU patients, 33 were excluded for incomplete data and 1 for being under 18 years of age (Figure 1). Data were collected from 1,025 medical records. The median age was 62 years (IQR, 46.0–73.5 years), with a predominance of males, 573 (55.9%). The length of hospital stay of these patients had a median of 17 days (IQR, 8–30 days) and the SAPS III severity score presented a median of 47 (IQR, 35.0–62.5).
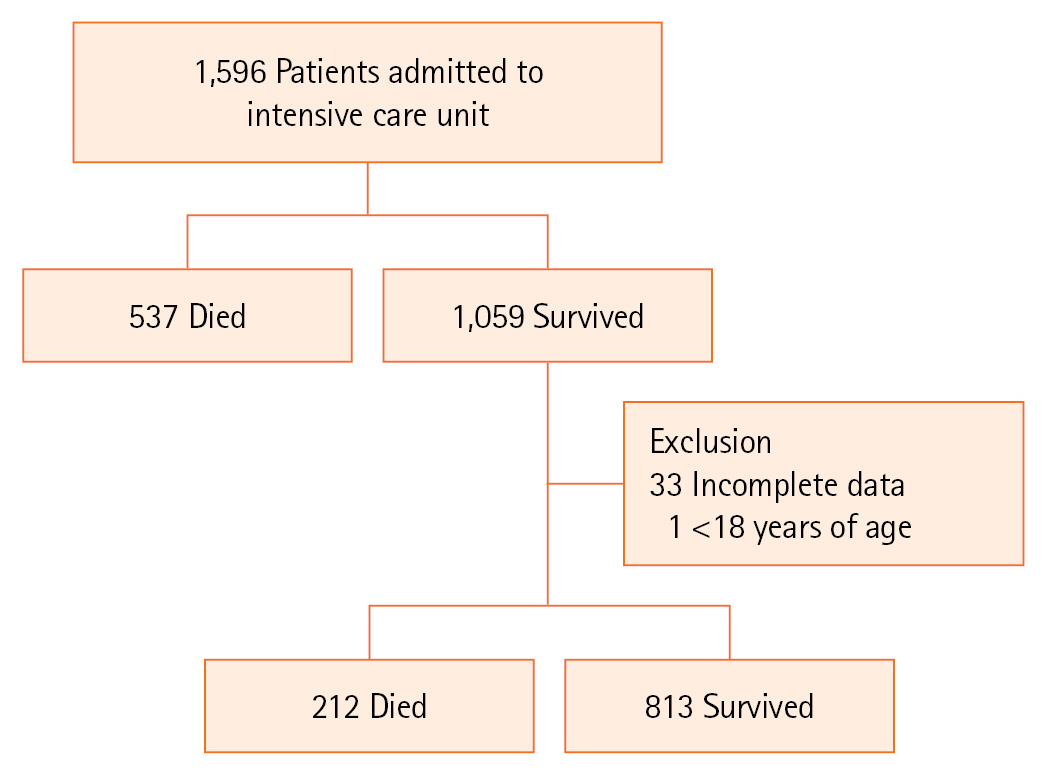
Flowchart of patients.
Of the total number of patients studied, 314 (30.6%) had some type of infection at ICU discharge, 92 (9%) were readmitted to the unit, and 212 (20.7%) died. Considering the patients who developed some type of infection, in 103 (32.8%) it was not possible to identify the microorganism, 78 (24.8%) were sensitive microorganisms, 81 (25.8%) were XDR, 50 (15, 9%) MDR, and 2 (0.6%) PDR. The most frequently found infectious foci were pulmonary, with 253 cases (77%), followed by the urinary tract with 63 (18.1%) and the surgical site with 24 (6.4%).
There were 588 (57.4%) unplanned ICU admissions and 437 (42.6%) planned admissions in the study period. The most frequent admission diagnoses were 153 lower limb osteosynthesis (14.9%), 128 digestive tract surgeries (12.5%), 84 intracranial hemorrhages (8.20%), 81 sepsis (7.9%), 52 neurosurgeries (5.1%), 44 peripheral vascular surgeries (4.3%) and 44 head traumas (4.3%).
When assessing vital status at hospital discharge, the median age of non-survivors (67.5 years) was higher compared to survivors (60 years, P<0.001). There was no association between sex and hospital mortality (P=0.103). The length of hospital stay and the SAPS III were higher among non-survivors (P<0.001). The presence of infection and readmission to the ICU were associated with hospital death (P<0.001). When analyzing the 212 cases of death, 117 (55.2%) occurred in infected patients; 28 (13.2%) by sensitive microorganisms, 30 (14.2%) by unidentified microorganisms, and 59 (27.8%) by resistant microorganisms (Table 1).
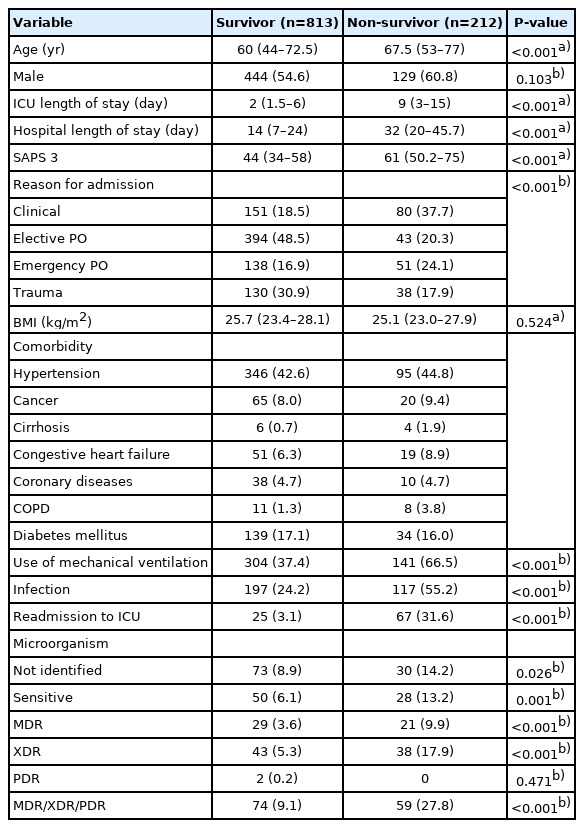
Univariate analysis to describe of intensive care unit survivors according to hospital outcome
In the logistic regression, the vital status on hospital discharge was considered as the dependent variable, and age, length of hospital stay, SAPS III, presence of infection, readmission to the ICU, and microorganisms were considered as covariates. The variables that remained in the regression model were age (OR, 1.029; 95% CI, 1.01–1.04; P<0.001), length of hospital stay (OR, 1.011; 95% CI, 1.003–1.019; P=0.004), SAPS III (OR, 1.042; 95% CI, 1.031–1.054; P<0.001), presence of infection (OR, 1.251; 95% CI, 1.081–1.447; P=0.003), and readmission to the ICU (OR, 11.659; 95% CI, 6.522–20.842; P<0.001) (Table 2). Kaplan-Meier analysis shows a median 49,000 days (95% CI, 42.987–55.013 days) after ICU discharge and 200 death events in 90 days (Figure 2).
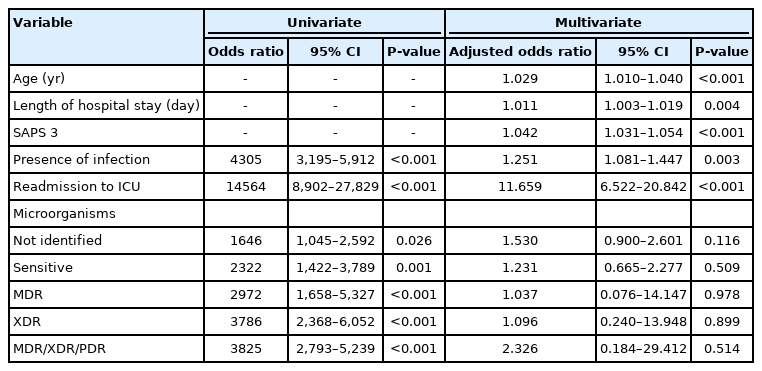
Univariate and multivariate analysis for factors associated with mortality in ICU survivors, from January 2017 to December 2018

Analysis of 90-day survival after intensive care unit discharge of 1,025 patients. Kaplan-Meier analysis shows a median 49,000 days (95% confidence interval, 42.987–55.013) intensive care unit discharge and 200 death events in 90 days.
DISCUSSION
The present study describes factors associated with hospital mortality in ICU survivors. The presence of infection on discharge from the ICU and readmissions demonstrated the greatest weight for the risk of death for these patients. These results can support decisions on optimizing HAI prevention and treatment, in addition to the allocation of resources and the prioritization of patients at a higher risk for intermediate care units after leaving the ICU [14,15].
Previous studies have shown that several factors may be associated with worse outcomes after ICU discharge. The intensity of therapeutic interventions and nursing overload at ICU discharge were associated with an increase in hospital mortality [3]. A systematic review described a readmission score that predicts adverse events after ICU discharge. The Minimizing ICU Readmission score takes into account several factors for this prediction, such as the SAPS II prognostic score at ICU admission, the use of a central venous catheter during the ICU stay, the SOFA score at ICU discharge, the presence of SIRS in the last 2 days of ICU stay, and discharge from the ICU at night [16].
Although the prognostic scores present moderate performance, with limitations in their calibration in low and middle-income countries, the SAPS III remains the most applied prognostic assessment tool in several countries [17,18]. The SAPS III calculated at ICU discharge could better reflect the risk of hospital death, but it is not common for units to have this data in routine care furthermore, SAPS III was developed to predict hospital mortality, not ICU mortality. In our study, we chose the SAPS III at ICU admission because it is the score available in the data source and because it is adopted by the institutional policy to evaluate the unit's performance and, therefore, can be easily incorporated to identify patients at a high risk of an unfavorable outcome at ICU discharge.
In a recent study of patients affected by coronavirus disease 2019 (COVID-19), age was the factor identified as associated with increased mortality [19], similar to what was found in our sample, where each year of age increased the chance of post-ICU death by approximately 3%. On the other hand, Madotto et al. [20] describe that the presence of comorbidities and limitations of life support treatments resulted in worse outcomes in ICU survivors.
Our post-ICU discharge mortality can be considered high when compared with results from Europe and New Zealand [21,22]. Although the research institution has implemented follow-up of surviving ICU patients by a rapid response team led by an intensive care physician, there is a high demand for ICU beds that pressures early discharge and there is no availability of intermediate care beds. Reports from low- and middle-income countries show similar results [5].
The prevalence of death in infected patients who survived the ICU was high in our study. The increased risk of post ICU mortality in patients with infections has been pointed out by other authors [23-26]. It is estimated that infection by MDR increases hospital mortality by approximately 1.7 times [23,24], which is similar to the results of the current study.
Pneumonia is the most frequent focus of infection reported by other studies [27-29], and this result is consistent with our findings. Klebsiella species was the most commonly isolated microorganism in our patients. This bacterium is related to almost a third of infections caused by Gram-negative bacteria in general, and presents high resistance to antimicrobials [30,31]. Other Gram-negative microorganisms responsible for HAIs are Enterobacteriaceae, Pseudomonas aeruginosa, Acinetobacter baumannii, and Stenotrophomonas maltophilia. The frequency of pneumonia caused by Klebsiella pneumoniae resistant to carbapenems is above 25%, while the frequency for P. aeruginosa is between 20 and 40% and for A. baumannii, between 40% and 70% [32].
Readmission to the ICU is associated with higher mortality and longer hospital stays [33]. Patients surviving readmission should be monitored and, preferably, remain in intermediate care units. The worse prognosis of patients requiring readmission could be associated with decompensation in the ward, which may result in late intervention. The use of intermediate care units can meet the needs of these higher-risk patients who require surveillance [14]. The length of hospital stay, as a risk factor for death, was also demonstrated in the present study, corroborating studies that show that a period longer than 6 days exposes the patient to more infectious risks [34].
It is possible to reduce readmission rates and increase the safety of surviving ICU patients through the implementation of rapid response teams, in view of the follow-up performed by an intensive care physician in the wards of patients discharged from the ICU [35]. It is estimated that implementation of the rapid response team is associated with a 20.6% decrease in the mortality rate [36].
The study population composed exclusively of ICU survivors, in addition to the sample size, can be considered strengths of the present study. Limitations of the study are the fact that it is a retrospective and single-center analysis, which limits its external validity. Also, a limited number of variables were investigated as risk factors for mortality. Other factors that can affect mortality, such as underlying comorbidities, the use of mechanical ventilation, renal replacement treatment or vasoactive drugs were not included in the regression analysis.
In conclusion, a high mortality rate was observed in patients who survived hospitalization in the ICU and the factors associated with hospital mortality were age, SAPS III, presence of infection, readmission to the ICU, and length of hospital stay.
KEY MESSAGES
▪ Infection diagnosis on intensive care unit discharge increases risk of hospital mortality.
▪ Intensive care readmission is a risk factor for hospital death in critical ill survivors from intensive care unit.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualization: LGAS, ELL, CMCG. Data curation: LGAS, CMDMC, TBT, CMCG. Formal analysis: ELL. Methodology: LGAS, CMDMC, TBT, LTQC, CMCG. Project administration: CMCG. Visualization: all authors. Writing–original draft: LGAS, TBT. Writing–review & editing: CMC, LTQC, ELL, CMCG.
Acknowledgements
None.