How to Enhance Critical Care in Korea: Challenges and Vision
Article information

Abstract
The goal of critical care is to reverse patients’ acute problems in effective and ethical ways with minimum costs. Unlike in other medical fields, the quality of Korean critical care has lagged behind that of advanced countries. Moreover, the level of critical care quality differs significantly between university hospitals. The suboptimal critical care level has multifactorial causes. The major challenge to Korean intensivists is, therefore, how to overcome barriers in the current critical care delivery system to improve outcomes for critically ill patients and reduce medical errors in error-prone Intensive Care Unit (ICUs). A long-term task force including all stakeholders should address the multifactorial barriers to better outcomes. The Korean Society of Critical Care Medicine should perform the central role to dismantle the barriers step by step with a long-term vision for a desirable critical care delivery system in our society. A capable critical care team with full-time intensivists is the most urgent requirement for proper, timely care in ICUs. Intensivists should focus on basic but essential management so scarcity of resources can be minimized. Publicity about ICU to the general public is also urgently required to draw the attention of medical policy makers to the current suboptimal level of our critical care system.
Introduction
Critical care medicine provides intensive care and monitoring within an optimal timeframe to prevent premature death and reduce the morbidity and suffering of patients with critical but reversible illnesses. This service is provided in Intensive Care Units (ICUs), which have the infrastructure and expertise necessary to manage critical illness. In Korea in 1962, two university hospitals set up ICUs as postoperative respiratory care units. When the Korean Society of Critical Care Medicine (KSCCM) was organized in 1980, 18 university hospitals and nine general hospitals had ICUs. Although the number of ICUs has been increasing since then, the quality of critical care remains suboptimal compared with other medical specialties in Korea. Moreover, the level of ICU organization and critical care quality differ significantly even between university hospitals.[1] The major challenge to Korean intensivists is, therefore, how to dismantle the barriers in the current critical care delivery system to improve outcomes for critically ill patients and reduce medical errors in ICUs.
Current status of ICUs in Korea
There were an estimated 17 adult ICU beds per 100,000 people in 2009, according to data from the National Health Insurance Corporation (NHIC), which is comparable to other advanced countries.[2] However, it is questionable whether the number of ICU beds reported to NHIC is suitable as a universal definition of ICU adequacy as considered by critical care professionals. A questionnaire survey to identify the current status of ICUs was performed in 2009 by the KSCCM for 105 hospitals registered as critical care specialty training hospitals in Korea.[3] Two hundred twenty ICUs in 86 hospitals (41 in public, 179 in private hospitals) responded to the survey (81.9% response rate). Of those, 56.4% were located in or near the capital city. Most ICUs were open units, and 88.2% of the 220 were specialized (Table 1). In most Korean ICUs, patients are admitted and managed not by a critical care subspecialty, but by a primary attending physician who might not be conversant with current critical care practices and guidelines. Thus, most ICUs in Korean university hospitals are divided simply by the characteristics of commonly admitted patients, but they are not managed by critical specialties suitable to the critical care required. In fact, excluding pediatric ICUs, only 17 ICUs (17.3%) in nine hospitals had intensive care specialists with a 5-day work week, and 12 of those 17 ICUs were in Seoul.
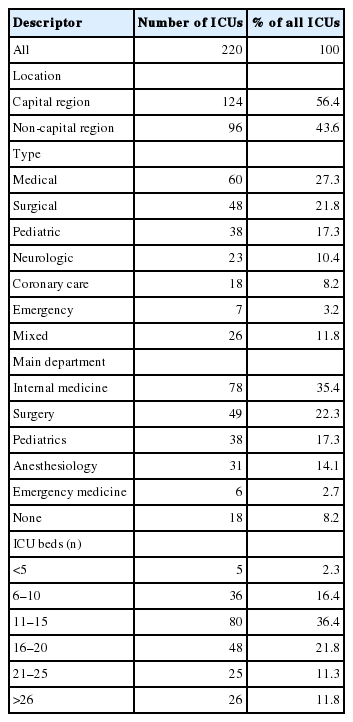
Descriptive characteristics of 220 ICUs in 86 Korean hospitals
The average daytime nurse-to-patient ratio was 1:2.7 and varied from 1:2.9 in small hospitals to 1:3.2 in mixed ICUs. One nurse provided care for more than four patients in 19 of the surveyed units. This situation could become worse at night due to decreased personnel on night shifts, as often occurs in an open ward setting. Moreover, because Korea has very few respiratory therapists, the overall bedside duties of ICU nurses are increased with a corresponding loss of quality in patient care.
On the other hand, medical technology adoption in ICUs is more up-to-date than the staffing of critical care providers. A picture archiving communication system (PACS) was available in 98.6% of the ICUs surveyed, and electronic medical records (EMRs) were available in 49.1%. Local arterial blood gas analysis (ABGA) monitoring was available in 61.4% of the ICUs, and the numbers of ventilators and monitors per bed were 0.66 and 1.10, respectively. Among the 3197 patients covered by the survey, the most common reasons for admission to adult ICUs were respiratory insufficiency and postoperative management.
Challenge in our ICUs
As revealed in the survey, the current crucial challenge in Korean critical care is insufficient staffing to deliver desirable critical care on time, which results in poor outcomes for the critically ill. Although physicians with a critical care subspecialty work in all university hospitals, few of them work in their ICUs as full-time intensivists. Thus, patient care in ICU is at high risk to be fragmented by the individually consulted specialties, and overall care might miss the benefit available from a team approach. To deliver true multidisciplinary care for a critically ill patient with multiple problems, an experienced full-time intensivist should play the key role of integrating recommendations from a multidisciplinary team of professionals. Also, the nurse-to-bed ratio is still poor even in the ICUs of tertiary hospitals. Many studies have demonstrated a relationship between decreased nurse staffing levels and increased adverse patient outcomes in ICU, including mortality, infection, and pressure ulcers.[4–8] To overcome these problems, minimum standards for nurse staffing levels recommended by critical care nurse associations,[9,10] which include nurse-to-patient ratios of 1:1 or 1:2, have been adopted in many advanced countries.[11,12]
The main reason for inappropriate critical care staffing is the financial loss required to maintain even a reasonable, much less a desirable level of ICU staffing in Korea. Even the NHIC’s own investigation in 2004 revealed that the reimbursement rate was around 46% of actual critical care expenses. Moreover, the reimbursement system, which has seven different levels of financial reimbursement, is currently set up to lead to more financial loss as ICU care is enhanced. Critical care staffing was also associated with an inappropriate legal standard for critical care delivery expressed in a regulation of a medical law (enforcement rule article 28, paragraph 8) that was revised by the Ministry of Health and Welfare in 2008. According to the regulation, in contrast with a neonatal ICU which is required to have a full-time specialized doctor; there was no obligation to have a full-time doctor in an adult ICU. After more than 10 years of discussions among stakeholders, including the KSCCM and Ministry of Health and Welfare, the Ministry of Health and Welfare now requires a full-time intensivist with a medical specialty board in th e adult ICU of any tertiary hospital as of July 2014.
The absence of qualified critical care professionals in ICUs leads to a weak standard of care with low compliance to even highly recommended essential measures of critical care. A typical example is the very low compliance rate with the “Surviving Sepsis Campaign guideline” in Korean ICUs,[1] similar to other Asian countries (Fig. 1).[13] The low compliance rate was associated with undesirable mortality from severe sepsis.[13] The high mortality in our ICUs was also revealed by an investigation of the NHIC in 2004. That investigation showed that accumulative mortality of ICU patients, which was calculated by adding the hospital mortality and the mortality within 1 month after discharge from the hospital, was 32.3%. The high rate might partly be due to terminally ill patients who receive care in ICUs in Korea, but who are not recommended for ICU care in high income countries. Nonetheless, when considering that, according to the same 2004 investigation, the medical expenses of ICU patients accounted for 22.5% of total annual medical expenses, improving the outcomes of critically ill patients is a truly urgent challenge to critical care professionals in Korea.
How to enhance critical care?
The goal of critical care support is to prevent premature death and reduce the morbidity and suffering of critically ill patients through intensive therapy for reversible illnesses within an optimal timeframe. The substandard level of critical care in Korean hospitals necessitates system-level change. It is an urgent challenge to be addressed in our healthcare system because the need for appropriate ICUs has been increasing as our society ages. Moreover, recent pandemic illnesses, such as influenza virus and Ebola virus infections, also threaten our society. Figuring out how to solve our multifactorial failure in critical care delivery, including the unreasonable critical care reimbursement system, shortage of critical care professionals, and unacceptable level of legal standards for critical care, is not easy. We need a benchmark to reduce avoidable trial and error and to shorten the learning period by learning from other countries’ critical care delivery systems, and even from lower income countries. For this, the KSCCM has been building partnerships with the Society of Critical Care Medicine, Japanese Society of Intensive Care Medicine, European Society of Intensive Care Medicine, and other societies under the Asian Pacific Association of Critical Care Medicine.
The first recommendation is that we should reprioritize our medical investment for better critical care delivery. Administrators even in university hospitals prefer investing money to upgrade the hardware equipment in an ICU rather than to improve critical care staffing. The KSCCM believes that improving ICU care can be achieved by standardizing critical care through dedicated full-time critical care physicians. The term we choose is important to ensure we are understood and that our meanings are not misinterpreted by others. Full-time intensivist is one example of a term which we have experienced difficulty defining for stakeholders. We need a consensus between stakeholders how to be defined Full-time intensivist considering our current critical care delivery condition. And, a qualified full-time intensivist should be differentiated from a self-intensivist, who is self-qualified for critical care. To prepare qualified intensivists, the Society established a critical care specialty under the endorsement of the Korean Academy of Medical Societies on April 15th, 2008.
Secondly, an efficient critical care team should be established in ICUs. The team does not need to be big at first, but it should be set up with adequate communication among members and rapid decision-making capability. Through a successful critical care team approach, high-quality critical care can be achieved.
Third, we should enhance the relevant legal support. For this, a long-term task force including all stakeholders, including policy makers, should address critical care reimbursement, individualized legal standards for ICU organizations suitable to various hospital levels, and surveillance for ICU quality improvement. Quality improvement should include outcome measures, such as ICU mortality rate, ICU length of stay, average days on mechanical ventilation, suboptimal management of pain, and patient/family satisfaction.[14]
Fourth, we should monitor compliance with essential measures to be performed in ICUs. The essential measures include a patient bedhead elevation of more than 30 degrees, appropriate peptic ulcer disease prophylaxis, appropriate deep venous thrombosis prophylaxis, hand washing, appropriate antibiotic selection on time and duration to use, as-early-as-possible catheter removal, effective assessment of pain and delirium, appropriate use of blood transfusions, and low tidal volume strategy.
Fifth, a rapid response team (RRT) should be implemented at tertiary care hospitals. RRT (commonly called a medical emergency team) goes beyond the critical care team confined to the ICU. Through an appropriate RRT, preemptive management for an acutely deteriorating patient is possible. Last, (and perhaps for some should be regarded as the first), education for the public and policy makers about ICU, what it is and what it needs, should be an ongoing process. Although the concept of critical care has gained widespread acceptance among medical professionals, medical policy makers, the general public, and even hospital administrators’ recognition of the need and role for doctors specializing in critical care has lagged behind in our society.
Conclusion
A lot of work must be done to dismantle the barriers to better critical care in Korea. The KSCCM should play a central role in solving the problems step-by-step with a long-term vision of how to approach improved critical care. To perform the proper care on time with critically ill patients, development of a capable care team with full-time intensivists is the first challenge in most of our ICUs. A well-prepared critical care delivery system must be properly compensated, an urgent requirement in our society. Intensivists should be keen on basic but essential measures for better outcomes so the scarcity of medical resources can be minimized.
Notes
No potential conflict of interest relevant to this article was reported.