Beyond survival: understanding post-intensive care syndrome
Article information

Abstract
Post-intensive care syndrome (PICS) refers to persistent or new onset physical, mental, and neurocognitive complications that can occur following a stay in the intensive care unit. PICS encompasses muscle weakness; neuropathy; cognitive deficits including memory, executive, and attention impairments; post-traumatic stress disorder; and other mood disorders. PICS can last long after hospital admission and can cause significant physical, emotional, and financial stress for patients and their families. Several modifiable risk factors, such as duration of sepsis, delirium, and mechanical ventilation, are associated with PICS. However, due to limited awareness about PICS, these factors are often overlooked. The objective of this paper is to highlight the pathophysiology, clinical features, diagnostic methods, and available preventive and treatment options for PICS.
INTRODUCTION
Intensive care and emergency medicine have undergone significant advancements in the last few decades, which have led to a dramatic improvement in the short-term prognosis and survival rates of intensive care unit (ICU) patients. However, a similar effect has not been observed in quality of life or long-term outcomes [1], and the incidence of new onset or worsening of physical, mental, and neurocognitive health complications in patients following a period of stay in the ICU, collectively referred to as post-intensive care syndrome (PICS), has increased [2]. Physical impairments associated with PICS are largely due to ICU-acquired muscle weakness (ICU-AW), which includes multiple disorders including critical illness neuromyopathy and muscle deconditioning and commonly presents as skeletal muscle weakness and difficulty weaning from the ventilator [3]. Neurocognitive impairments span multiple domains including visuospatial skills, visual and working memory, attention, and executive function [4]. Psychiatric impairments include post-traumatic stress disorder (PTSD), anxiety disorders, and depressive disorders [5]. The effects of PICS can last long after hospital admission, causing patients and their families physical, emotional, and financial stress. Psychiatric and neurocognitive impairments may also be experienced by family members of the patients, which is referred to as PICS-F [6]. A multicenter prospective cohort study from the United States found one or more PICS problems in as many 60% of survivors of a critical illness following ICU admission and co-occurring PICS problems in 20% of survivors of a critical illness following ICU admission [7].
PICS affects one of every five adult patients within 1 year after discharge from a critical care facility [8]. Several modifiable risk factors such as duration of sepsis, delirium, and mechanical ventilation are associated with PICS; controlling these risk factors is associated with lower rates of PICS [7]. A higher incidence of physical and neurocognitive impairments has been reported in patients who underwent a prolonged period of hypoxemia and acute respiratory distress syndrome [9]. Factors such as female sex, pre-existing psychological disorders, inflammation, communication barriers, administration of analgesics, and a negative ICU experience may contribute to the psychiatric aspects of PICS [8]. Higher rates of PTSD were recorded in patients undergoing unplanned admission and surgery, presumably because these patients had less time to prepare psychologically than those who underwent elective surgery. Most studies regarding PICS have been conducted in Europe and the United States, with little data from Asian countries. Recent studies from South and East Asian countries have reported a low incidence of PTSD [10]. However, PICS was documented in multiple countries in Europe as well as China and the United States during the coronavirus disease 2019 (COVID-19) pandemic; symptoms of dyspnea, fatigue, and psychological distress were reported after discharge by ICU patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection [11]. In addition, Halpin et al. [12] reported a high incidence of breathlessness in Black, Asian, and minority ethnic groups at 4–8 weeks after discharge.
Prevention of PICS requires a multidisciplinary approach involving nurses, social workers, and psychologists. Adequate emotional support requires good communication between the discharged patient and the healthcare team, family support in the ICU, and psychological and behavioral therapies. Early nutrition therapy along with early mobilization play crucial roles in preventing physical impairment, including ICUAW [13]. While no association between socioeconomic and PICS-free status has been reported, studies have demonstrated an association between higher number of years of education and higher odds of being PICS-free. This could be due to unmeasured factors such as health literacy, access to health care, and better health behaviors. In addition, frailty is associated with higher rates of mortality and morbidity, with higher Clinical Frailty Scale scores associated with a lower odds of being PICS-free [7]. The purpose of this article is to provide a comprehensive review of PICS including its pathophysiology, prevention strategies, and treatment modalities to increase awareness among medical students, residents, and healthcare professionals.
PATHOPHYSIOLOGY
A dramatic improvement in ICU survival rates have inadvertently resulted in a significantly larger burden of patients who suffer from post-ICU sequelae; however, there is a lack of familiarity and understanding of these post-ICU sequelae (Figure 1).

Post-intensive care syndrome (PICS) manifestations. ICU-AW: intensive care unit-acquired muscle weakness; PTSD: post-traumatic stress disorder.
PHYSICAL IMPAIRMENTS
ICU-AW is the most common and debilitating physical manifestation of PICS and is characterized by symmetrical weakness of the body. This can be subcategorized as critical illness myopathy, which affects the muscles; critical illness polyneuropathy, which affects the nerves; or critical illness neuromyopathy, in which both nerves and muscles are affected. Diagnosis is based on a combined score less than 48 on the Medical Research Council scale after grading all testable muscle groups based on values recorded 24 hours apart [14]. Other contributing factors to weakness include joint contractures due to limited mobility and ectopic ossifications [4]. The pathogenesis of ICU-AW involves multiple factors that can act independently or in combination. The sequence of events is described below.
Muscle Degradation Due to Proteolysis during the Phase of Acute Insult
Microvascular dysfunction plays a pivotal role in the acute phase of critical illnesses and is heavily implicated in the pathogenesis of ICU-AW. Microvascular dysfunction ensues in conditions involving systemic inflammation such as sepsis and results in the transformation of endothelial cells to a pro-inflammatory phenotype. This involves shedding of the endothelial glycocalyx, alterations in the endothelial barrier function, and a subsequent increase in vascular permeability. Proinflammatory transformation of endothelial cells is a key feature of critical illnesses and involves upregulated expression of the inflammatory cytokines tumor necrosis factor (TNF)-α, interleukin (IL)-1, and IL-6, which are all involved in muscle degradation [15]. TNF-α propagates catabolic pathways by promoting increased expression of genes associated with the ubiquitin-proteasome system responsible for massive intracellular proteolysis. IL-1, which is often found in the blood of patients with critical illnesses, has also been identified as a contributor to skeletal muscle atrophy by inhibiting protein synthesis, while IL-6 is involved in both the regulation of protein synthesis and protein degradation [16,17].
Impaired Muscle Regeneration during the Recovery Phase
In those with ICU-AW, impaired muscle degeneration is attributed to the loss of satellite cells, also known as myogenic stem cells, which are located beneath the basal lamina of muscle fibers and proliferate to give rise to myoblasts [18]. Depletion of satellite cells is associated with depletion of endothelial cells as they share regulatory factors such as vascular endothelial growth factor, and notch signaling from endothelial cells drives satellite cells into quiescence, which can potentially lead to satellite cell depletion [19]. Other instrumental mechanisms in ICU-AW include dysregulation of autophagy, which is essential for degradation of damaged cellular components and maintenance of cell homeostasis. Dysregulation of autophagy is associated with muscle wasting and occurs in critical illnesses as a result of the large number of damaged cellular components that accumulate due to inflammation. Mitochondrial dysfunction is also common in ICU-AW, rendering skeletal muscle cells unable to meet their cellular energy demands (Figure 2).
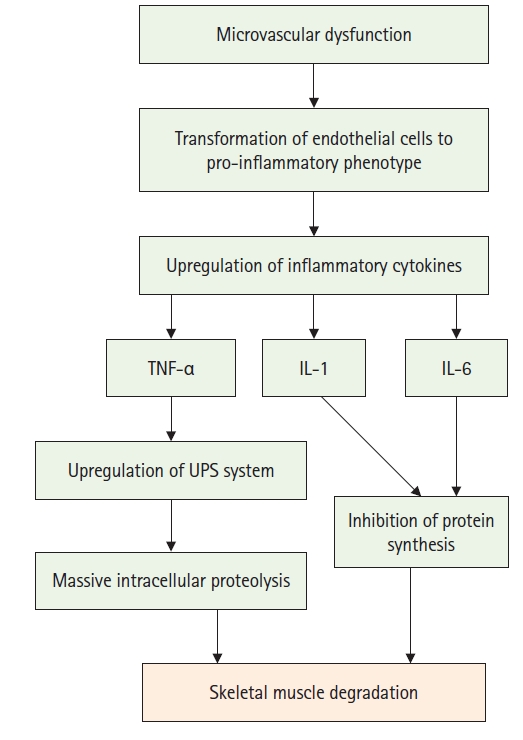
Muscle pathophysiology. TNF: tumor necrosis factor; IL: interleukin; UPS: ubiquitin-proteasome system.
COGNITIVE IMPAIRMENTS
Various mechanisms are involved in the development of long-term cognitive impairment in PICS. One such mechanism is neuronal apoptosis triggered by dopamine receptor activation in response to vagal signals. The vagus nerve is responsible for carrying afferent signals from the peripheral organs to the brain stem, where multi-synaptic pathways are activated. This nerve responds to stimuli such as the stretch reflex in the lungs (particularly in the case of mechanical ventilation) or inflammation (via toll-like receptor-4, IL1R or TNF). Additionally, the vagus nerve is dependent on dopaminergic signaling, which potentiates hippocampal apoptosis [20]. Alongside the aforementioned factors, systemic endothelial dysfunction has also been proposed to play a key role in the development of acute brain injury in ICU survivors. Endothelial dysfunction is a central feature of inflammatory states such as sepsis, and the blood-brain barrier, which comprises endothelial cells, could be vulnerable to the same dysfunction. Endothelial activation can result in increased expression of adhesion molecules and coagulation mediators that can increase blood-brain-barrier permeability, alongside which cerebral hypoperfusion and thrombosis make the brain vulnerable to insult [21]. Cerebral hypoperfusion and thrombosis have been implicated in the development of cerebral ischemia, which can induce white matter changes that may eventually manifest as long-term cognitive impairments (Figure 3) [22].
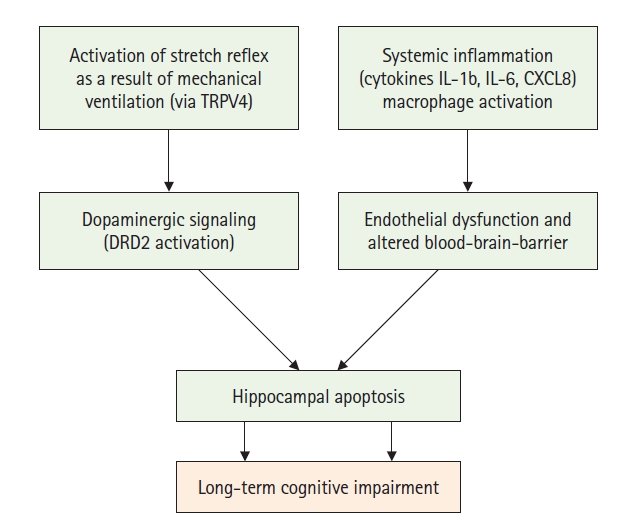
Cognitive pathophysiology. IL: interleukin.
PSYCHOLOGICAL IMPAIRMENTS
Anxiety, depression, and PTSD, all of which are stress-related, are the most common psychological manifestations of PICS, and patients typically present with a combination of these conditions. A negative ICU experience and delirium are significantly associated with development of psychological impairments in post-ICU patients [6]. Delirium in ICU patients is thought to be caused by various mechanisms including loss of central cholinergic activity, increased dopaminergic activity, central nervous system inflammation, hypoxemia, cerebral hypoperfusion, hyponatremia or hypernatremia, and hypoglycemia. Other associated factors include increased glucocorticoid levels during stress and disturbance of the circadian rhythm [23]. In addition to delirium, prolonged sedation, use of benzodiazepines and vasopressors, and lack of social support during the illness are all thought to contribute to psychological impairments in post-ICU patients [24]. Correlations between psychiatric symptoms and post-ICU sleep disturbances have been reported in previous studies [25]. Post-ICU trauma symptoms and depression symptoms are associated with post-ICU sleep disturbances including insomnia, hypersomnia, and excessive day-time sleepiness (Figure 1) [25].
DISCUSSION
Increased use of ICU services and advancements in the diagnosis and treatment of life-threatening conditions such as multiple organ system failure, respiratory failure, sepsis, and shock has resulted in growing numbers of ICU survivors [26]. PICS refers to a complex of symptoms experienced by ICU survivors and characterized by persistent or new onset impairments in physical, cognitive, and psychological components that can negatively affect the quality of life of both the patient and their family.
Approximately 50%–70% of all ICU survivors have at least one PICS-related disability, and these disabilities may persevere for 5–15 years following discharge. Among ICU survivors, nearly 50% have PICS-related physical impairments, and 30%–80% have PICS-related cognitive deficits. These impairments are more prevalent in older individuals [27]. PICS has mostly been evaluated in the primary care setting in the United States. Although identification of PICS symptoms can be difficult, certain aspects of the ICU recovery center, which is a model initiated by Vanderbilt University in 2012, may help diagnose PICS symptoms. In this model, initial evaluation occurs 2 weeks post-hospital discharge and includes spirometry and a 6-minute walk test to evaluate physical impairment. In addition, medication reconciliation and counseling are performed, and the ICU course and related active medical problems are reviewed. Targeted case management assessment; screening for depression, anxiety, and PTSD; and cognitive assessment using the Montreal Cognitive Assessment or Mini-Mental Status exam are also recommended [3,28]. Because executive function is the most commonly affected cognitive domain in PICS, the Society of Critical Care Medicine recommends employing the Montreal Cognitive Assessment, which incorporates an executive function component and is a sensitive detector of mild cognitive impairment [29]. The physical function intensive care test, which has excellent reliability and sensitivity, can also be used to monitor changes in strength and functional outcomes in the ICU. In mechanically ventilated tracheostomy patients who are able to stand, this test can measure endurance, strength, cardiovascular capacity, and functional level and can be repeated after weaning from ventilation [30]. Several prognostic factors such as pre-existing disability, frailty, or nursing home use can be used to predict a patient’s likelihood of complete recovery from intensive care. Patients who have pre-existing disabilities, are frail, and/or who reside in a nursing home are less likely to regain functional independence than previously healthy patients. The National Institute for Health and Care Excellence’s Guidelines on Rehabilitation after Critical Illness recommend multi-professional rehabilitation after critical illness, starting in the ICU and continuing in the ward and after hospital discharge [31]. Guidelines from the Society of Critical Care Medicine's updated Surviving Sepsis Campaign 2021 recommend screening for financial and social support for patients and families and shared decision-making in discharge planning and medications, mentioning sepsis and common impairment after sepsis in the discharge summary, and evaluating for physical, mental, and emotional issues after hospital discharge. Other recommendations include using a critical care transitional program for ICU-to-floor transitions; a hand-off procedure for care transitions; verbal and written sepsis education; and referral of patients to peer support groups, post-critical illness follow-up programs, and outpatient rehabilitation centers [32].
The risk of PICS can be reduced by avoiding sedation, psychotropic use, hypoglycemia, hypoxemia, and environmental modifications and by ensuring early physical rehabilitation and mobility for older people [30]. The Pain, Agitation, and Delirium guidelines are being implemented in ICU care at more than 70 major hospitals across the United States through the ICU Liberation Collaborative, a real-world quality improvement initiative. These guidelines employ the ABCDEF bundle, an evidence-based strategy, to prevent PICS [33]. "A" stands for "assessment, prevention, and management of pain," while "B" represents both spontaneous awakening trials and spontaneous breathing trials, as well as coordination of these trials between nurses and respiratory therapists. "C" represents choice of sedation and analgesia. Numerous studies have shown that patients who are kept "awake and alert" or barely sedated with drugs other than GABAergic benzodiazepines spend less time on a ventilator and are more likely to be delirium-free. "D" stands for delirium assessment, prevention, and management and allows identification of otherwise overlooked delirium and triggers patient-centered interventions to shorten the length of brain dysfunction through adherence to each of the bundle pieces. "E" stands for early mobility and exercise. This part of the bundle necessitates an aggressive approach by the team (not just the therapists, but also the nurses). This can be extremely difficult at times because it requires taking intubated patients off sedation and getting them out of bed. "F" stands for family engagement and empowerment (Table 1) [34].
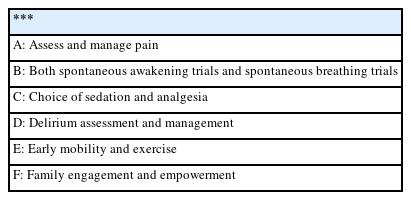
Preventing PICS, the ABCDEF bundle
Compliance is a crucial aspect of prevention and management of PICS since changes in compliance with different elements of the ABCDEF bundle and other treatment strategies can alter and even negate outcome benefits. Various studies have shown that patients do not improve if compliance is not high and if all the elements of the ABCDEF bundle are not followed [33]. Due to the strong connection between nutritional therapy and PICS, nutritional therapy is crucial for PICS prevention. Appropriate energy delivery and protein intake are the most essential components of muscle synthesis; however, overfeeding should be avoided as it could induce autophagy and worsen PICS [1]. Another method to prevent PICS is an ICU diary, a record of medication and interventions kept for ICU patients while they are sedated and ventilated. It is written by family members, nurses, and others. After discharge, the patient can read the diary and gain a better understanding of what has occurred. This has been shown to reduce PTSD symptoms in patients and their families [35].
Given that oversedation contributes to the development of cognitive and psychiatric symptoms, guidelines recommend decreased use of sedation for ventilated patients. Customized sedation and analgesia management for individual patients is crucial to avoid cognitive impairment, such as confusion and delirium; these interventions also reduce pain and improve mobility. Environmental changes are useful in lowering the likelihood of delirium. Dark rooms, constant noise, and frequent interruptions have all been associated with disturbance of the sleep-wake cycle, which may induce delirium and should be avoided. Anticholinergics, opioids, and sedative medicines should be used cautiously in the treatment of delirium [36].
Follow-up of patients discharged from the ICU can be performed at intensive care follow-up clinics, which can also be used as locations to diagnose and treat PICS. Although mainly used in Europe, these follow-up clinics are gradually being introduced in North America. There is no fixed template for these types of facilities or patient evaluation methods, and treatment modalities may vary. Reduction of PTSD symptoms among follow-up patients at these clinics may be due to individualized interventions; more research is required to establish the usefulness of these facilities (Tables 2 and 3) [1].
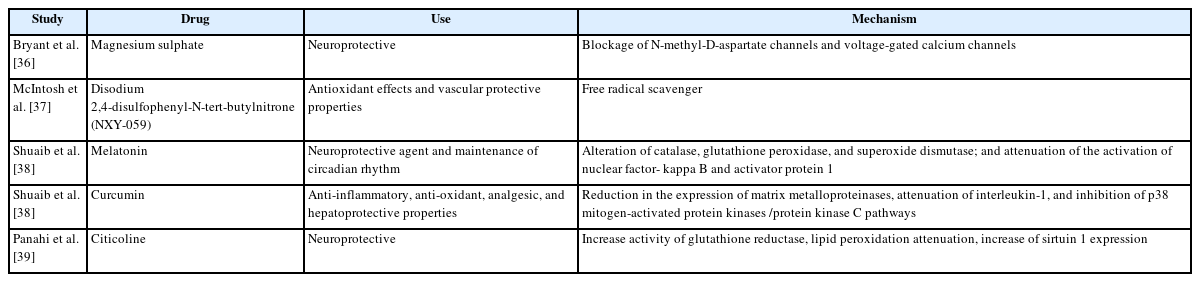
Pharmacological intervention of post-intensive care syndrome
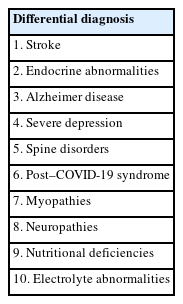
Differential diagnosis of post-intensive care syndrome
CONCLUSIONS
A plethora of impairments spanning physical, psychiatric and neurocognitive domains is increasingly being seen in patients following a period of stay in intensive care facilities; these impairments have an adverse long term impact on the well-being of both patients and their families. Several modifiable and non-modifiable factors spanning patient demographics such as age, sex, race, preexisting disabilities, frailty, hypoxia, and negative ICU experiences have been reported to increase the risk of PICS. Catabolic pathways leading to muscle degeneration and neuronal apoptosis along with endothelial dysfunction can lead to various impairments. A multimodal approach addressing contributing factors, communication techniques, and involvement of psychotherapy as well as physical and nutritional therapy needs to be incorporated into ICU care to decrease the incidence of PICS. Assessment of physical and neurocognitive function along with screening for psychiatric disorders at regular follow-up visits is important to identify and manage PICS early in its disease course. Future studies are required to gain a better understanding of the pathophysiology of PICS and to identify prevention and treatment strategies.
KEY MESSAGES
▪ Post-intensive care syndrome refers to the persistent or newly onset physical, mental, and neurocognitive complications that can occur following a stay in the intensive care unit.
▪ It was extensively observed during coronavirus disease 2019 (COVID-19) pandemic in the United States among other countries.
▪ Its manifestations include physical impairments, including impaired muscle regeneration, cognitive impairment, and psychological impairment.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
ACKNOWLEDGMENTS
None.
AUTHOR CONTRIBUTIONS
Conceptualization: JM, BS. Visualization: JM, BS. Project administration: JM. Writing–original draft: LG, MNS, JM, BS, VB. Writing–review & editing: VB, VG, RJ.