The quality of dying and death for patients in intensive care units: a single center pilot study
Article information

Abstract
Background
To identify the necessary care for dying patients in intensive care units (ICUs), we designed a retrospective study to evaluate the quality of dying and death (QODD) experienced by the surrogates of patients with medical illness who died in the ICU of a tertiary referral hospital.
Methods
To achieve our objective, the authors compared the QODD scores as appraised by the relatives of patients who died of cancer under hospice care with those who died in the ICU. For this study, a Korean version of the QODD questionnaire was developed, and individual interviews were also conducted.
Results
Sixteen people from the intensive care group and 23 people from the hospice care group participated in the survey and completed the questionnaire. The family members of patients who died in the ICU declined participation at a high rate (50%), with the primary reason being to avoid bringing back painful memories (14 people, 87.5%). The relatives of the intensive care group obtained an average total score on the 17-item QODD questionnaire, which was significantly lower than that of the relatives of the hospice group (48.7±15.5 vs. 60.3±14.8, P=0.03).
Conclusions
This work implies that there are unmet needs for the care of dying patients and for the QODD in tertiary hospital ICUs. This result suggests that shared decision making for advance care planning should be encouraged and that education on caring for dying patients should be provided to healthcare professionals to improve the QODD in Korean ICUs.
INTRODUCTION
More than 75% of all deaths in Korea occur in hospitals [1]. However, domestic studies on the quality of dying and death in hospitals are rare. In intensive care units (ICUs), a large number of patients with terminal illnesses die while receiving life-sustaining treatments. Treating terminally ill patients with dignity is an important role for medical professionals [2]. For this reason, it is necessary to survey the quality of dying and death for patients in ICUs and hospices.
The quality of dying and death (QODD) is a tool proposed by Patrick et al. [3] through systematic literature studies that measures the quality of care for dying patients. The tool’s validity and reliability have been evaluated and demonstrated [4], and has been translated into other languages, including German, Spanish, and Korean [5-7].
To identify the necessary care for dying patients in ICUs, we studied the quality of dying and death experienced by the surrogates of patients with medical illnesses who died in the ICU of a tertiary referral hospital. For this, the authors compared the QODD as appraised by the family members of patients who died of cancer under hospice care with those who died in the ICU. For this study, a Korean version of the QODD questionnaire was developed and individual interviews were conducted.
MATERIALS AND METHODS
Screening Participants
The researchers screened medically ill patients over 18 years old who died either in the adult ICU or under hospice care at a single tertiary medical center in the period between October 2016 and October 2017. We reviewed their hospital records for any suggestion of the patient’s medical futility, which refers to medically irreversible conditions or an active dying process with or without life-sustaining treatment. Based on the medical records, major medical decision makers or family members were selected for the questionnaire survey. Patients whose deaths occurred within the previous 4 weeks were excluded from the study. Also excluded were those deceased who had stayed for less than 72 hours at the ICU and who received hospice care for 2 weeks or less. Relatives who declined to participate in the questionnaire survey were excluded from the comparative analysis. Their reasons for nonparticipation were noted.
Study Design and Ethical Considerations
The institute in which this study was carried out is a tertiary referral medical center. The ICUs in this center have 56 beds and the hospice has 15 beds. The hospice at the hospital is the only accredited facility in the district that provides in-hospital care, home-visiting care, and consultative services. The hospice employs trained specialists. The institute provided standard pain management for the care of dying patients according to guidelines [2,8,9].
Patient information was collected from medical records. A standardized questionnaire for the QODD was used during individual interviews conducted by trained researchers. When face-to-face interviews were not available, postal or email correspondences were used. Two researchers, one from the ICU and the other from the hospice, underwent two training sessions on the questionnaire to obtain correct responses and eliminate potential biases.
The purpose of the study was explained to the survey participants. The participants consented to the study by participating in the survey, and the consent form was waived. This study was approved by the Ethics Committee of Chungnam National University Hospital (IRB No. 2018-03-038-001).
Questionnaire of the Quality of Dying and Death
This study adopted the “Quality of Dying and Death–17-item version” developed by Downey et al. [10], which employed 17 questions of the highest priority from the original “Quality of Dying and Death–31-item version” [4]. The questions were translated into Korean before they were revised and finalized after review by four researchers. Each question has two parts. The first asks relatives how often the deceased experienced each item using a scale, where 0 is “none of the time” and 5 is “all of the time.” Some questions require a “yes” or “no” response instead of a scale. The second part asks relatives to rate that aspect of the deceased’s dying experience on a scale from 0 to 10, where 0 is a “terrible experience” and 10 is an “almost perfect experience.” A total score was presented within a range of 0 to 100 after adding the sum of all the scores from the questionnaire and dividing it by the number of questions. This means that the higher the total score, the greater the quality of dying and death [4]. The 17-item questionnaire consists of the following five domains: (1) symptoms and personal control; (2) preparation for death; (3) family; (4) treatment preferences; and (5) whole person concerns [10].
Statistical Analysis
Data were presented as the mean or median for continuous variables or as numbers with percentages for categorical variables. Non-normally distributed data were expressed as ranges with minimum and maximum value. We used skewness to measure the asymmetry of the probability distribution. For a unimodal distribution, negative skewness indicates that the tail on the left side of the probability density function is longer than on the right. Conversely, positive skewness indicates that the tail on the right side is longer than on the left.
Nominal variables were compared using a chi-square or Fisher exact test, and the mean values in the two groups were compared using a Student t-test. Non-normally distributed continuous variables were compared using a Mann-Whitney U-test. Statistical significance was defined as P < 0.05. Statistical analyses were performed using PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Participants
During the study period, 1,289 medically ill patients were admitted into the ICU. Among them, 92 patients died while receiving medical treatments in the ICU. The researchers screened 40 patients eligible for the selection criteria.
The surrogates of eight patients were not reachable. Of the remaining 32, 16 surrogates participated in the face-to-face survey and completed the questionnaire (participation rate of 50%; completion rate of 100%) (Figure 1). The main reason given for declining participation was to avoid bringing back painful memories (14 people, 87.5%).

Flowchart of the survey.
During the study period, 93 terminally ill cancer patients died while on in-hospital hospice care or home-visiting hospice care. Among them, 34 relatives were eligible for the selection criteria. Twenty-six surrogates agreed to participate in the survey, but only 23 of them completed the questionnaire, either by 16 postal correspondences or seven face-to-face interviews (participation rate, 76.5%; completion rate, 88.5%) (Figure 1).
The median age of the participants in the intensive care group was 52 years. The majority of the survey participants from this group were adult children (15 participants, 93.8%) (Table 1). The median age of the participants in the hospice group was 55 years, and among these participants, 12 adult children (56.5%) and nine spouses (39.1%) participated in the survey.
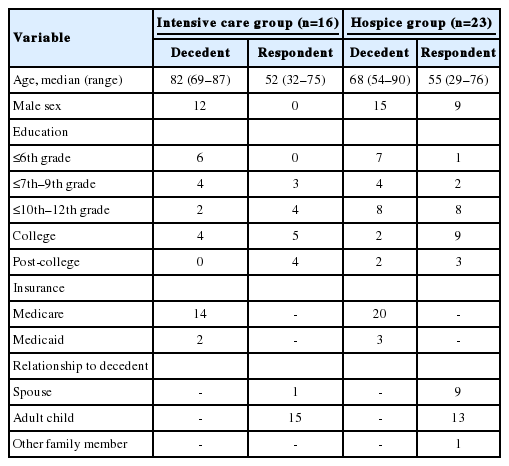
Demographics of the decedents and respondents who participated in a QODD questionnaire
Characteristics of Patients
The median age of the deceased from the intensive care group was 82 years, and 12 patients from this group were male (75.0%) (Table 2). In this group, infection-related illnesses accounted for 56.2% of deaths, including six deaths from pneumonia and three deaths caused by other infections (Table 2). The median length of stay in the ICU was 18 days. Fourteen patients died in the ICU, while two patients died in a general ward after being transferred for end-of-life care in their last days. All 16 patients received active intensive care for prolonging their life, such as mechanical ventilation, within 7 days of their death, but their conditions were medically irreversible (Supplementary Table 1). They had all provided a documented (81.2%) or verbal (18.8%) DNR (do not resuscitate) order, according to advance directive (6.3%) or advance care planning (93.7%) with their surrogate.

Demographics of intensive care group and hospice care group
The median age of the 23 patients from the hospice group was 68 years. Fifteen of these were male (65%) (Table 2). The causes of all of the deaths in this group were cancers (22 solid cancers and one hematologic malignancy). Ten patients died in the hospice, while 13 patients died in their homes. None of the patients received any life-sustaining treatments such as mechanical ventilation during the last 7 days prior to their deaths.
The Quality of Death
QODD total score
The average total score on the 17-item QODD questionnaire from the family members of the intensive care group was 48.7 (standard deviation [SD], 15.5; skewness value, 0.114). The average total score from the family members of the hospice group was 60.3 (SD, 14.8; skewness value, 0.164). The lower average QODD total score from the intensive care group was statistically significant (P = 0.03) (Figure 2).
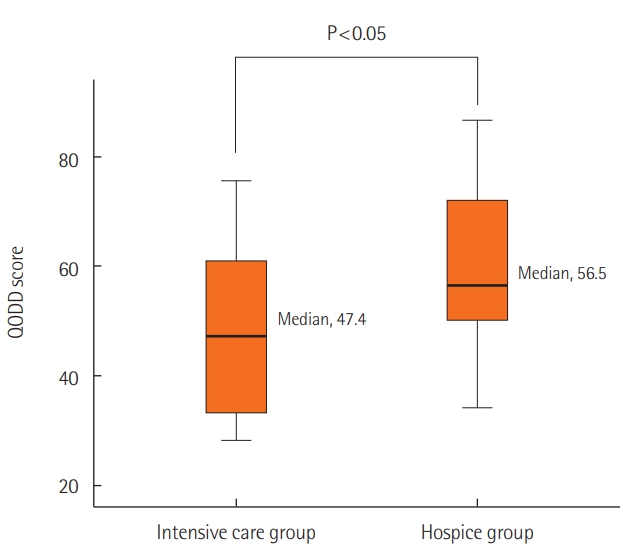
Comparison of quality of dying and death (QODD) between the intensive care group and hospice care group.
QODD by domains and items
Symptoms and personal control
Although the patients in the intensive care group had been provided pain management according to pain assessment protocols, their relatives’ rating for the QODD “pain under control” item was lower than that of the hospice group (2.1 vs. 5.3, P = 0.001) (Table 3). The intensive care group relatives’ rating for the “breathing comfort” item was significantly lower than that of the hospice group (2.1 vs. 4.1, P = 0.032) (Table 3).

Comparison of family respondents’ ratings between the intensive care group and hospice care group
Preparation for death
The relatives of the intensive care group provided ratings for the “untroubled about strain on loved ones” item and the “funeral arrangements in order” item that were significantly higher than those of the hospice group (P = 0.007 and P = 0.043, respectively) (Table 3). However, this group’s rating for “good-byes said” was significantly lower than that of the relatives of the hospice group (3.5 vs. 6.3, P = 0.030) (Table 3).
Family
On the question, “How often did the deceased spend time with family and friends,” the intensive care group’s rating for “time with the children” was significantly lower than that of the hospice group (4.6 vs. 7.8, P = 0.010).
Treatment preferences
All patients from the intensive care group had been receiving life-sustaining treatments, including mechanical ventilation. Their relatives’ rating for the QODD was significantly lower than that of the hospice group (5.2 vs. 8.2, P = 0.053).
Whole person concerns
On the question of “dignity and self-respect,” the rating of the relatives of the intensive care group was statistically significantly lower than that of the hospice group (2.6 vs. 6.5, P = 0.001).
General review by participants
For the “QODD of decedent’s last days,”’ the rating of the relatives of the intensive care group was lower than that of the hospice group (4.3 vs. 6.9, P = 0.126), although this result was not significant.
Subgroup Comparison on the QODD in the Intensive Care Group
In the intensive care group, some respondents rated a higher total QODD score than others. The ratings for the following items were significantly higher in the rater group with higher QODD scores than those in the latter group: “untroubled about strain on loved ones,” “healthcare costs covered,” “spiritual advisor visits,” and “funeral arrangements” (Table 4). In this group, two patients were transferred out of the ICU for end-of-life care in their last days and died in a general ward death bed. The ratings of the QODD from the relatives of these two patients were higher than those of the relatives whose loved ones died in the ICU (median, 64.5 vs. 45.0, P = 0.095).

Comparison by subgroups of the decedents in the intensive care unit and factors associated with QODD total score
DISCUSSION
Settings of ICUs are not conducive to the provision of palliative care. However, it has become an important task for medical professionals in ICUs to provide an appropriate level of palliative care in accordance with the diverse medical conditions of patients [2,11].
The goal of palliative care is to improve quality of life for both the patient and the family by focusing on providing relief from the symptoms and stress of a serious illness [12]. According to this definition, palliative care should not only provide continuous medical care until death, but should also provide various evidence-based interventions aimed at relieving patients’ pain and their relatives’ suffering [11]. Therefore, the experience of patients and their relatives is an important factor in assessing the quality of palliative care in ICUs.
However, it can be argued that a better way of assessing the quality of palliative care is to directly ask patients with terminal illnesses and their caregivers questions about their experiences [10]. Evaluating patients and their family members’ experience could identify unsatisfactory healthcare services and provide opportunities to improve the quality of hospital care. Understanding the current level of quality of care and identifying performance goals must precede improving the quality of care [11,13].
Previous studies have identified and presented the key areas of the QODD through various research methods, including questionnaire surveys, group interviews with patients and relatives, and expert opinions and intervention studies [14- 19]. Patrick et al. [3] presented the six areas of the QODD: “symptoms and personal care,” “preparation of death,” “moment of death,” “family,” “treatment of preferences,” and “whole person concerns.” The above measuring tools broadly encompass the two key aspects of the QODD: “appropriateness of scientific and medical care” and “appropriateness of personal and cultural aspects of care.” This approach supports the fact that many studies assessing the QODD of critically ill patients in the ICUs use such domains and items [20,21].
This study is based on comparative assessments of the QODD questionnaire by family members whose loved one died either in the ICU or in hospice. There a couple potential issues related to this methodology. First, compared to the hospice, the ICU has very different functions and purposes. Therefore, it could be that the characteristics of the patients from these two groups are not identical. However, there are two commonalities between the two groups. First, medical professionals were able to predict patients’ incurability and death. Although the underlying causes were different, all the decedents in the two groups were irreversibly incurable regarding their medical condition. In this study, advance care planning including DNR orders had been given to critically ill patients in the intensive care group as well as to terminal cancer patients in hospice care. Second, patients from both groups needed palliative care and end-of-life care during their last days. The hospice patients received standardized palliative care and end-of-life care during their last days. However, the design to allow the omission of essential palliative care on the predetermined grouping even in the same ICU would lead to critical ethical conflict. Therefore, as demonstrated by previous studies, the hospice group can help us to identify unmet needs of the patients from the ICU [22,23].
A second issue could be that the experience and perception of the deceased are not necessarily the same as their relatives’ [3]. The main participants of this study are the close relatives who cared for the deceased. It is quite possible that the relatives may not be able to accurately assess symptoms, care experience, and the perceptions of the patients [3]. However, it is important to acknowledge that the assessments from the relatives based on their experience of caring would closely reflect the actual perceptions of the quality of care that healthcare providers may not identify [3,17].
The QODD total score and QODD by domains and items in the ICU group are lower than those of the hospice group, which was the natural expectation in this study. However, there are a few findings from this study. First, the survey participation rate from the relatives of the intensive care group was lower (n = 16, 50.0%) than that of the hospice group. The main reason given for the low participation was to not “bring back the memories.” The relatives of the hospice group would receive emotional support from the hospice during their grieving process. Conversely, the relatives of patients in intensive care do not generally receive such emotional support, even though death can occur rather suddenly. There was no way of knowing how the nonparticipating relatives would have assessed the QODD, but it is reasonable to assume that the high decline rate and the reason for its declining reflect an inappropriate level of care in the ICUs.
Second, this study found that for both groups, “opportunity to avoid or choose life-sustaining treatments” was important and was correlated with the QODD. In Korean culture, terminally ill patients had difficulty determining even their own life-sustaining treatments regarding their previous advance directives by February 2018. This may hinder the essential advance care planning process for improving quality of dying and death. Many physicians feel uncomfortable in beginning and leading conversations regarding end-of-life care for multiple reasons, including personal attitudes [24,25]. These imply that education for healthcare professionals should be provided to enhance clinicians’ performance in caring for dying patients in the ICUs. Recent guidelines also support that medical professionals should have knowledge and competence for end-of-life care [2,26,27].
Last, this study found that relatives needed enough time to accept and prepare for their loved one’s death once the treatment to prolong the patient’s life was determined to be futile. In the intensive care group, respondents with a higher QODD experience were highly satisfied with questionnaire items such as “spiritual advisor visits,” “funeral arrangements,” “goodbyes said,” and “time with children.” Such items are associated with better end-of-life care. For this, shared decision making, including advance care planning, should be encouraged early in ICUs. Many studies found that good communication with medical professionals was a major factor affecting satisfaction of the relatives [28,29]. In ICUs, good communication and shared decision making among stakeholders may provide dying patients with better end-of-life care to improve their QODD in their last days [27,30,31].
This study designed a retrospective survey of the QODD to identify unmet needs for the care of dying patients in ICUs. By assessing the intensive care group relatives’ perceptions of the QODD, this study suggests, as have previous studies, that there are unmet needs for the care of dying patients in the ICU. A few limitations of this study should be noted. The participants of the study were possibly biased, as the participants were from a single referral hospital. Further, since the participants were a small group, selection bias could not be avoided. The assessment tool, i.e., the QODD, was developed for those in the United States. Therefore, social and cultural differences should be acknowledged and a more measured interpretation of the results from this study is needed.
In conclusion, this study found that in this tertiary referral hospital’s ICU, there are unmet needs for the care of dying patients and for the quality of dying and death. This result suggests that shared decision making for advance care planning should be encouraged and that education on caring for dying patients should be provided to healthcare professionals to improve the quality of dying and death in Korean ICUs.
KEY MESSAGES
■ The survey participation rate from the relatives of the intensive care group was lower (50.0%) than that of the hospice group (76.5%), with the reason of avoiding painful memories.
■ The total score of the quality of dying and death (QODD) from the family members of the intensive care group was statistically significantly lower than that of the hospice group.
■ This study implies that there are unmet needs for the care of dying patients and for the quality of dying and death in intensive care units.
Notes
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
Acknowledgements
This study was completed as a policy research project (2017) with the financial support of the Korea National Institute for Bioethics Policy (KoNIBP).
We are indebted to Yeon-sil Choi and Young Sim Choi for the data collection of this article. Also we are grateful to Hospice Care Team of Chungnam National University Hospital for their hard work.
Notes
AUTHOR CONTRIBUTIONS Conceptualization: JYM, MP. Data curation: YC, JL. Formal analysis: YC, JYM. Funding acquisition: MP. Methodology: MP, YC, JYM. Project administration: JYM, DHK. Visualization: DHK. Writing - original draft: YC, JYM. Writing - review & editing; JYM, HA.
Supplementary Materials
The online-only supplement data are available with this article online: https://doi.org/10.4266/acc.2018.00374.