Feasibility of Immediate in-Intensive Care Unit Pulmonary Rehabilitation after Lung Transplantation: A Single Center Experience
Article information

Abstract
Background
Physical function may influence perioperative outcomes of lung transplantation. We investigated the feasibility of a pulmonary rehabilitation program initiated in the immediate postoperative period at an intensive care unit (ICU) for patients who underwent lung transplantation.
Methods
We retrospectively evaluated 22 patients who received pulmonary rehabilitation initiated in the ICU within 2 weeks after lung transplantation at our institution from March 2015 to February 2016. Levels of physical function were graded at the start of pulmonary rehabilitation and then weekly throughout rehabilitation according to criteria from our institutional pulmonary rehabilitation program: grade 1, bedside (G1); grade 2, dangling (G2); grade 3, standing (G3); and grade IV, gait (G4).
Results
The median age of patients was 53 years (range, 25 to 73 years). Fourteen patients (64%) were males. The initial level of physical function was G1 in nine patients, G2 in seven patients, G3 in four patients, and G4 in two patients. Patients started pulmonary rehabilitation at a median of 7.5 days (range, 1 to 29 days) after lung transplantation. We did not observe any rehabilitation-related complications during follow-up. The final level of physical function was G1 in six patients, G3 in two patients, and G4 in 14 patients. Fourteen of the 22 patients were able to walk with or without assistance, and 13 of them maintained G4 until discharge; the eight remaining patients never achieved G4.
Conclusions
Our results suggest the feasibility of early pulmonary rehabilitation initiated in the ICU within a few days after lung transplantation.
INTRODUCTION
Lung transplantation (LTx) has become the standard of care as a lifesaving procedure for carefully selected patients suffering from end-stage lung disease refractory to other treatments [1]. However, a growing body of literature has indicated that patients who have survived LTx commonly have significant and prolonged neuromuscular complications that impair their physical function [2,3] and quality of life [4] after hospital discharge. Moreover, a modest decrease in mortality after LTx [5] and technical advancements, such as bridging strategies, have allowed older and more debilitated patients with end-stage lung disease to be considered as LTx candidates, although a more complicated clinical course can be expected for these patients [6-8].
Rehabilitation is an important component in the care of patients after LTx [9], but there are currently no standard guidelines focused on rehabilitation in LTx [10]. In addition, the efficiency of pulmonary rehabilitation (PR) with a conventional start of exercise upon weaning of sedation or mechanical ventilation outside the intensive care unit (ICU) has been well described in LTx patients [11,12], but there is a paucity of data regarding PR initiated in the ICU as early as possible for patients post-LTx. Physical function has been suggested to influence perioperative outcomes after LTx [13,14]. Immobility plays a crucial role in the development of neuromuscular weakness, which can influence the performance of activities of daily living and the return to social activities in ICU survivors [15]. This study aimed to demonstrate the feasibility of early PR initiated in the ICU for patients who had undergone LTx by analyzing the early transplantation outcomes.
MATERIALS AND METHODS
Study Design and Patients
Data were retrospectively extracted from a prospectively-collected center registry of LTx patients and electronic medical records from the ICU. Consecutive patients who underwent LTx between March 2015 and February 2016 were assessed for inclusion in this study. Among these patients, those who received early PR initiated in the ICU according to our institutional eligibility criteria (Figure 1) were selected for this study. Patients were excluded if PR was initiated 2 weeks after admission to the ICU post-transplant. The usual procedures for LTx have been described previously [16]. All patients were admitted to the ICU from the operation room. This study was approved by the Institutional Review Board of Severance Hospital of Yonsei University College of Medicine, with a waiver of individual consent due to the retrospective study design (IRB No. 4-2013-0770).

Assessment of eligibility for pulmonary rehabilitation. ICU: intensive care unit; RASS: Richmond Agitation-Sedation Scale; FiO2: fraction of inspired oxygen; PEEP: positive end-expiratory pressure; SpO2: peripheral oxygen saturation; MAP: mean arterial pressure; DVT: deep vein thrombosis; INR: international normalized ratio.
Pulmonary Rehabilitation Program
In 2015, a structured rehabilitation program was developed at our center, with a focus on improving rehabilitation and facilitating mobility. The program was designed to be initiated within the ICU for patients with the following conditions or treatments: (1) LTx recipients; (2) prolonged mechanical ventilator use after surgery; (3) prolonged mechanical ventilator use in chronic obstructive pulmonary disease; and (4) prolonged mechanical ventilator-dependent chronic respiratory failure. The PR was developed by a core rehabilitation team, consisting of a pulmonary/critical care physician, specialist nurse, and physical therapist. On admission to the ICU after LTx, all recipients received physiotherapy provided by the ICU nursing staff at least once daily from day 1 post-transplant. Physiotherapy was individually tailored but primarily included frequent chest percussion and range of motion (ROM) of the upper and lower extremities lasting 5 to 10 minutes, and a position change every 4 hours. In addition, as soon as LTx recipients were considered able to receive PR, initial assessment of the functional grade for mobilization capacity and subsequent establishment of a rehabilitation plan were conducted by a specialized physical therapist. A qualitative assessment of the use of steroids or neuromuscular agents was made for each patient.
Our PR protocol involved four levels of mobilizing therapy, consisting of 60 minutes of exercise each day, 5 days a week. The functional grade of mobilizing capacity was recorded weekly until PR was over, as illustrated in Figure 2, and the corresponding level of PR was delivered by an attending specialized therapist. In brief, subjects of grade 1 were confined to bed and received bedside physical therapy, including passive ROM, active-assistive ROM, active ROM, resistance exercise, sitting exercise leaning against the backrest, and bed cycling. Subjects who were able to sit on the edge of the bed (grade 2) received dynamic sitting balance training. The ability to stand with one’s knees supported by others (Bobath standing) or to stand with a walker at the bedside was grade 3. Advancement to the final grade was based on the ability to walk (grade 4, gait group).

Pulmonary rehabilitation program based on the functional grade. ROM: range of motion; tid: ter in die, three times a day; PTx: physical therapy.
Statistical Analysis
Continuous variables were analyzed with Mann-Whitney Utests and summarized as median and interquartile range. Categorical data were analyzed with Fisher exact tests or Pearson chi-square tests, depending on the distribution, and were summarized as absolute frequencies and percentages. All analyses were performed with the SPSS version 16.0 software (SPSS Inc., Chicago, IL, USA).
RESULTS
Patient Characteristics Prior to PR in the ICU
During the study period, 26 patients had LTx and PR after ICU admission. Of these 26 patients, 22 were eligible for the study: they had PR sessions of at least 7 days that began in the ICU within 4 weeks after transplant. Patient demographics and preoperative status are summarized in Table 1. The median age of the 22 patients was 53 years (range, 25 to 73 years), and 14 (64%) patients were males. Indications for LTx were idiopathic pulmonary fibrosis (n=12), collagen vascular disease interstitial lung disease (n=1), chronic pulmonary obstructive disease (n=1), bronchiectasis (n=2), bronchiolitis obliterans syndrome after allogeneic stem cell transplantation (n=3), acute interstitial pneumonitis (n=2), and primary pulmonary hypertension (n=1). Emergency status as assessed by the Korean Lung Allocation Score [17] is summarized in Table 1. Preoperative extracorporeal membrane oxygenation (ECMO) support was used in seven patients (32%). The median ischemic time was 282 minutes (range, 185 to 325 minutes), and all patients received bilateral LTx using ECMO for intraoperative cardiopulmonary support. All patients were intubated and transferred to the ICU after LTx; 12 (55%) were weaned off of ECMO in the operating room.
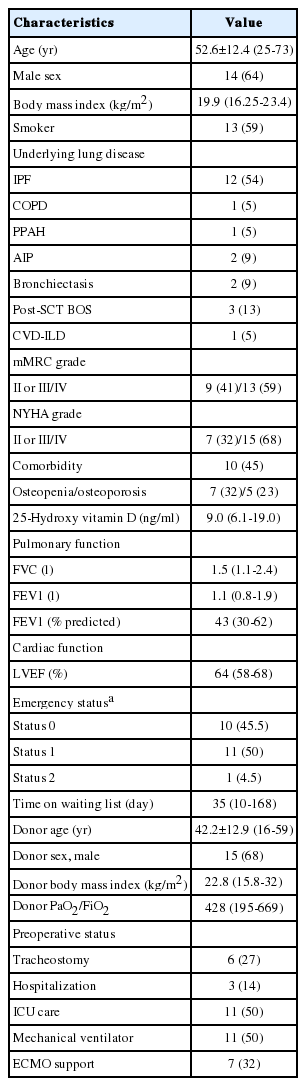
Pretransplant baseline characteristics
Physical Function Assessed by Mobilizing Capacity
Eight patients (36%) had received rehabilitation prior to LTx with a median of 26 days (range, 2 to 100 days). Of the eight patients who had preoperative PR, three had received hematopoietic stem cell transplantation. All 22 patients started PR at a median of 7.5 days (range, 1 to 29 days) after LTx (Table 2). We did not observe any rehabilitation-related complications during follow-up. Median time from weaning of intraoperative ECMO support and PR initiation was 6 days (range, 1 to 21 days). Thirteen patients (59%) were on mechanical ventilator support when PR was initiated with a median of 11.5 days (range, 2 to 43 days), while eight patients were on tracheostomy status. Neuromuscular disorder was observed in six patients. At the time of PR, the initial functional grade of mobilizing capacity according to our institutional grading system (Figure 2) was grade 1 in nine patients, grade 2 in seven patients, grade 3 in four patients, and grade 4 in two patients (Table 2). Patients received a median of 6.5 weeks (range, 1 to 36 weeks) of rehabilitation before hospital discharge or cessation for safety reasons. At the end of PR, the functional grade was grade 1 in six patients, grade 3 in two patients, and grade 4 in 14 patients. Fourteen of the 22 patients were able to walk with or without assistance, and 13 of them maintained grade 4 until discharge; the eight remaining patients never achieved grade 4. In comparison to those who failed to achieve and maintain grade 4, patients with grade 4 had significantly lower scores on the modified Medical Research Council dyspnea scale (P=0.074) and the New York Heart Association functional class (P=0.022). These patients also had a significantly shorter median duration of propofol (8 days vs. 14 days, P=0.02) and remifentanyl (16 days vs. 23 days, P=0.004) infusions during immediate postoperative management. The use of other drugs, such as high dose steroids, used within 1 month prior to PR, muscle relaxants, or midazolam, did not differ between grade 4 patients and patients of lower grades. Other pretransplant clinical characteristics also did not differ between these groups.
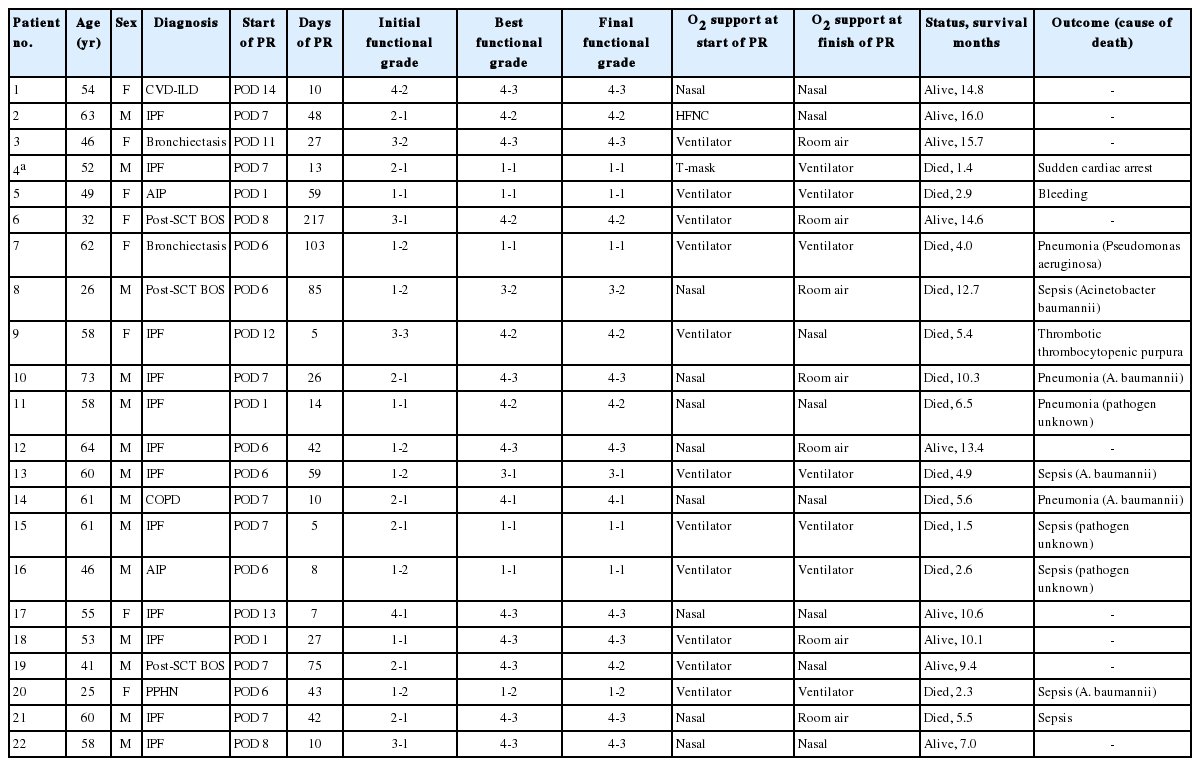
Change of functional grade of mobilizing capacity and survival outcomes
Clinical Outcomes of Lung Transplantation
Median duration of postoperative ECMO support was 2 days (range, 1 to 9 days); median duration of postoperative mechanical ventilation was 13 days (range, 3 to 149 days). Six patients received second ECMO support due to bleeding (n=3), pneumonia (n=2), or cardiac arrest (n=1). The median ICU stay was 13 days (range, 3 to 149 days), and the median hospital stay was 43 days (13 to 221 days). The ICU stay was shorter in grade 4 patients (6.5 days) than in patients of lower functional grades (32.5 days, P<0.001). Likewise, the hospital stay was shorter in grade 4 patients (50.0 days) than in patients of lower functional grades (102.5 days, P=0.035). Within 6 months from LTx, there were 10 cases of mortality, and after a median follow-up of 13.4 months (range, 7.0 to 16.0 months) after LTx, 13 patients (59%) had died (Table 2). Infection (77%) was the most common cause of death in our cohort.
DISCUSSION
After LTx, the recipient’s physical capacity can be affected by prolonged hospitalization with an ICU stay, postoperative complications, and use of immunosuppressants [18]. Consequently, many patients receiving LTx suffer from substantial muscle dysfunction, reduced physical capacity, and a decline in health-related quality of life [19,20]. In an attempt to improve the mobilizing capacity of LTx recipients as early as possible, we assessed LTx recipients using our institutional selection criteria for an in-ICU rehabilitation program within 48 hours to 72 hours postoperatively. The findings of this small case series suggest that in-ICU PR as early as possible postoperatively is feasible and safe for patients who undergo LTx, as no relevant complications related to PR were observed.
Several previous trials have suggested that rehabilitation should begin as early as possible postoperatively and should prioritize upright positioning and gait exercises in critically ill patients with acute respiratory failure, often with prolonged mechanical ventilation support, or in patients during the postoperative period [21,22]. Patients with in-ICU achievement of grade 4 mobility (gait) spent less time in the ICU and in the hospital and had improved survival. However, these findings should be interpreted with caution because measures that employ standard clinical tests, such as the ICU mobility scale or functional status score for the ICU, were not available for this study. Neuromuscular weakness is common in critically ill patients and is highly correlated with increased duration of mechanical ventilation, increased length of stay in the ICU, and increased in-hospital mortality for critically ill patients [23-25]. Therefore, it is possible that the patients with less complicated pre- and post-transplant clinical courses and, consequently, less neuromuscular weakness, also had better walking ability. The most common cause for mortality in our study was infection. Objective measurements of early mobilizing ability to evaluate its effect on post-transplant infectious complications would be useful to demonstrate the efficacy of early PR after LTx and to improve post-transplantation survival outcomes.
Use of immunosuppressants and a prolonged hospital course in LTx patients can contribute to delayed recovery of quadriceps strength [26]. Moreover, as shown in our study results, prolonged use of sedatives can be associated with weakness and low physical capacity although there remains substantial controversy regarding this association [23].
Previous reports of rehabilitation for LTx recipients demonstrated the efficacy of postoperative rehabilitation using an outpatient program that began after the recipients were discharged from the hospital. A randomized controlled trial by Fuller et al. [27] demonstrated that rehabilitation programs of either 7 weeks or 14 weeks were both beneficial in terms of functional exercise capacity, lower limb strength, and quality of life at 6 months after LTx. Because our patients received PR initiated in the ICU before they were healthy enough for discharge, interruption of the rehabilitation program was somewhat frequently observed, depending on how complicated the post-transplant course and deconditioning was, although the interruption was not significantly associated with achievement of gait (data not shown). In fact, no prior studies have focused on the rehabilitation of patients before discharge in the early postoperative period [10,28]. As the demographics of transplant candidates has shifted from young and fit patients to elderly adults with comorbidities and frailty, development of an early rehabilitation program suitable for these patients should be further explored.
This pilot study had some limitations. First, our sample size was small, and the data are from a single center. Second, the retrospective nature of the study meant we could not draw conclusions about the causal effect of early PR within the ICU on transplantation outcomes. Finally, the level of physical activity could not be assessed by measurements that had been validated in ICU patients specifically [10]. Physical activity is usually measured by time spent walking (6-minute walking test) or doing activities of daily living. However, these measurements are not appropriate for assessing the level of physical activity of critically ill patients receiving treatment in the ICU. Further evaluation of the utility of our in-ICU rehabilitation program for immediate postoperative LTx patients should include measurement tools of physical function to demonstrate the causal effect on transplantation outcomes.
In conclusion, our results suggest the feasibility of early PR initiated in the ICU within a few days after LTx. Although future prospective studies will be needed to verify the effectiveness of our early in-ICU PR program and the superior posttransplant outcomes of patients who could walk, our results underline the potential importance of early PR specific to LTx patients.
KEY MESSAGES
▪ Rehabilitation is an important component in the care of patients after lung transplantation (LTx).
▪ This study aimed to demonstrate the feasibility of early pulmonary rehabilitation initiated in the intensive care unit for patients who had undergone LTx by analyzing the early transplantation outcomes.
Notes
No potential conflict of interest relevant to this article was reported.