Analysis of avoidable cardiopulmonary resuscitation incidents with a part-time rapid response system in place
Article information

Abstract
Background:
Although a rapid response system (RRS) can reduce the incidence of cardiopulmonary resuscitation (CPR) in general wards, avoidable CPR cases still occur. This study aimed to investigate the incidence and causes of avoidable CPR.
Methods:
We retrospectively reviewed the medical records of all adult patients who received CPR between April 2013 and March 2016 (35 months) at a tertiary teaching hospital where a part-time RRS was introduced in October 2012. Four experts reviewed all of the CPR cases and determined whether each event was avoidable.
Results:
A total of 192 CPR cases were identified, and the incidence of CPR was 0.190 per 1,000 patient admissions. Of these, 56 (29.2%) were considered potentially avoidable, with the most common cause being doctor error (n=32, 57.1%), followed by delayed do-not-resuscitate (DNR) placement (n=12, 21.4%) and procedural complications (n=5, 8.9%). The percentage of avoidable CPR was significantly lower in the RRS operating time group than in the RRS non-operating time group (20.7% vs. 35.5%; P=0.026). Among 44 avoidable CPR events (excluding cases related to DNR issues), the rapid response team intervened in only three cases (6.8%), and most of the avoidable CPR cases (65.9%) occurred during the non-operating time.
Conclusions:
A significant number of avoidable CPR events occurred with a well-functioning, part-time RRS in place. However, RRS operation does appear to lower the occurrence of avoidable CPR. Thus, it is necessary to extend RRS operation time and modify RRS activation criteria. Moreover, policy and cultural changes are needed prior to implementing a full-time RRS.
INTRODUCTION
Cardiopulmonary arrest is a catastrophic event that is associated with an increased risk of organ failure as well as high levels of morbidity, mortality, and added costs [1-3]. Research has shown that a significant proportion of in-hospital cardiopulmonary arrests (IHCAs) were preventable before the event, as signs of premature aggravation were found [4,5]. Therefore, the rapid response system (RRS) was introduced to identify and stabilize “at-risk” patients at an early stage, prior to arrest [6,7].
The RRS has been reported to reduce the incidence of cardiopulmonary resuscitation (CPR), particularly in general wards [8,9]. However, it does not prevent the occurrence of CPR entirely, as not all CPR cases that occur under RRS monitoring are preventable. A previous U.S. study conducted at a university-affiliated tertiary care hospital with a well-established, full-time RRS, however, reported that 18% of 104 IHCAs were “avoidable” [10]. These cases were sufficiently preventable and should not have occurred. In order for the RRS to become a more effective safety system, specific needs and concerns must be addressed to reduce the occurrence of “avoidable” CPR cases. Our institution has a well-functioning, part-time RRS that was introduced 6 years ago [11]. In this study, we analyzed the incidence and causes of avoidable CPR cases that occurred under a part-time RRS. We will discuss strategies to ensure that safety monitoring systems are ideal.
MATERIALS AND METHODS
Research Ethics
This study was performed in accordance with the amended Declaration of Helsinki. The Institutional Review Board of the Seoul National University Bundang Hospital where the research was performed approved the study protocol (IRB No. B-1611-372-103) and waived the requirement for informed consent due to the retrospective study design.
Patients and Settings
We conducted this retrospective study at a 1,300-bed tertiary care, university-affiliated hospital. The hospital includes a general ward (1,172 beds), intermediate units (62 beds), and five intensive care units (ICUs; medical, surgical, neurosurgical, neonatal, and emergency). We used the RRS registry to identify IHCAs between April 2013 and March 2016 (35 months). Adult patients ( > 18 years of age) who experienced cardiopulmonary arrest in either a general ward or an intermediate unit were included in the study. Events occurring in the ICUs, emergency department, pediatric ward, or operating room were excluded. Four experts (two intensivists and two rapid response team nurses) separately reviewed all CPR cases in a partly blinded manner (the event date and place were blinded), specifically focusing on whether the event was avoidable. A cardiopulmonary arrest was defined as an event in which cardiac compressions were attempted to restore spontaneous circulation, with cessation of spontaneous circulation confirmed or suspected according to any signs or symptoms [12].
Definition of Avoidable CPR
The term “avoidable” was assigned to a case when all four experts agreed that the event was potentially avoidable and was defined if at least one of the following was noted during the 48 hours preceding the event and was considerably related to CPRs [10,13]: (1) delayed ( > 2 hours) or inadequate response from the assigned doctor to abnormal signs or symptoms, (2) procedural complication potentially responsible for the event, (3) delay ( > 20 minutes) by the assigned nurse in calling the doctor, (4) medication-related event (e.g., overdose or inappropriate use of medication), (5) do-not-resuscitate (DNR) issue (i.e., no documented DNR order in place until the event, despite verbal DNR orders or discussions of DNR status with the patient’s family), and (6) other causes closely associated with the event (e.g., other unexpected or unintentional episodes which led to the CPR).
Part-Time RRS Screening and Non-screening Unit
The RRS was introduced in our hospital in October 2012 and has been used on a part-time basis. The system operates between 7 am and 10 pm on weekdays and between 7 am and 12 pm on Saturdays. There are two ways to activate the RRS: via a direct call or via the electronic medical record (EMR) screening system. Our RRS is activated in most cases by the RRS screening system (over 90% of cases), while < 10% of RRS cases are activated via direct calls [14]. The screening system has 10 triggering criteria. If an abnormal value (based on predefined criteria) is recorded in the EMR, this is automatically detected by our screening system, and an alert is transferred to the RRS nurses. Then RRS nurses will attend the patient for a primary check, and if further work-up and specific interventions are required, they notify the RRS physicians [14].
The RRS screens all hospital wards except for intermediate units (non-screening units). An intermediate unit is characterized by nearly continuous monitoring or a level of monitoring comparable to intensive nursing (the nurse-to-patient ratio is 1:4 in an intermediate unit vs. 1:6 in a general ward). This unit is used for patients with severe conditions who require more frequent care and monitoring than patients in the general ward, but who have fewer care and monitoring requirements than patients in the ICU. As patients who are in the intermediate units are already closely monitored, the RRS can only be activated via a direct call in an emergency. Routine RRS screening is not performed on the intermediate units (RRS non-screening units). The detailed characteristics of the RRS are summarized in Supplementary Table 1.
Data Collection
The following data for patients undergoing CPR were obtained from the medical records: demographic information, comorbidities, date on which CPR was performed, return of spontaneous circulation, and hospital survival rates. The Charlson comorbidity index and cardiac arrest risk triage score were calculated, with higher scores indicating a higher possibility of cardiac arrest [15].
Statistical Analysis
Data for continuous and categorical variables are represented as mean ( ± standard deviation) and number (percentage), respectively. Comparisons between groups were conducted using a Student t-test for continuous variables and Pearson’s chi-square test for categorical variables. The linear-by-linear association test was used to test for trends in a table that was larger than two-by-two. The IBM SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA) was used for statistical analyses. The P-values < 0.05 were considered statistically significant.
RESULTS
During the study period (35 months), a total of 192 CPRs (145 in the general ward and 47 in the intermediate unit) were identified (Figure 1). Differences in the characteristics of patients with IHCA during RRS operating times compared to during RRS non-operating times are described in detail in Table 1. There were no significant differences in age (mean, 71 vs. 67 years), Charlson comorbidity index (mean, 3.0 vs. 3.2), cardiac arrest risk triage score (mean, 23.4 vs. 22.4), or IHCA causes between the RRS non-operating time group and the RRS operating time group. Hospital survival rate was significantly higher in the RRS operating time group than in the RRS non-operating time group (32.9% vs. 20.0%, P = 0.042). The percentage of cases classified as avoidable CPR was significantly lower in the RRS operating time group than in the RRS non-operating time group (20.7% vs. 35.5%, P = 0.026).

Distribution of cardiopulmonary resuscitation (CPR) cases according to rapid response system monitoring and operating times.

Baseline characteristics, causes, and outcomes of patients with in-hospital cardiopulmonary arrest
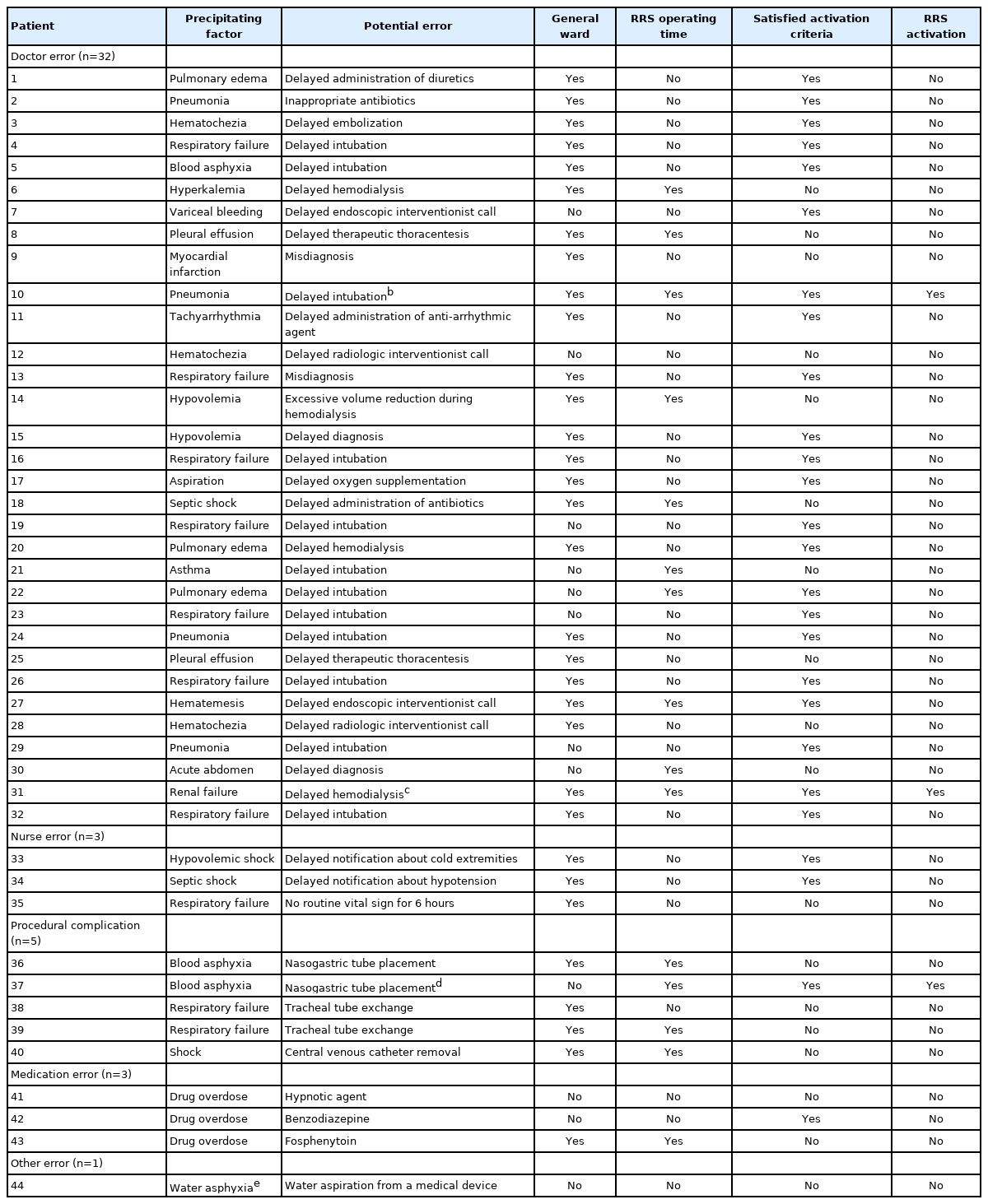
The four experts agreed that CPR was potentially avoidable in 56 cases (29.2%) (Table 2). The most common causes were doctor error (n = 32, 57.1%), followed by a DNR issue (n = 12, 21.4%) and procedural complications (n = 5, 8.9%). However, there was no significant difference in the causes of avoidable CPR between the RRS operating and non-operating times (P = 0.504). Details of precipitating factors for CPR and the associated potential errors are summarized in Table 3. Among the avoidable CPR cases, except for cases with a DNR issue, three cases in which CPR occurred despite prior RRS examination and intervention were identified.

Causes of potentially avoidable CPR cases
DISCUSSION
In the present study, 29.2% (56/192) of CPR cases were considered potentially avoidable, corresponding to an average of 1.6 cases per month. The rate of avoidable CPR cases was significantly lower during RRS operating times than during non-operating times. Although implementation of the RRS did not eliminate all avoidable CPRs, these findings suggest that RRS operation can reduce the rate of avoidable CPR. Among 44 avoidable CPR cases (excluding DNR issue-related cases), only three cases (6.8%) were examined by the RRS team (Table 3). Most of the avoidable CPR cases (65.9%) occurred during the non-operating time. Moreover, only five out of 15 avoidable CPR cases that occurred during the operating time met the RRS activating criteria. These findings indicate the necessity of expanding RRS operation and modifying the RRS activating criteria (e.g., introduction of serum electrolytes, mentality and urine output criteria, and mitigation of SpO2 criteria).
Most avoidable CPR cases were related to doctor error. There was no significant difference in the rate of doctor errors between the RRS operating time and non-operating time. These results imply that avoidable CPRs would not be completely prevented by the full-time RRS since doctor error accounts for a considerable portion. Preventing doctor errors is of utmost importance. Whether or not a doctor makes an error depends on the specific doctor’s medical knowledge and experience; therefore, continuous education for medical personnel is crucial.
Five CPR cases were potentially associated with procedural complications. Cases that involve nasogastric tube placement and tracheostomy tube exchange rarely occur and can be prevented if performed by experienced personnel [16,17]. Most practitioners know that these procedures are relatively simple, easy, and safe; thus, they are often performed carelessly. A rigorous educational program should be introduced to minimize fatal complications by emphasizing the risks involved in simple procedures as well as those associated with more complex techniques.
We identified 12 cases involving DNR issues in which discussions regarding end-of-life care or DNR status between medical personnel and the families of patients were not documented prior to events. These patients eventually died after resuscitation. Resuscitation in terminally ill patients is generally considered unfavorable and futile [18]. The RRS appeared to contribute to the determination of CPR status [19-21]. Active and intensive discussion on admission between medical personnel and the families of patients regarding end-of-life care and CPR status is required for patients in whom resuscitation is likely to be futile.
This study has some potential limitations that should be considered. Because of the retrospective study design, we could not know the exact situation at the time of the CPR event and could only rely on the clinical chart review. However, to minimize bias, we restricted the designation of avoidable CPR to cases where all four experts agreed after independently analyzing the data (while partially blinded, i.e., blinded to the event time and place). Second, since our results are derived from a single tertiary care, university-affiliated hospital, it is unclear if our results are generalizable.
In conclusion, despite the low incidence of IHCA, a significant number of avoidable CPR cases occurred under a well-functioning, part-time RRS. However, RRS operation appears to lower the occurrence of avoidable CPR. Thus, it is necessary to extend the RRS operation time and modify RRS activating criteria to reduce these truly preventable events. Moreover, policy and cultural changes (e.g., proper and continuous education for medical personnel and early identification and placement of the DNR order) should be addressed prior to expanding to full-time RRS.
KEY MESSAGES
▪ We investigated the incidence and causes of avoidable cardiopulmonary resuscitation (CPR) while a part-time rapid response system (RRS) was in place.
▪ A significant number of avoidable CPR events occurred.
▪ It is necessary to extend RRS operation time and modify RRS activation criteria.
Notes
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: JYC, JSP, YJC, HIY, JHL, CTL, YJL. Data curation: all authors. Formal analysis: JYC, DSL, YYC, JSP, YJC, HIY, JHL, CTL. Writing–original draft: JYC. Writing–review & editing: YJL.
SUPPLEMENTARY MATERIALS
Supplementary materials can be found via https://doi.org/10.4266/acc.2020.01095.
Characteristics of the rapid response system