Medical Management of Brain-Dead Organ Donors
Article information

Abstract
With improving healthcare services, the demand for organ transplants has been increasing daily worldwide. Deceased organ donors serve as a good alternative option to meet this demand. The first step in this process is identifying potential organ donors. Specifically, brain-dead patients require aggressive and intensive care from the declaration of brain death until organ retrieval. Currently, there are no specific protocols in place for this, and there are notable variations in the management strategies implemented across different transplant centers. Some transplant centers follow their own treatment protocols, whereas other countries, such as Bangladesh, do not have any protocols for potential organ donor care. In this review, we discuss how to identify brain-dead donors and describe the physiological changes that occur following brain death. We then summarize the management of brain-dead organ donors and, on the basis of a review of the literature, we propose recommendations for a treatment protocol to be developed in the future.
INTRODUCTION
Every day, the demand for organs [1] is increasing at a faster rate than that at which organs are becoming available for transplants. With this increasing demand, the responsibility with regard to caring for potential organ donors is also rising. Appropriate medical management of a potential organ donor is a very important issue, requiring a multidisciplinary team approach for successful organ transplantation [2]. For graft survival after donation, all available organs in the donor need to be maintained at their normal physiological condition until the time of organ retrieval [1]. Intensivists play a vital role in the management of potential organ donors through the identification of potential donors, declaration of brain death, and proper medical care—all of which can improve the rates of graft survival [2-4]. There are many countries worldwide that lack proper guidelines on the identification and management of potential donors, including Bangladesh. Early identification of a potential donor is critical in starting early medical management for successful organ transplantation.
A potential organ donor is defined by the presence of either brain death or a catastrophic and irreversible brain injury that leads to fulfilling the brain death criteria [5]. Brain death is defined as the irreversible loss of all brain functions, including the brain stem [6]. Brain death occurs in response to increased intracranial volume, which may be caused by brain swelling and the collection or obstruction of cerebrospinal fluid flow (hydrocephalus) [7,8]. As the intracranial pressure (ICP) rises, blood flow to the brain falls and finally stops: the brain dies=irreversible=patient death [7,8].
To diagnose and declare brain death, certain criteria need to be fulfilled, including [7,8]; (1) irreversible coma, (2) absence of brain stem reflexes, and (3) no self-respiration. Evaluation of brain death should be considered in patients who have suffered a massive, irreversible brain injury with identifiable causes. A patient determined to be brain-dead is legally and clinically dead [6]. Sometimes, it may be difficult to differentiate brain death from other medical states, such as barbiturate overdose, alcohol intoxication, sedative overdose, hypothermia, hypoglycemia, coma, and chronic vegetative states [9].
A brain-dead individual shows no clinical evidence of brain function upon physical examination, which includes no response to pain and no cranial nerve reflexes. Additionally, there is no pupillary response (fixed dilated pupils), oculocephalic reflex, corneal reflex, no response to the caloric reflex test, and no spontaneous respiration [9]. Brain electrical activity stops completely or drops to such low levels that they are undetectable with most equipment; an electroencephalogram (EEG) will therefore be flat, although this can also be observed during deep anesthesia or with cardiac arrest [10]. An EEG is considered a confirmatory test, whereas other tests, such as transcranial Doppler ultrasonography and cerebral scintigraphy (technetium Tc 99m exametazime), are regarded as ancillary tests. However, cerebral angiography is considered the most sensitive confirmatory test in the determination of brain death [11].
If the vital organs can be maintained and kept functional in the body of brain-dead patients by continuing mechanical ventilation and other life-support measures, it will provide an optimal opportunity for performing transplantations [9]. Once neurologic death is declared, the intensivist can play an important role in implementing appropriate management strategies to preserve organ function to maximize successful organ procurement. This can even begin prior to family discussions about organ donation [12]. Organ donor management should be started immediately after brain death occurs and should continue once consent from the family for donation is obtained [5].
Data shows that progression from brain death to somatic death results in the loss of 10% to 20% of potential donor tissues, therefore timely treatment of the donor is very crucial [5]. Strict organ-protective intensive care of the potential organ donor is therefore the first step towards a successful transplant and in the treatment of the future organ recipient [13]. Continuing care for the brain-dead donor is often critical, difficult, and complex, and may extend over several hours or even days.
It is assumed that the preferred goal for successful organ donation is to maintain the hemodynamic variables and laboratory parameters within the normal ranges [14]. Thus, the guidelines we propose mainly focus on maintaining normal hemodynamic values and laboratory parameters as the therapeutic goals. It is agreed that portions of these guidelines may differ from established treatment protocols from individual organ procurement organizations (OPOs) across different countries. However, our guidelines have been prepared based on our own clinical experience in brain-dead donor management and standard critical care practice. We offer these considerations to those centers or countries, like Bangladesh, where there are currently no proper guidelines available for donor care. Final treatment objectives and management should be determined by local OPOs or authorities.
PATHOPHYSIOLOGICAL CHANGES IN IRREVERSIBLE LOSS OF BRAIN FUNCTION
Different clinical studies have shown that central sympathoadrenergic regulation of circulation and the pituitary temperature are disrupted during development and irreversible loss of brain function; thus, there is an interruption in hypothalamic-pituitary-adrenocortical regulation [15]. The rising ICP results in a massive release of proinflammatory and anti-inflammatory cytokines and catecholamines [16]. Ultimately, brain death results in the loss of central regulatory mechanisms, which leads to several pathophysiological alterations in hemodynamics, hormone balance, body temperature, and lung function (Table 1) [13,17-19].
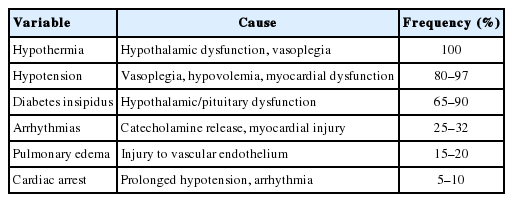
Frequency of pathophysiological changes in irreversible loss of brain function
Cardiovascular Changes
In a brain-dead patient, ICP rises, which compromises cerebral blood flow and causes hemodynamic changes, described as the “Cushing reflex,” which is a mixed picture of vagal and sympathetic stimulation. As pontine ischemia develops, it clinically manifests as bradycardia and hypertension [20]. When blood supply is further compromised, ischemia progresses to the medulla oblongata, involving the vagal motor nucleus [20]. This results in compensatory arterial hypertension, perhaps associated with bradycardia, followed by marked sympathetic stimulation with intense vasoconstriction, raised systemic vascular resistance, and tachycardia [2]. This clinical picture is known as the “catecholamine storm,” and these features are also associated with central redistribution of blood volume, increased afterload, and visceral ischemia [2].
The level of increase in catecholamines is dependent upon the rate of increasing ICP and may even elevate as much as 1,000-fold from baseline if the ICP rises very rapidly [21]. The effects of the catecholamine surge on the myocardium results in an altered metabolism associated with depletion of adenosine triphosphate in the cardiac myocyte. This is evidenced by the fact that 20%–25% of brain-dead donors show evidence of myocardial ischemia with 40% showing echocardiographic evidence of myocardial dysfunction [21]. Acute myocardial injury occurring around the time of brain death has been identified in both animal and human studies [2].
As ischemia progress down the spinal cord, it may cause loss of function in the thoracic sympathetic chain with severe hypotension resulting from a reduction in afterload. As the aortic diastolic pressure decreases, it may compromise the coronary perfusion pressure to critical levels, resulting in myocardial ischemia [20]. The resulting hypotension may lead to hypoperfusion of all organs, including the heart, if not properly and timely treated, and may contribute to rapid donor loss [22]. Additional factors may contribute to hypotension, including diuretics (mannitol), hyperglycemia-induced osmotic diuresis, diabetes insipidus (DI), hypothermic “cold” diuresis, inadequate fluid resuscitation and decreased oncotic pressure after crystalloid resuscitation, ongoing blood loss, rewarming of the patient, and relative adrenal insufficiency as a result of trauma, and critical illnesses [5].
Respiratory Changes
The lungs are the organs most often assumed to be medically unsuitable for transplants, with only 10%–20% of lungs eligible for transplantation [23]. Neurogenic pulmonary edema (NPE) and inflammatory acute lung injury are the two main factors related to brain-death-induced lung injury and dysfunction [24]. In a brain-dead person, the NPE is related to a sympathetic storm caused by hemodynamic and sympathetic mechanisms. NPE can occur immediately after a neurological insult, but it may also occur earlier, before the patient is distinguished as a potential organ donor [25]. The sympathetic storm leads to systemic vasoconstriction and an increase in cardiac afterload, thus increasing left ventricle and left atrial pressures. The blood is shifted from the periphery to the central compartment, causing an increase in both pulmonary blood volume and pulmonary artery pressure. Increased left atrial and pulmonary artery pressures may lead to a massive increase in pulmonary capillary pressure and pulmonary edema. This elevated hydrostatic pressure would ultimately lead to structural damage to the capillary endothelium [25]. Respiratory arrhythmias may progress to apnea and cardiac arrest if there is no supporting mechanical ventilation [2].
In addition, proinflammatory mediators that are released following brain death may further contribute toward lung injury by promoting infiltration of activated neutrophils into the lungs [26]. Other contributing factors for lung dysfunction include chest trauma, aspiration, and atelectasis [17]. Moreover, long-term dependency on mechanical ventilation also creates a predisposition toward nosocomial chest infections [20].
Renal Changes
Experimental models have demonstrated that biomarkers for renal tubular injuries may be elevated as early as 30 minutes after the onset of brain death [20]. Both proinflammatory and procoagulant effects caused by brain death have been identified as main contributing factors [20]. Pretransplant kidney biopsies of a brain-dead donor found that the kidneys contain more infiltrating T lymphocytes and macrophages compared to those from living and cardiac-dead donors. There is also compelling evidence showing a greater release of inflammatory cytokines during reperfusions in brain-dead donor kidneys [27].
Endocrine Changes
Brain death may cause significant endocrine changes that vary in timing and severity, resulting in anterior and posterior pituitary failure [28]. Animal studies have shown that in baboons with acute increases in ICP, posterior and anterior pituitary function is rapidly lost after brain death [29], which is associated with deterioration in cardiac function and a shift to an anaerobic metabolism. However, the profile is less consistent in the case of human donors [2].
Function of the posterior pituitary gland becomes clinically lost in as many as 80% of brain-dead organ donors, which results in the development of DI with electrolyte imbalances, hypovolemia, and circulatory instability, and can create major problems in organ donor management [30,31]. DI develops because of a lack of anti-diuretic hormones released from the posterior pituitary gland, and if left untreated, can causes polyuria and result in hypovolemic shock and hypernatremia. Other causes of polyuria, such as hyperglycemia or the use of a diuretic or osmotherapy, should be excluded before considering a diagnosis of DI [20].
Usually, anterior pituitary function appears to be preserved or partially affected due to preserved pituitary blood flow [32]. Most donors show normal values of thyroid-stimulating hormones (TSH), adrenocorticotropic hormones, and human growth hormones, which indicate there is some residual function and, thus, perfusion of the hypothalamic pituitary neuroendocrine system [28]. Thyroid hormones and TSH levels show the typical picture of “sick euthyroid syndrome” that actually accompanies severe brain injury, rather than as a result of TSH deficiency [28].
Hyperglycemia is also a common endocrine change in brainstem-dead patients due to reduced insulin concentrations and insulin resistance [2]. In addition, hyperglycemia may worsen with stress, alterations in carbohydrate metabolism and the use of glucose solutions; however, as C-peptide levels increase over time, insulin levels will subsequently normalize [21]. If untreated, hyperglycemia may cause pancreatic cell damage, which may affect pancreatic graft; therefore, measures should be taken to maintain strict euglycemia to minimize this risk [21]. Untreated hyperglycemia may also affect outcomes after a renal transplantation [33].
Systemic Inflammatory Response
An active systemic inflammatory response is a common and typical picture of all brainstem-dead donors [34] and can be quite severe. Although inflammation may be associated with trauma and other critical illnesses, it can be particularly severe in a brain-dead donor as mediators are released from the damaged brain. Additionally, generalized ischemia-reperfusion injury, metabolic changes at the time of the catecholamine storm, or failure to adequately restore to the normal cardiovascular state further complicate matters [2]. Plasma levels of interleukin-6 also increase in the donor and may lead to poorer graft utilization and subsequent graft dysfunction [35].
Hematological Changes
Anemia is commonly found in brain-dead patients when traumatic bleeding occurs, with coagulopathy and fluid administration further exacerbating the condition [36]. Isolated head injuries are present with coagulopathy in 34% of cases [37]. Necrotic brains release tissue thromboplastin [38] and plasminogen activators, which are also released from cerebral injuries, and result in disseminated intravascular coagulation [20]. Bleeding complications may occur due to a deranged coagulation profile (prothrombin and activated partial thromboplastin time) and thrombocytopenia [20]. Leukocyte count may be elevated from the cerebral insult, with a systemic inflammatory state or nosocomial infection possibly occurring in the later stages [20].
Hypothermia, Stress, and Metabolic Responses
Hypothermia is a common feature in brain-dead organ donors due to the loss of thermoregulatory control, exposure to cold ambient temperatures, or massive infusions of cold intravenous (IV) fluids or blood products [39]. It may also occur due to a reduced metabolic rate, excessive heat loss, or loss of protective mechanisms such as vasoconstriction or shivering [2]. Preventing hypothermia is preferred rather than attempting to treat it. Once hypothermia develops, it is difficult to warm patients and may directly affect cardiac function, induce arrhythmias, coagulation cascades, and interfere with oxygen delivery to tissues [36].
PRACTICAL ASPECTS OF ORGAN DONOR MANAGEMENT
The fundamental principles of organ donor management in intensive care units (ICU) are based on monitoring programs and therapies. These include confirmation of therapeutic goals, regular review of the donor patient’s state, and prompt changes in therapy when required [2]. The medical management of the potential brain-dead organ donor is often dependent on the discretion of the primary critical care team with considerable variation in practices between ICUs [20].
The target of management is to maintain physiological homeostasis in order to continue optimal organ function and to maximize graft viability in the organ recipient [20]. Given the variation in management protocols, donor goals were developed to establish a standard protocol aimed at maintaining the physiology close to normal values based on routine monitoring of ICU patients [2]. An early and easy-to-remember series of goals were established known as the “rule of 100” [40]: systolic arterial pressure >100 mmHg, urine output >100 ml/hr, arterial partial pressure of oxygen (PaO2) >100 mmHg, and hemoglobin concentration >100 g/L. Later, an additional goal was included: “blood sugar 100% normal” (Gelb AW, personal communication; 2011).
Although there is still considerable variation in treatment protocols, application of management techniques, donor acceptance, and achievement of donor goals [41,42], a higher number of transplantable organs is possible using protocols or systems that can easily and reliably promote achievement of management goals [43].
Temperature Management
Prevention of hypothermia should be preferred compared with its reversal. It is easier to prevent hypothermia by actively warming the donor body, and bodies with temperatures <34°C should be subjected to core warming [36]. Surface warming should be performed for all patients with hypothermia and should be continued to maintain a temperature over 35.8°C before and during the retrieval operation [28,44]. Active warming can be achieved using warm blankets, fluid warmers, and heated humidifiers in ventilator circuits [39], as well as by adjusting the ambient temperature.
Cardiovascular Management
Hemodynamic goals
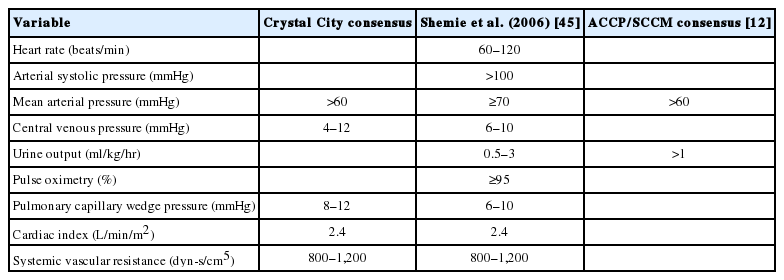
Goals for the management of hemodynamic status in donors are as follows [5]: (1) to maintain normovolemia; (2) to control blood pressure (BP); (3) to optimize cardiac output (CO) to maintain perfusion pressure of all organs; and (4) to minimize use of vasoactive agents. Although some consensus recommendations have been made (Table 2) [20,45], currently, there is still a lack of clear evidence for recommendations on ideal hemodynamic goals in organ donor management. Logically, recommendations on BP values should be individualized; for example, higher BP targets for potential organ donors with known hypertension [20].
Hypertension
Anti-hypertensive drugs are typically not required after brain death due to the transient nature of the autonomic storm [36]. Hypertension is very unlikely to occur after brain death, and as donor organs tend to be at higher risk of hypotension rather than hypertension, a conservative treatment plan is recommended [14]. In the case of a hypertensive donor, the goal for mean arterial BP is <90 mmHg, but it should always be kept above 65–70 mmHg [14]. If necessary, short-acting anti-hypertensive drugs, such as esmolol, sodium nitroprusside, hydralazine, labetalol, or nitroglycerine, are preferred as long-term use of anti-hypertensive drugs are usually not required [36].
Hypotension
Systemic hypotension is very common in brain-dead donors and may occur in up to 97% of cases [46]. Signs of continuing hemorrhage (external, gastrointestinal, urinary, abdominal, etc.) should be checked, and medications that may contribute towards hypotension (e.g., anti-hypertensive drugs, β-blockers) should be avoided [36]. Three management strategies are commonly adopted, and the direction of treatment depends on the clinical response. These strategies include volume expansion, vasopressors and inotropes, and hormonal replacement as described below [5].
Volume expansion and fluid management
Hypovolemia is a common scenario in brain-dead donors and appropriate fluid resuscitation is usually considered the first step in correcting hypotension [28]. There is debate on the selection of fluid, with no consensus on which type of fluid is more appropriate. At different centers, both crystalloids and colloids are used and often in combination [28]. However, the decision for fluid selection should be considered based on serum electrolytes, sugar levels, hemodynamics of the patient, estimated volume deficiency, and polyuria from DI [36].
(1) Fluid
The recommendations are as follows [5,36]. (1) Crystalloids with balanced salt content should be used to avoid hypernatremia (concurrent DI). Lactated Ringer’s solution and halfnormal saline (0.45%) are frequently used [36]. A solution of 0.9% normal saline may cause hyperchloremic acidosis, which increases renal vascular resistance and confounds base excess when used as a resuscitation fluid. Excessive IV fluids containing 5% dextrose may worsen hyperglycemia and hypothermia [36]. (2) Colloids, such as hydroxyethyl starches, need to be avoided in organ donors as they can damage renal epithelial cells and cause early graft dysfunction in the transplanted kidneys [36]. (3) Albumin solutions (4% and 20%) can be used to reduce the amount of fluid volume administered. However, it is usually only moderately effective, and the high sodium content of albumin-based solutions should also be considered [36]. (4) Lactated Ringer’s solution or half-normal saline solution (0.45%), with the addition of sodium bicarbonate at 50 mmol/L, can be given if the donor has acidosis to reduce the incidence of hypernatremia (i.e., sodium levels ≥150 mmol/L) in donors [5].
(2) Monitoring
Hemodynamic monitoring tools are used in the assessment of volume status and responses to therapy [12]. Pulmonary artery or central venous catheter insertion, as well as noninvasive monitoring techniques, should be considered. Serial or continuous measurements of central venous pressure or pulmonary arterial obstructive pressure are necessary. Stroke volume, CO, cardiac index, and mixed venous oxygen saturation should also be monitored continuously [12].
Vasoactive agents
Patients require additional vasoactive agents when adequate fluid resuscitation is not sufficient to restore BP and CO. It has been estimated that approximately 80%–90% of donors require inotropic and/or vasopressor support [47]. There are widely divergent opinions concerning the use of vasoactive medication, with no consensus or randomized controlled trials (RCTs) to determine which drugs to use and which to avoid [28]. Depending on local practices and protocols, noradrenaline, adrenaline, vasopressin, dopamine, and/or dobutamine are commonly used solely or in combination. Animal models have shown that high doses of catecholamines may cause cardiomyopathy [48]. Although no RCTs in humans currently exist, animal models have demonstrated a reduced inflammatory response and improved oxygenation when using noradrenaline [49].
Very few retrospective studies currently exist examining the selection of catecholamines for use in organ-protective intensive care [50-52]. In Germany, norepinephrine is most often used to target parameters at low dosages, whereas in the Anglo-American arena, vasopressin is often preferred over norepinephrine. The recommended dose of noradrenaline is 0.5–4 U/hr [50-52]. In some centers, if the CO is lowered, dobutamine is also used.
Vasopressin is highly effective in DI management and reduces the hemodynamic need for using different catecholamines [53,54]. However, other studies have shown that norepinephrine increased both coronary and renal blood flow in the normal mammalian circulation [55], whereas vasopressin had no effect [56]. At present, there are no convincing studies or consensus to demonstrate that one vasopressor is superior to another [28].
Although dopamine is used frequently by some centers, other transplant teams prefer not to use it as dopamine causes presynaptic modulation of norepinephrine release. Therefore, prolonged dopamine infusions may cause depletion of norepinephrine stores in the heart, possibly resulting in myocardial dysfunction after transplantation [57,58]. Some studies have found that combining 1-deamino-8-D-arginine vasopressin with a low dose of epinephrine may produce prolonged hemodynamic stability in brain-dead patients without causing worsening of liver or renal functions [59], although such approaches are still considered experimental.
Combined hormonal therapy
Although “triple-therapy” (the combination methylprednisolone, vasopressin, and triiodothyronine [T3]) remains controversial, some studies have reported that it may improve both hemodynamic stability in brain-dead patients, as well as the quality of the procured organs [60]. Some centers use triple therapy according to their local protocol with the decision of initiating hormonal therapy undertaken in discussion with the organ retrieval teams [60].
The United Network for Organ Sharing has conducted an analysis on 10 years of data covering several hormone replacement modalities and showed that the combination of a thyroid hormone, corticosteroid, insulin, and an antidiuretic hormone was the most promising in multiple organ procurement [61]. Combined hormonal therapy is particularly indicated in patients in which volume loading and vasoactive medications have not produced hemodynamic instability [39]. Hormone replacement therapy may be initiated if hemodynamic goals are not met and/or the left ventricular ejection fraction remains less than 45% [12]. The recommended replacements are [2,5,14,36]: (1) vasopressin: 1 U bolus followed by an infusion of 0.5–4.0 U/hr, (2) methylprednisolone: 15 mg/kg immediately after the diagnosis of brain death and every 24 hours afterwards. Alternatively, 250 mg followed by 100 mg/hr until organ retrieval, (3) insulin infusion to maintain blood glucose levels between 80 and 150 mg, (4) thyroxine (T4; 20 μg bolus) followed by infusions of 10 μg/hr. T3, administered as a 4 μg bolus, followed by infusion of 3 μg/hr. T4 improves hemodynamic status and prevents cardiovascular collapse in hemodynamically unstable organ donors.
Arrhythmias
Atrial and ventricular arrhythmias, as well as conduction defects, occur frequently in brain-dead organ donors and are more commonly seen in cases with a longer lag between brain death and organ removal [36,62]. Additionally, electrolyte and arterial blood gas (ABG) disorders, hypotension with myocardial ischemia, hypothermia, inotropes infusion, myocardial contusions, and increased ICP are important contributing factors to the development of arrhythmias [40]. Special attention should be paid to treat arrhythmias promptly, as severe problems are associated with them.
Prevention of arrhythmia
To prevent and reduce the risk of developing cardiac arrhythmias, electrolytes, BP, fluid volume, and body temperature should all be carefully monitored and maintained within the normal range [36].
Treatment of tachyarrhythmia
Standard therapies, such as amiodarone or cardioversion, can be used to treat arrhythmias [36]. While atropine is not useful in the management of bradycardia, adrenaline, isoprenaline, or pacing, may be effective in such cases [63]. Ultimately, all brain-dead individuals undergo terminal arrhythmias that are resistant to therapy [62]. In such cases, cardiopulmonary resuscitation should be performed for at least a limited period and especially if the donor is already in the operating room [40].
Respiratory Management
Currently, there are a limited number of RCTs examining optimal management strategies for respiratory function in braindead donors [28]. An RCT involving 118 potential donors reported that lung protective ventilation (i.e., lowest possible plateau pressure, tidal volumes of 6 ml/kg of ideal body weight, and moderate positive end expiratory pressure [PEEP] of 5–10 cmH2O to achieve an oxygen saturation of >92%) doubled the lung transplant rate from 27% to 54% [64].
In the majority of circumstances, volume-limited controlled mechanical ventilation is typically used during organ donor care. The goals of mechanical ventilation include maintaining [14]: (1) peak airway pressure: <40 cmH2O, (2) plateau airway pressure: <35 cmH2O, (3) fraction of inspired oxygen (FiO2): lowest possible to maintain peripheral arterial oxygen saturation (SpO2) >92% and PaO2 >70 mmHg, (4) PEEP: minimum 5 cmH2O, adjust to maintain PaO2 >70 mmHg, (5) auto-PEEP <5 cmH2O, (6) ABG values: pH 7.35–7.45; arterial partial pressure of carbon dioxide (PaCO2) >16 mmHg, <60 mmHg to maintain pH within goal range; PaO2 >70 mmHg; HCO3 not independently adjusted.
The respiratory passage must be kept clear of any obstruction with routine measures, such as suctioning, positioning, and turning, continued to achieve this [36]. Although atelectasis and excessive fluid resuscitation are two major causes of hypoxemia that often preclude the use of lungs in transplantation, these factors can be corrected [5]. Recently, it has been recognized that lung injury and inflammation may occur due to the use of prolonged mechanical ventilation. It has been suggested that the strategies for alveolar recruitment to treat atelectasis should be applied judiciously, with the end inspiratory plateau pressure limited to less than 30 cmH2O [5]. Strategies (e.g., PEEP to maintain oxygen delivery to the organs due to reduction in atelectasis, avoidance of interstitial fluid overload, and maintenance of oxygen saturations within normal limits) should be undertaken and normocapnia should be maintained [36].
Endocrine Management
Thyroid hormone replacement
Positive effects on the routine administration of thyroid hormones as a part of the brain-dead organ donor management protocol have not been reported in many studies [65,66]. This has created considerable debate within the transplant field. Animal studies have demonstrated that deterioration in cardiac function could be reversed with T3 supplementation [67,68], although no such correlation was found in human studies [45,66,69].
Although T3 levels decrease in roughly 75% of patients, very few brain-dead donor patients actually reach significantly low T3 levels, while free T4, conversely, seems to be less affected with only one-third presenting subnormal values [20]. Actually, abnormal thyroid function values seen after brain death are more consistent with “sick euthyroid syndrome” rather than true hypothyroidism [45,66]. Thus, routine replacement of thyroid hormones is not recommended for all organ donors [20]. Some guidelines suggest thyroid hormone supplementation only if impaired cardiac performance is documented despite overall good general management [70,71]. Thyroid hormone supplementation may be safe if over dosing is avoided [72,73]. Perhaps only patients with true hypothyroidism will actually benefit from thyroid hormone replacement since not all brain-dead donors exhibit a total absence of anterior pituitary gland function [12].
Corticosteroids
High doses of corticosteroids may reduce brain death-induced inflammation and help to modulate immune function, thereby improving donor organ quality and post-transplant graft function [12]. Therefore, treating brain-dead donors with corticosteroids is often recommended [5,74]. The main purpose of using corticosteroids is not to treat adrenocortical failure, but rather to attenuate the immune responses and reduce the catecholamine requirement for maintaining BP [20].
The use of methylprednisolone in brain-dead donors leads to improved short- and long-term outcomes for most transplanted organs [28], along with improved oxygenation, reduction of extravascular lung water [23], and increased lung yield. It also reduces inflammation in the liver [75], heart [76], and kidney [77]. Administration of methylprednisolone to the organ donor reduces inflammation in the kidney after transplantation [77]; however, there is no evidence of reduction of the incidence or duration of primary graft failure. Methylprednisolone should be administered as soon as possible as its use is associated with increased organ retrieval [78].
Insulin
Major hormonal alterations caused by brain death may result in insulin resistance and gluconeogenesis. Moreover, the practice of administering solutions containing dextrose and the use of corticosteroids may further worsen glucose homeostasis [12]. Hyperglycemia is closely associated with reduced host immune responses that result in an increased risk of infection, worsening of renal function in renal transplant recipients, as well as osmotic diuresis [20]. A retrospective study on deceased organ donors showed that higher glucose levels with greater fluctuating levels were associated with reduced pre-recovery of renal function [33].
It is generally accepted that uncontrolled hyperglycemia should be treated and deceased hyperglycemic organ donors should be treated as other critically ill patients. However, there still remains considerable debate regarding target glucose levels for intensive insulin therapy in critically ill patients [12]. Hyperglycemic organ donor patients should be treated according to the local institutional guidelines used for other critically ill patients. Routine use of IV fluids containing dextrose should be avoided [12].
Anti-diuretic hormone
If the patient develops DI, electrolytes should be monitored frequently and corrected accordingly [20]. If left untreated, this may result in hypovolemia, hyperosmolality, hypernatremia, hypermagnesemia, hypokalemia, hypophosphatemia, and hypocalcemia [40]. IV fluids should be given to replace fluid loss through urine and a balanced salt solution or fluids with low-sodium content (5% dextrose or 0.45% saline) should be used to maintain sodium levels between 135 and 145 mEq/L [36].
Treatment for arginine vasopressor or antidiuretic hormone deficiency should be considered if hypotension persists despite adequate volume resuscitation and if one or more of the following criteria are identified in the absence of other causes [12]: polyuria (urine output >3–4 L/day or 2.5–3.0 ml/kg/hr), normal or increased serum osmolality, (3) inappropriately diluted urine (specific gravity <1.005, urine osmolality <200 mOsm/kg H2O), (4) hypernatremia (Na+ >145 mmol/L). DI can be treated by replacement of fluid with adequate crystalloid solutions and by administration of desmopressin. Vasopressin can also be used as an alternative to desmopressin [2,46].
Renal Management
As shown in experimental animal models and historical databases, kidneys are at high risk for developing ischemia because of increased levels of catecholamines at the time of brain death. Subsequent hypoperfusion is also possible if donor management is inadequate and is not appropriately treated [3]. Effective donor management is associated with good renal graft function, even if liberal fluid therapy is avoided [2]. Renal management should be achieved by appropriate fluid management and judicial use of vasopressor drugs.
Hematological Management
Anemia
The most likely causes of anemia during donor care management are continued blood loss or excessive blood draws performed for laboratory testing, with hemolysis very unlikely to occur [14]. The target is to maintain the hematocrit (Hct) above 30%. If the Hct drops below 30%, two units of packed red blood cells (PRBCs) should be transfused rapidly. Hct levels should be reassessed 1 hour after every PRBC infusion, with repeated transfusions necessary if Hct levels remain below 30% [14].
Coagulopathy
Coagulopathy should be treated promptly with management including the administration of red blood cells, clotting factors, and platelets [40]. However, the transfusion of blood or blood products should be given only when necessary [36]. In certain cases, the onset of severe coagulopathy may necessitate the rapid transfer of the donor from the ICU to the operating room for organ retrieval [40].
Infectious Disease Protection
The diagnosis of sepsis may be difficult in brain death as elevated leukocyte count and tachycardia are non-specific for infectious processes. Additionally, fever may not be clinically evident in some patients due to hypothalamic dysfunction [20]. The principles of antimicrobial therapy are similar to other critical non-organ donor patients. Antimicrobial therapy should be given based on the results of gram staining or cultures; empirical therapy can be started if recommended by the transplant team to treat suspected pathogens causing infection [39]. Nephrotoxic antimicrobials should be avoided if possible and the use of prophylactic antimicrobials are not routinely recommended [39]. Preventive measures include maintaining pulmonary hygiene with regular tracheal suctioning and oral care, keeping the head of the bed elevated, as well as aseptic management of invasive lines or catheters that should be removed as soon as they are no longer needed [20].
Management of Nutrition
Nutrition should be continued based on standard ICU protocols in patients waiting for consent for organ donation from family members [79]. Continuing enteral feeding to maintain adequate nutrition in potential donors may help to provide beneficial effects on organ functioning [80].
PROPOSAL OF PROTOCOLS FOR ORGAN DONOR MANAGEMENT
In this review, we have thoroughly mentioned and identified the physiological effects of irreversible total loss of brain function in brain death. We have also mentioned the practical aspects of brain-death management and the care of potential organ donors. We have reviewed in detail different guidelines and protocols used in brain-dead donor management and found that each transplant center follows their own protocol.
Although there is considerable variation in treatment protocols for different centers with no authentic guidelines in the management of potential brain-dead organ donors, herein, we propose a guideline for consideration. Our proposed treatment protocol, based primarily on the Korea University Anam Hospital (Seoul, Korea) management protocol for brain-dead organ donors, has been prepared for centers or countries, such as Bangladesh, where no management guidelines are currently available. Our proposed guideline (shown below) will help other centers to prepare their own management protocols for proper management of potential organ donors. This will increase chances of successful transplantations in the future.
Protocol for the Management of Brain-Dead Organ Donors
Main protocols are summarized in Table 3. The oxygen challenge test is a major criterion for lung donor selection. The ratio of PaO2/FiO2 is recorded to determine the predictive variables of the donor lung PaO2/FiO2 ratio [81]. Good oxygenation is considered a good indicator for determining the functional quality of the lung [82]. During the oxygen test, lung compliance is tested under direct vision by disconnecting the endotracheal tube from the ventilator; if the lungs remain inflated or only slowly collapse, this indicates interstitial fluid accumulation, pneumonia, or small airway obstructive disease (emphysema), or major airway plugging. After removing all atelectatic zones by squeezing, the lungs will gently reinflate. A blood gas sample is then drawn from the left and right pulmonary veins to reassess the oxygenation capacity of both lungs separately [82].
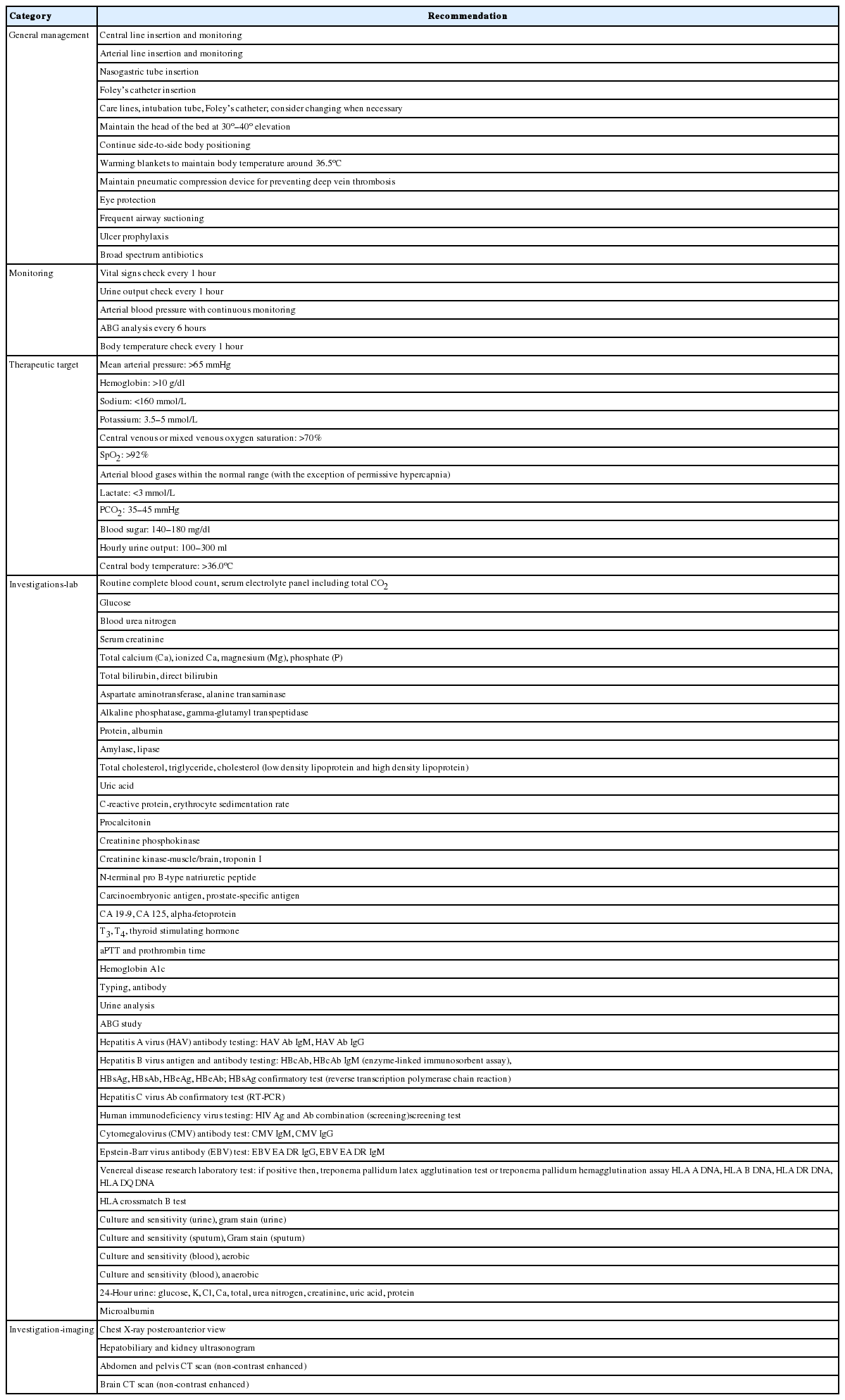
Protocols for the management of brain-dead organ donors
Although most studies demonstrate that the results of the oxygen challenge test predict the outcome of lung transplantations, in other studies, it is considered a categorical variable. Some studies suggest different cutoff points for the oxygen challenge test [81]. For example, based on the international criteria for lung donation, an oxygen challenge test with a result <400 mmHg is usually considered ideal and a result <200 mmHg as not acceptable [81]. It is recommended that the donor PaO2 should be <300 mmHg. If the result of the donor oxygen test is <300 mmHg after transplantation, pulmonary function may have deteriorated [83]. Donors with suboptimal oxygen challenge test results should not be excluded immediately, however. Instead, more aggressive donor management strategies should be undertaken to decrease the percentage of unusable donor lungs and to maximize transplantation opportunities [81].
Medication protocols for brain-dead organ donors are summarized in Table 4.
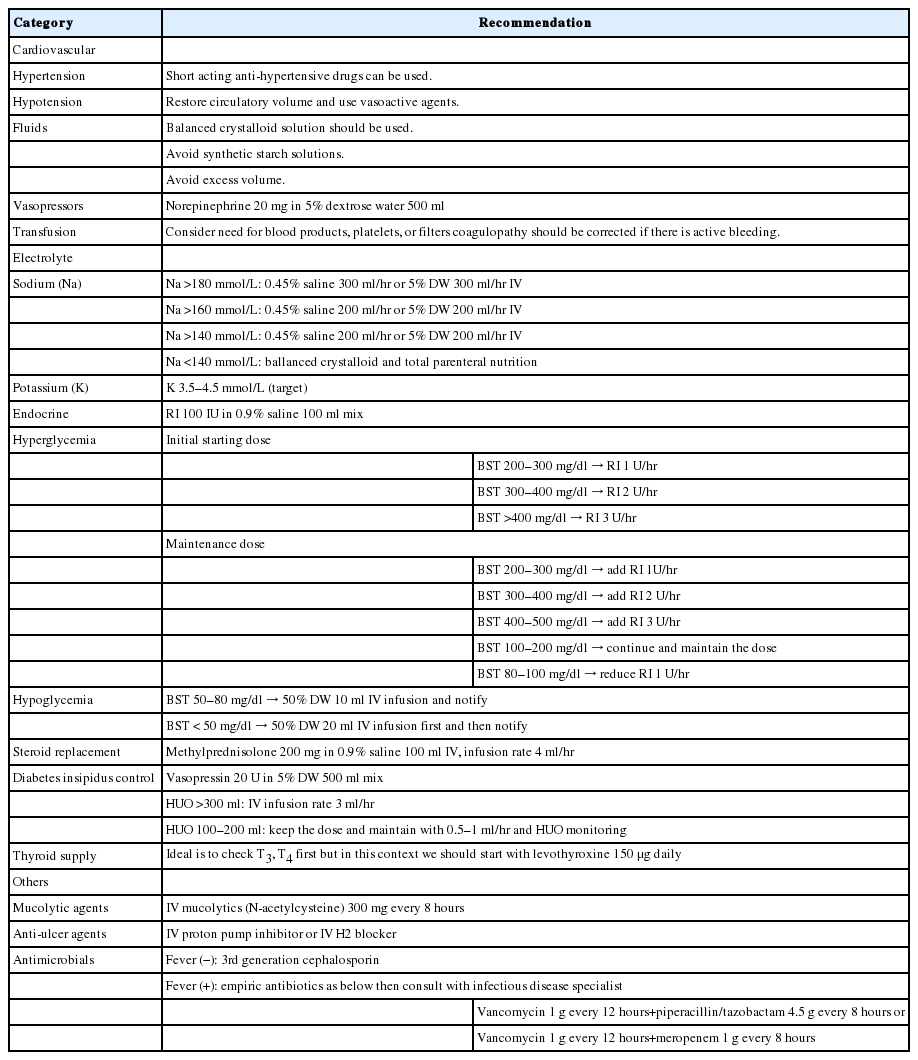
Medication protocols for brain-dead organ donors
CONCLUSIONS
As brain stem death leads to an expected pattern of complex multiple organ failure, appropriate management and adequate care of the potential organ donor before and after brain death can increase the number and quality of donor organs [36]. The management of a brain-dead organ donor is very challenging. To achieve this goal, adequate fluid resuscitation, intense vasoactive medication, immunosuppressive therapy, and sufficient hemodynamic, and physiological monitoring are required [28]. The current protocols are based on expert opinions, and mostly recommend extended hemodynamic monitoring, early-differentiated volume, and vasopressor or catecholamine therapy [13]. The protocol we have proposed and provided in the checklist may help intensivists manage brain-dead organ donors to promote successful organ and tissue donations.
KEY MESSAGES
▪ Intensivists need to play a vital role in the management of potential organ donors through identification of potential donors, declaration of brain death, and proper medical care, all of which can improve the rates of graft survival.
▪ The protocol we have proposed and provided in the checklist may help intensivists in managing brain-dead organ donors to promote successful organ and tissue donation.
Notes
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
Acknowledgements
First of all, I express my ever gratitude to almighty Allah who has given me the enough strength, spirit, and fortitude to carry out this laborious job. With upmost regards, I owe my heartiest gratitude and indebtedness to my honorable teacher and guide Dr. Jae Myeong Lee (Assistant Professor of Department of Acute Care Surgery, Korea University Anam Hospital, Seoul, Korea) who is the corresponding author of this article, for her constant courage, close supervision and scholarly support throughout this work. I also give thanks to Korea University Anam Hospital authority to give me the opportunity of working in this hospital and provide all the supports to complete this research work successfully. I owe a deep debt gratitude to Dr. Harun Ur Rashid, Professor and Chairman of the Kidney Foundation, Dhaka, Bangladesh, who arranged my fellowship training on brain-dead donor management in Korea University Anam Hospital, Seoul, Korea and I am also grateful to Dr. Md. Nizamuddin Chowdhury, Professor and Head, Department of Nephrology, Dhaka Medical College Hospital, for his encouragement, invaluable skillful advice and suggestion which have been instrumental for me throughout the period of this work. I am indebted to my parents and family members for their sacrifice, wholehearted support, and continuous inspiration.
Notes
AUTHOR CONTRIBUTIONS
Conceptualization: JML. Project administration: all. Visualization: JML. Writing - original draft: all. Writing - review & editing: all.