Decision-making regarding withdrawal of life-sustaining treatment and the role of intensivists in the intensive care unit: a single-center study
Article information

Abstract
Background
This study examined the experience of withholding or withdrawing life-sustaining treatment in patients hospitalized in the intensive care units (ICUs) of a tertiary care center. It also considers the role that intensivists play in the decision-making process regarding the withdrawal of life-sustaining treatment.
Methods
We retrospectively analyzed the medical records of 227 patients who decided to withhold or withdraw life-sustaining treatment while hospitalized at Ewha Womans University Medical Center Mokdong between April 9 and December 31, 2018.
Results
The 227 hospitalized patients included in the analysis withheld or withdrew from life-sustaining treatment. The department in which life-sustaining treatment was withheld or withdrawn most frequently was hemato-oncology (26.4%). Among these patients, the most common diagnosis was gastrointestinal tract cancer (29.1%). A majority of patients (64.3%) chose not to receive any life-sustaining treatment. Of the 80 patients in the ICU, intensivists participated in the decision to withhold or withdraw life-sustaining treatment in 34 cases. There were higher proportions of treatment withdrawal and ICU-to-ward transfers among the cases in whom intensivists participated in decision making compared to those cases in whom intensivists did not participate (50.0% vs. 4.3% and 52.9% vs. 19.6%, respectively).
Conclusions
Through their participation in end-of-life discussions, intensivists can help patients’ families to make decisions about withholding or withdrawing life-sustaining treatment and possibly avoiding futile treatments for these patients.
INTRODUCTION
End-of-life care and life-sustaining treatment withholding and withdrawal (LSTW) received little attention from intensive care unit (ICU) clinicians during the mid-20th century. During this time, ICU monitoring and critical care medicine was just beginning to develop, and most intensivists focused on extending patients’ lives using advanced technology rather than comforting patients in their final days of life [1]. Despite intensivists’ efforts to save lives, approximately 540,000 patients die in ICUs annually in the United States, accounting for 22.4% of all deaths in the country [2]. Ultimately, intensivists recognized that they are not only responsible for saving lives, but also providing end-of-life care to terminally ill patients [3]. Furthermore, ICU resources are limited, and delivery of nonbeneficial treatment can undermine patient dignity. Therefore, there has been growing emphasis on the importance of research and education regarding advanced care planning, end-of-life care, and LSTW [1,4].
In South Korea, two prominent cases prompted public discussion regarding the decision to forego life-sustaining treatments (LSTs). The first case is the “Boramae Hospital Case (1997).” In this case, a doctor at Boramae Hospital withdrew life-sustaining mechanical ventilation from a patient who had suffered from a brain hemorrhage with the consent of the patient’s wife. In doing so, this physician was charged with aiding a murder. The second case is “Grandma Kim’s case (2008),” in which the Supreme Court ordered LSTW of a 77-year-old grandmother, Kim Ok-kyung, at the request of her family because she was in a persistent vegetative state [5-7]. These two conflicting court rulings involving LSTW confused clinicians. After these cases, there was growing public support in South Korea for enactment of the decision to forego LSTs.
After much discussion and public consultation, a law concerning “Hospice, palliative care, and withdrawal of life-sustaining treatment” was enacted in February 2016. A demonstration of the project was provided by the Korean Ministry of Health and Welfare before the law was enforced nationally on February 4, 2018 [5,6]. Thus far, this law has only been enforced for two years in Korea. Regardless, physicians use it to address their difficulties in making decisions regarding LSTW, because there is little precedent or research in clinical settings to which they can refer. Intensivists, in particular, encounter these difficulties often because of their constant exposure to critically ill patients.
It is of utmost importance to determine when to withhold or withdraw LST in critically ill patients in the ICU, as some medical interventions in this setting may be futile or against the wishes of terminally ill patients. LST for terminally ill patients without expected recoveries also leads to considerable cost [8,9]. Intensivists must not only concentrate on treating patients admitted to the ICU, but also address the redistribution of ICU resources. In addition, unlike the prior emphasis on medical paternalism, the approach has recently shifted to shared and engaged decision making among physicians, patients, and their families. This is particularly true regarding terminally ill patients, for whom a patient’s autonomy must be respected. Therefore, it is important for intensivists to provide patients and their families with clinical information to help them to decide on the extent of LST in patients at the end of life [10].
The purpose of this retrospective study was to identify the current status of decisions regarding LSTW for patients hospitalized in ICUs by reviewing cases that involved this at Ewha Womans University Medical Center Mokdong (EUMC-Mokdong). We also considered the role of ICU intensivists in the decision-making process regarding LSTW through separate examination of cases in which they participated in this process.
MATERIALS AND METHODS
Study Design and Population
The target population was patients aged ≥ 20 years who were hospitalized at EUMC-Mokdong, which is a tertiary medical institution with approximately 800 beds (including 54 ICU beds). To perform a retrospective analysis, we collected the medical records from 227 patients who had decided to withdraw LST between April 9 (when the LST consulting team was launched and decisions regarding LSTW began to be made) and December 31, 2018.
We collected data from 88 ICU patients who decided to withdraw LST. However, we only analyzed the baseline characteristics of 80 of these patients, because the hospitalization process was not complete for eight patients within the medical record collection period. In EUMC-Mokdong, dedicated ICU intensivists treat patients hospitalized in every department through consultation with other departments by applying an open ICU model. In cases in which the attending physician did not choose to consult with intensivists, the physician independently decided whether to continue or discontinue LST without the intensivists’ intervention. These patients were included in the control group.
Conversely, if the ICU was involved in cases in which the patient was receiving end-of-life care or who was terminally ill (and not responding to aggressive treatment), the intensivist consulted with the attending physician about withholding or withdrawing LST. If the physician judged that the patients would not survive despite aggressive treatment, the intensivists in charge communicated with patients’ families to decide whether to withhold or withdraw LST, and to determine the extent of the treatment to be provided. These cases were included in the intensivist group.
If intensivists judged a patient to be nearing the end of their life with no chance of survival, they completed the “Judgment Sheet on Patients in the End-of-Life Process,” along with the attending physicians in the relevant department, to decide whether to withdraw or withhold LST. This process also allowed the physicians to determine the extent of LST that would be provided based on interviews with the patient’s family. If the patient’s family so desired, the patient was transferred to a general ward, and the LSTW process was implemented. This process might involve extubation or the removal of a mechanical ventilator, and pain control.
We assigned the ICU patients into two groups depending on whether or not intensivists participated in the decision-making process to withdraw LST. We analyzed the differences between the two groups by comparing whether the decision was made to withdraw or withhold LST, the duration of ICU hospitalization, and the patients’ progress.
Data Collection
We collected and analyzed basic clinical data and information related to decisions regarding LSTW for patients hospitalized in EUMC-Mokdong who made such decisions and met the selection criteria. With regard to the basic clinical data, we recorded each patient’s age, sex, medical department, diagnosis, hospitalization ward, and Acute Physiology and Chronic Health Evaluation (APACHE) II score at the time of ICU hospitalization. We recorded the following information with regard to the decision to withdraw LST: the date on which the decision was made; the type of judgment; whether an intensivist participated in writing the patient’s end-of-life judgment sheet and completing the form for the decision to withdraw LST; LSTW interventions; and whether the decision to withdraw or withhold LST was implemented.
The clinical data were collected using Excel data and electronic medical records based on the forms for the decision to withdraw or withhold LST. These forms were as follows: confirmation of the patient’s intention to withhold or withdraw LST (advance directives or statements from patients’ families), confirmation of the patient’s family members’ intention regarding the LSTW decision, implementation of the decision to withhold or withdraw LST, application to access medical records, judgment sheet for patients in the end-of-life process, terminal patient’s management record card, and application for advance directives. The withdrawal or withholding of LST was performed by dedicated LSTW nurses in the hospital. Based on these data, we analyzed the characteristics of the patients who decided to withhold or withdraw LST. We also collected a list of ICU patients, and divided them into the two groups as described above. Between these two groups, we analyzed differences in the results regarding LSTW, such as: patients’ progress, length of stay in ICU, days before death after the decision was made to withdraw LST, and implementation of the decision to withhold or withdraw LST. This study was approved by the Institutional Review Board at EUMC-Mokdong (IRB No. 2019-02-034). Informed consent was waived.
Statistical Analysis
IBM SPSS ver. 25.0 (IBM Corp., Armonk, NY, USA) was used for the data analysis. With regard to the patients’ basic clinical data, continuous variables (such as age and APACHE II scores) were expressed numerically as means ± standard deviations. In cases in which the variables were not distributed normally, the variables are expressed as medians (interquartile ranges). Other nominal variables are expressed as numbers and percentages. We used a chi-square test and Fisher’s exact test to compare nominal variables that represented the basic clinical data and differences between the two groups. An independent t-test was performed to compare the mean values. A Mann-Whitney U-test was used when the dependent variables were not normally distributed. The significance level was set at P < 0.05.
RESULTS
Baseline Characteristics of the Participants
The general characteristics of the 227 patients who met the selection criteria during the study period are shown in Table 1. The department that decided to withhold or withdraw LST most frequently was the Department of Hemato-oncology (n = 60, 26.4%). Within this department, the most common diagnosis was cancer, and more specifically, gastrointestinal tract cancer (n = 66, 29.1%). Regarding the chosen LSTW interventions, the proportion of patients who decided not to receive any LST was the largest (64.3%). The remaining patients chose individual LST interventions (Table 2). Of these, the patients who chose not to receive cardiopulmonary resuscitation accounted for the largest proportion (32.2%; multiple responses). Regarding the forms for LSTW decisions, “Confirmation of the patient’s family members’ intention regarding the LSTW decision (agreement of all family members of unconscious patients)” accounted for the largest proportion of patients (52%), followed by “Confirmation of the patient’s intention to withhold or withdraw LST (statement from the patient’s family; 27.7%).” The number of cases in which advance directives for LST were prepared accounted for the lowest proportion of patients (20.3%) (Table 2).

General characteristics of patients who made decisions regarding LST during admission (admission patients) and during ICU admission (ICU patients)

Chosen interventions for withdrawing or withholding LST by group
Clinical Characteristics of ICU Patients
In total, 80 ICU patients decided to withhold or withdraw LST. The department that made LSTW in the ICU decisions most frequently was the Department of Neurosurgery (23 patients, 28.7%). The most common diagnosis in this department was cerebral hemorrhage (Table 1).
Of the ICU patients who decided to withhold or withdraw LST, 32 (40.0%) decided to withhold or withdraw all LST, while the remaining 48 decided to decline cardiopulmonary resuscitation (Table 2). In addition, 34 (42.5%) and 28 (35.0%) patients declined dialysis and mechanical ventilation, respectively (multiple responses). The number of cases in which LST was withheld was higher than those in whom LST was withdrawn (76.3% vs. 23.8%). In the ICU, most patients died (n=70, 87.5%) after the LSTW decision was made. The median number of days from ICU admission to LSTW decision was 8.0 (3.3–17.8). The average number of days between the decision and death was 3.0 (2.0–5.0) (Table 3).
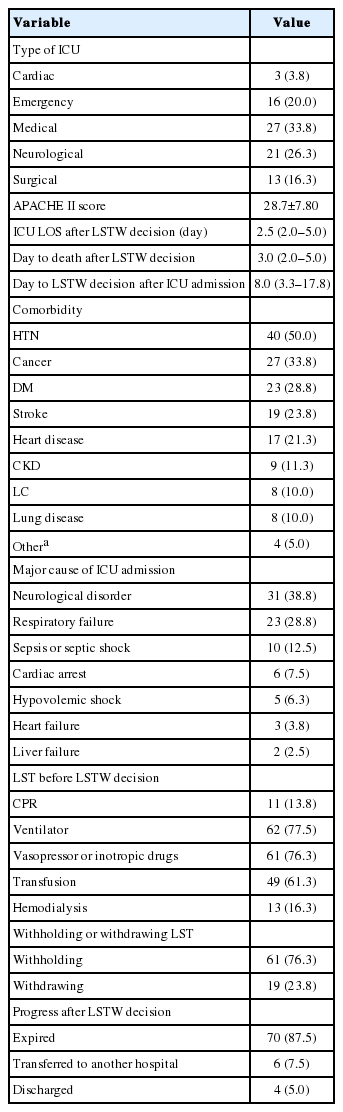
Clinical statuses and progress of ICU patients who decided to withhold or withdraw LST in EUMC-Mokdong Hospital
Comparing the Intensivists and Control Groups
Of the 80 ICU patients who decided to withhold or withdraw LST, the number of patients for whom intensivists participated in the LSTW decisions was 34 (Table 4). The patients’ age, disease severity (identified via the APACHE II scores), and comorbidities, did not differ significantly between patients for whom intensivists did and did not participate in the LSTW decisions (age, P = 0.950; APACHE II, P = 0.814).

Differences in characteristics between patients for whom intensivists did (intensivists group) and did not (control group) participate in LSTW decisions
The most common admission department in the intensivists group was neurosurgery (64.7%) and in the control group, pulmonology (23.9%, P < 0.001). The most prevalent comorbidity was hypertension (HTN) in both groups. Neurological disorders were the major cause of ICU admission in the intensivists group, while respiratory failure was the most prevalent cause of ICU admission in the control group (P = 0.002). In the intensivist group, the most common LST before the LSTW decision was mechanical ventilation (94.1% vs. 65.2%, P = 0.002). In the control group, the administration of vasoactive drugs was the most common LST (80.4% vs. 70.6%, P = 0.306).
Among the cases in which intensivists participated in the decision, the proportion of cases involving LST withdrawal was higher than that involving LST withholding (50.0% vs. 4.3%, respectively, P < 0.001). In addition, the proportion of patients who moved to the general ward from the ICU following the LSTW decision was significantly higher in the group in whom intensivists participated in the LSTW decision than it was when intensivists did not participate (52.9% vs. 19.6%, P = 0.002). The median duration of ICU hospitalization after the LSTW decision was shorter (2 days) when intensivists participated in the decision than it was when they did not (3 days), although this difference was not significant. The progress made by the patients in these two groups did not differ significantly.
Comparison between Withdrawn Group and Withheld Group
In order to identify the variables affecting the LST withholding or withdrawing, we divided the participants into a “withdrawn” group and a “withheld” group. There were 19 patients withdrawn from LST and 61 patients in whom LST was withheld (Table 5). There were no significant differences in age, APACHE II score, comorbidities, or days to LSTW decision between the two groups.

Differences in characteristics between patients who had LST withdrawn (withdrawn group) and withheld (withheld group)
Neurosurgery was the most common department to withdraw LST (78.9%), while the most common department for deciding to withhold LST was pulmonology (18.0%, P < 0.001). The most frequent cause for ICU admission in the withdrawn group was neurological disorder (78.9%), while respiratory failure accounted for the largest number of ICU admissions in the withheld group (37.7%, P < 0.001). Considering the type of LST, mechanical ventilation was significantly more frequently administered in the withdrawn group than it was in the withheld group (100.0% vs. 70.5%, P = 0.005).
DISCUSSION
This retrospective, single-institution study examined how LSTW has been conducted clinically since the law concerning “Hospice, palliative care, and withdrawal of life-sustaining treatment” was implemented in Korea. We analyzed differences between cases in which ICU intensivists did and did not participate in LSTW decisions.
There were no statistically significant differences in age, APACHE II score, comorbidities, or days from ICU admission to LSTW decision among the study participants. There were, however, significant differences between the two groups with regard to the medical department, main cause of ICU admission, and use of mechanical ventilation. Specifically, the most common department in the withheld group was neurosurgery, and the most prevalent cause of ICU admission was neurological disease. These findings are similar to the results of a previous study showing that neurological diagnosis is associated with withholding or withdrawing LST in ICU patients [11].
When comparing the intensivists group to the control group, we found significant differences in the medical department and the main cause of ICU admission. Neurological disorders were the most common cause of ICU admission in the intensivist group. This finding may be related to the fact that neurosurgery is the department in which intensivists are most frequently consulted. In addition, there was a significant difference between the two groups with regard to the medical department, which may have been influenced by the adoption of an open ICU model in the hospital where the study was performed. Intensivists in this hospital do not manage all patients admitted to the ICU. Instead, they participate in the care of patients for whom they are consulted by the attending physicians. Therefore, there appears to be a difference in the departments that frequently refer to intensivists and those that do not do so frequently depending on the tendency of each physician. Although there were differences between the two groups with regard to the medical departments, reason for ICU admission, and type of LST performed, we found that the intensivists group tended to withdraw LST rather than withhold LST compared to the control group.
In Asia, there is a weaker tendency toward LSTW for terminal ICU patients relative to that observed in the United States and Europe [12-14]. Moreover, Korea shows a stronger tendency toward active LST relative to that of other Asian countries for the same type of terminal patients (i.e., hypoxic-ischemic encephalopathy resulting from septic shock). In addition, Korea showed a tendency to withhold, but not withdraw, LST, even for patients who have “no chance of recovery to a meaningful life” [12]. This tendency may be attributable to many factors, such as religion, social culture, and the absence of a legal system [12,14,15].
However, our results demonstrated that attending doctors who were not ICU intensivists considered LST withdrawal more negatively than they did LST withholding. This tendency exists despite the fact that the legal system in Korea allows LSTW. There is a widely held opinion that there is no ethical difference between LST withdrawal and withholding [3,16,17]. Despite this, medical professionals’ unconditional insistence on only withholding LST (rather than withdrawing it) may not only prolong patients’ suffering, but also increase the cost of medical care resulting from prolonged LST. These choices may also lead to long-term economic burden to patients’ families and society in general [17,18].
Our results showed that the proportion of patients who decided to withdraw LST and the number of cases in whom patients were transferred to general wards from the ICU were higher when intensivists were involved in the LSTW decisions than they were when they were not. Although this difference was not statistically significant, the average duration of ICU hospitalization for patients in whom intensivists participated in the LSTW decisions was shorter than that observed for patients in whom intensivists did not participate. This finding may be due to the fact that, in the group in which intensivists participated in the LSTW decisions, both the attending physicians and intensivists extensively communicated with the patients’ families and helped them to make informed decisions. In this way, appropriate communication between medical staff and patients’ families can improve family members’ understanding of LST and help them to decide whether to withhold or withdraw treatment. This communication also allows patients to pass away in the presence of their family members in a private ward if this is requested by their families. Previous research has shown that high-quality communication between medical staff and families reduces the duration of ICU hospitalization [19,20]. In addition, other studies have found that sufficient communication can reduce the mental burden experienced by patients’ families and increase their satisfaction [21-23]. In addition, intensivists could not only reduce the length of time for which terminally ill patients receiving nonbeneficial treatment suffer by reducing the duration of ICU hospitalization, but also redistribute limited ICU resources appropriately [24].
This study has several limitations. It was a retrospective, single-institution study. Because of our hospital’s policy, there were significant differences between the intensivist group and control group with regard to the medical department and main reason for ICU admission. The study therefore may have been subject to selection bias because of differences between the two groups. In addition, because this study was focused on a small number of cases, we were unable to perform multivariate analysis between the intensivist and control groups. Given the study design, we are unable to identify causal relationships between the reported outcomes and the presence of intensivists’ participation. In addition, this study did not evaluate family members’ satisfaction with the LSTW decisions according to group. A well-designed, large-scale study is needed to examine these issues in the future.
The burden of ICU treatment is increasing worldwide [25], and the role of intensivists in end-of-life care will expand gradually. In the future, intensivists will need to triage the use of ICU resources and face increasing difficulties in determining when to move terminally ill patients from intensive treatment to palliative care. The results of this study suggest that intensivists can reduce patients’ suffering and the cost of medical treatment by communicating with patients’ families and ultimately reducing the duration of ICU hospitalization.
In the ICU, intensivists are not only responsible for saving the lives of critically ill patients, but also of addressing these patients’ quality of life. Therefore, intensivists must fully understand the ethical issues and legal systems that are related to LSTW decisions. In addition, intensivists must recognize the importance of appropriate communication with the families of terminally ill patients.
KEY MESSAGES
▪ Despite the enactment of a law regarding withdrawal of life-sustaining treatment, attending doctors who are not intensivists are less likely to withdraw life support than are intensivists.
▪ In the group in which intensivists participated in the decision-making process, intensivists helped patients’ families to reach decisions.
▪ After life-sustaining treatment withholding and withdrawal decision, patients were transferred to the general wards significantly more often than they were in the group in which intensivist did not participate.
Notes
CONFLICT OF INTEREST No potential conflicts of interest relevant to this article were reported.
Acknowledgements
We thank the dedicated LSTW nurses in Ewha Womans University Medical Center Mokdong for their help in data collection.
Notes
AUTHOR CONTRIBUTIONS
Conceptualization: SIL, JP, YJL. Data curation: SIL. Formal analysis: SIL, KSH. Methodology: SIL, JP, KSH. Project administration: SIL, YJL. Visualization: SIL, KSH. Writing–original draft: SIL, JP. Writing–review & editing: all authors.