Timing and Associated Factors for Sepsis-3 in Severe Trauma Patients: A 3-Year Single Trauma Center Experience
Article information

Abstract
Background
We hypothesized that the recent change of sepsis definition by sepsis-3 would facilitate the measurement of timing of sepsis for trauma patients presenting with initial systemic inflammatory response syndrome. Moreover, we investigated factors associated with sepsis according to the sepsis-3 definition.
Methods
Trauma patients in a single level I trauma center were retrospectively reviewed from January 2014 to December 2016. Exclusion criteria were younger than 18 years, Injury Severity Score (ISS) <15, length of stay <8 days, transferred from other hospitals, uncertain trauma history, and incomplete medical records. A binary logistic regression test was used to identify the risk factors for sepsis-3.
Results
A total of 3,869 patients were considered and, after a process of exclusion, 422 patients were reviewed. Fifty patients (11.85%) were diagnosed with sepsis. The sepsis group presented with higher mortality (14 [28.0%] vs. 17 [4.6%], P<0.001) and longer intensive care unit stay (23 days [range, 11 to 35 days] vs. 3 days [range, 1 to 9 days], P<0.001). Multivariate analysis demonstrated that, in men, high lactate level and red blood cell transfusion within 24 hours were risk factors for sepsis. The median timing of sepsis-3 was at 8 hospital days and 4 postoperative days. The most common focus was the respiratory system.
Conclusions
Sepsis defined by sepsis-3 remains a critical issue in severe trauma patients. Male patients with higher ISS, lactate level, and red blood cell transfusion should be cared for with caution. Reassessment of sepsis should be considered at day 8 of hospital stay or day 4 postoperatively.
INTRODUCTION
Trauma deaths typically occur within 48 hours of traumatic events, but the occurrence of sepsis is a major concern in trauma patients who have survived initial resuscitation [1]. Several published studies have identified risk factors for sepsis in trauma patients and have suggested that injury severity was the most common risk factor, although in rare cases, modifiable risk factors exist [2-4].
Sepsis-3 was recently defined as life-threatening organ dysfunction caused by a dysregulated host response to infection [5]. For this new definition, the Sequential Organ Failure Assessment (SOFA) score or quick SOFA (qSOFA) score was utilized [6]. Before the change in definition, systemic inflammatory response syndrome (SIRS) caused by infection was diagnosed as sepsis [7]. It was difficult to detect the timing of sepsis in trauma patients because severely injured patients usually presented with SIRS. However, it might be easier to detect sepsis using the sepsis-3 definition because severely injured patients are usually admitted to intensive care units (ICUs) for continuous monitoring with serial blood tests. The SOFA score and signs of infection are likely to be noticed during daily rounds. The purpose of the present study was to investigate the timing of the development of sepsis, defined by sepsis-3 criteria, and to identify the associated factors for sepsis occurrence in patients after severe trauma.
MATERIALS AND METHODS
Study Population
From January 2014 to December 2016, trauma patients in Ajou University Hospital Trauma Center were retrospectively reviewed. To identify severely injured patients, patients with Injury Severity Score (ISS) <15 were excluded. For monitoring of sepsis development, patients with a length of stay (LOS) <8 days were also excluded. Other exclusion criteria were as follows: under the age of 18 years, transferred from other hospitals, uncertain trauma history, and incomplete medical records (Figure 1). This study was performed according to the Helsinki Declaration and approved by the Institutional Review Board of Ajou Medical Center (IRB No. AJIRB-MED-MDB-17-464).
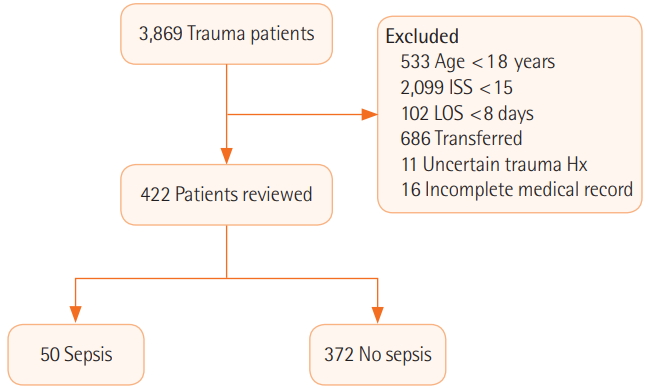
Flow diagram of patient enrollment. ISS: Injury Severity Score; LOS: length of stay; Hx: history.
Definitions
Sepsis-3 was defined as an increase of 2 or more points in the SOFA or qSOFA score due to infection. Infection was identified by image study, culture study, medical record, or opinion of an infection specialist. Sepsis-3 was monitored during total LOS in the hospital. Vital signs, Glasgow Coma Scale (GCS), and lactate level were measured when patients arrived at the hospital. Revised Trauma Score (RTS) was calculated based on GCS, systolic blood pressure, and respiratory rate. SIRS was defined based on initial vital signs and laboratory findings. Wounds were divided into four groups: abrasions, lacerations (subcutaneous deep), open wound (muscle-deep), or open wound (bone-deep). Antibiotics were considered to be any kind of antibiotics given in the emergency room.
Statistical Analysis
Continuous data were presented as median values and interquartile ranges, and categorical data were presented as frequencies and percentages. Comparisons were performed using the Mann-Whitney U-test for continuous variables and the chi-square analysis for categorical variables. Variables, selected after univariate analysis with P<0.10, were included in the multivariate analysis by applying binary logistic regression based on the forward selection (conditional) method, but overlapping variables were not selected. The results of the binary logistic analyses were summarized by estimating the odd ratio and the respective 95% confidence intervals. All analyses were performed using IBM SPSS version 21.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Patient Characteristics
A total of 3,869 patients were included, and after a process of exclusion, 422 patients were reviewed. Fifty patients (11.8%) were diagnosed with sepsis-3 and 372 patients were not. Demographic characteristics are shown in Table 1. The sepsis-3 group had a higher mortality rate (28.0% vs. 4.6%, P<0.001) and greater ICU LOS (23 days [range, 11 to 35 days] vs. 3 days [range, 1 to 9 days], P<0.001).
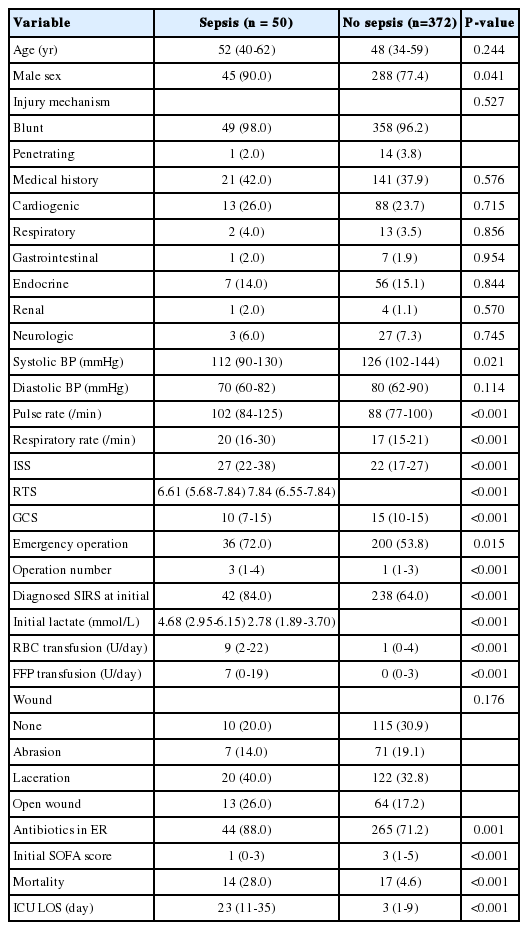
Demographics and clinical characteristics of severe trauma patients
Associated Factors for Sepsis-3
Sex, emergency operation, SIRS, antibiotics, GCS, ISS, transfusion, lactate, blood pressure, pulse rate, respiratory rate, and RTS were significantly different between the two groups. Sex, emergency operation, use of antibiotics, ISS, red blood cell (RBC) transfusion, lactate, and RTS were selected for multivariable analysis because vital signs, including SIRS and GCS, overlapped with RTS. After multivariable analysis, male sex, lactate, ISS, and RBC transfusion were selected as associated factors for sepsis-3 (Table 2).

Independent associated factors for sepsis after severe trauma
Timing and Focus of Sepsis
Among 50 patients in the sepsis group, no operation was performed in 10 patients. In all patients, the median timing of sepsis-3 was at 8 hospital days (range, 6 to 11 days). In patients who had undergone surgery, median timing of sepsis-3 was 4 postoperative days (range, 3 to 6 days) from the last surgery. The most common cause of sepsis involved the respiratory system (66.0%). One case presented with Escherichia coli in the blood, but the focus was not found. After antibiotic therapy without surgical debridement, the patient survived (Table 3).

Timing and focus of sepsis in severe trauma patients
DISCUSSION
Sepsis-3 was associated with poor prognoses in trauma patients, and male sex, lactate, ISS, and RBC transfusion were associated factors for sepsis-3 in the current study. Sepsis-3 occurred in 11.8% (n=50) of the study patients, and the inhospital mortality rate was 28.0% (n=14) for the sepsis-3 patients. Park et al. [8] demonstrated that the incidence of sepsis-2 was 8.2% and mortality was 6.7% in trauma patients (ISS >8) in the same country as our study. Sepsis-3 is more specific than the previous sepsis-2 definition because organ failure should be noticeable in sepsis [9]. Nevertheless, the incidence and mortality of sepsis-3 were higher in the current study because more severe patients (ISS ≥16) were included. Moreover, Shankar-Hari et al. [10] demonstrated that mortality with sepsis-3 in the ICU was 22.4%. Besen et al. [11] demonstrated that ICU mortality of patients with sepsis-3 was 25% and septic shock was 46% in low–middle-income countries, which were more severe than the mortality of patients with sepsis-2 (severe sepsis, 17%; septic shock, 44%). Although our study did not distinguish between septic shock and non-septic shock groups, mortality was similar in our study to that reported in these studies.
Kisat et al. [2] demonstrated that age, male sex, African-American race, hypotension, and motor vehicle crash were risk factors for sepsis in trauma patients. Osborn et al. [3] reported that ISS, RTS, admission GCS, and comorbid conditions (i.e., diabetes, cardiac disease, and immune disorder) were independent predictors of sepsis. Increased ISS was also significantly associated with the clinical outcome of sepsis patients. Wafaisade et al. [4] reported that male sex, ISS, operative procedure, RBC transfusion, GCS, and age were risk factors for sepsis. Similar to previous studies, male sex, lactate, ISS, and RBC transfusion were selected as associated factors for sepsis-3 in our study. Injury severity was correlated with immune system, and lactate level reflected the severity of trauma [12,13]. In large studies, male sex was associated with sepsis, which could be attributed to genetic or socioeconomic factors [14,15]. The ISS and male sex were common risk factors for sepsis that cannot be modified. However, RBC transfusion is modifiable if bleeding is controlled early. Therefore, early bleeding control might be considered to reduce the risk of sepsis.
Forty-two of 50 patients (84.0%) who were diagnosed with sepsis-3 presented with initial SIRS in this study. In addition, most patients presented with SIRS during admission because trauma patients usually require surgical or invasive procedures. Hence, it was difficult to distinguish between SIRS caused by trauma or by infection. The SOFA score can also be affected by trauma or by surgery; nevertheless, sepsis-3 might make it easier to define the timing of sepsis. If the patient is diagnosed with the septic condition and infection at some point, the timing of sepsis could be defined by retrospective review of vital signs and SOFA scores.
The respiratory system was the most common focus of sepsis in ICU patients [16]. Quenot et al. [17] demonstrated that 53.6% of ICU patients had respiratory infection as the cause of septic shock. In concordance with the previous study, the respiratory system was the most common focus in our study, with 66.0% of patients having respiratory infection as the cause of septic shock. The patients in this group received more operations, and ventilator care was usually required after surgery. Because prolonged mechanical ventilation increased the risk of respiratory infection in trauma patients [18], early weaning from ventilators via early operation should be considered.
Our study had several limitations. First, this study was retrospective in design and the number of patients was not sufficient. Second, the timing of sepsis is a matter of “hours” not “days.” Third, because some patients were diagnosed with sepsis in the general ward, the timing of sepsis might have been delayed.
In conclusion, sepsis-3 has critical effects in severe trauma patients. Male sex, ISS, lactate, and RBC transfusion were associated with sepsis. Unlike other associated factors, RBC transfusion is a modifiable risk factor. Efforts to reduce RBC transfusion are needed. Additionally, assessment for sepsis should be considered at day 8 in hospital or day 4 postoperative in order to better identify sepsis-3 timing.
KEY MESSAGES
▪ Sepsis was associated with poor outcomes in trauma patients who have survived during initial period.
▪ Around 8 days of hospital admission or 4 days of postoperation, we should pay attention to sepsis.
Notes
No potential conflict of interest relevant to this article was reported.