Association between mechanical power and intensive care unit mortality in Korean patients under pressure-controlled ventilation
Article information
 , Sang-Min Lee2, Hyung Koo Kang3, Kyung Chan Kim4, Young Sam Kim5, Yun Seong Kim6, Won-Yeon Lee7, Sunghoon Park8, So Young Park9, Ju-Hee Park10, Yun Su Sim11, Kwangha Lee12, Yeon Joo Lee13, Jin Hwa Lee14, Heung Bum Lee15, Chae-Man Lim16, Won-Il Choi17, Ji Young Hong18, Won Jun Song19, Gee Young Suh,20
, Sang-Min Lee2, Hyung Koo Kang3, Kyung Chan Kim4, Young Sam Kim5, Yun Seong Kim6, Won-Yeon Lee7, Sunghoon Park8, So Young Park9, Ju-Hee Park10, Yun Su Sim11, Kwangha Lee12, Yeon Joo Lee13, Jin Hwa Lee14, Heung Bum Lee15, Chae-Man Lim16, Won-Il Choi17, Ji Young Hong18, Won Jun Song19, Gee Young Suh,20
Abstract
Background
Mechanical power (MP) has been reported to be associated with clinical outcomes. Because the original MP equation is derived from paralyzed patients under volume-controlled ventilation, its application in practice could be limited in patients receiving pressure-controlled ventilation (PCV). Recently, a simplified equation for patients under PCV was developed. We investigated the association between MP and intensive care unit (ICU) mortality.
Methods
We conducted a retrospective analysis of Korean data from the Fourth International Study of Mechanical Ventilation. We extracted data of patients under PCV on day 1 and calculated MP using the following simplified equation: MPPCV = 0.098 ∙ respiratory rate ∙ tidal volume ∙ (ΔPinsp + positive end-expiratory pressure), where ΔPinsp is the change in airway pressure during inspiration. Patients were divided into survivors and non-survivors and then compared. Multivariable logistic regression was performed to determine association between MPPCV and ICU mortality. The interaction of MPPCV and use of neuromuscular blocking agent (NMBA) was also analyzed.
Results
A total of 125 patients was eligible for final analysis, of whom 38 died in the ICU. MPPCV was higher in non-survivors (17.6 vs. 26.3 J/min, P<0.001). In logistic regression analysis, only MPPCV was significantly associated with ICU mortality (odds ratio, 1.090; 95% confidence interval, 1.029–1.155; P=0.003). There was no significant effect of the interaction between MPPCV and use of NMBA on ICU mortality (P=0.579).
Conclusions
MPPCV is associated with ICU mortality in patients mechanically ventilated with PCV mode, regardless of NMBA use.
INTRODUCTION
Mechanical ventilation is an essential component of critical care, but it can damage the lungs, an event called ventilator-induced lung injury (VILI). Therefore, the primary goal of mechanical ventilation is to maintain adequate gas exchange and to reduce the work of breathing while minimizing VILI [1]. To achieve this goal, lung protective strategies, in which tidal volume and plateau pressure are limited, have been widely adopted [2]. However, other ventilator variables such as respiratory rate and driving pressure have also been shown to be associated with the development of VILI [3,4]. Because of the interdependence of the variables and the requirement for adequate gas exchange, adjustment of one variable results in changes in the other variables. Thus, it is difficult to predict how the adjustment of one variable will affect VILI.
Gattinoni et al. [5] proposed the mechanical power (MP) concept, which refers to the amount of energy transferred to the lungs as the result of mechanical ventilation and integrates various ventilator variables affecting VILI; these authors proposed a calculation of MP based on the equation of motion. Experimental studies have found correlations between MP and lung injury [6-8]. In a large observational study, MP was associated with higher mortality, longer intensive care unit (ICU) and hospital lengths of stay, and fewer ventilator-free days [9]. Gattinoni and colleagues’ original equation for MP is based on volume-controlled ventilation with a linear increase in airway pressure and was validated in paralyzed patients [5]. Thus, this equation may not be useful in a significant number of mechanically ventilated patients because the use of pressure-regulated ventilation has been increasing [10], and restricted use of neuromuscular blocking agents (NMBAs) is advocated due to their detrimental effects [11,12].
Recently, Becher et al. [13] developed an equation to calculate MP for patients under pressure-controlled ventilation (PCV) mode. This equation easily can be calculated with readily available parameters and may serve as a useful monitoring index in patients on PCV but has not been studied extensively, especially in patients undergoing ventilation with or without NMBA. We aimed to examine the association between ICU mortality and MP calculated using Becher’s equation (MPPCV) in patients undergoing PCV and to investigate whether the use of NMBA affects this relationship.
MATERIALS AND METHODS
Design and Population
This study was a retrospective analysis of a prospective Korean cohort that formed part of an international study [14]. The study protocol was approved by the Institutional Review Boards of all participating hospitals, and the need for informed consent was waived due to the non-interventional nature of the protocol. In 2016, 226 patients from 18 Korean ICUs participated in the Fourth International Study of Mechanical Ventilation of the VENTILA group [15]. That was a prospective, international, multicenter, non-interventional cohort study that enrolled adult patients who received invasive mechanical ventilation for at least 12 hours or non-invasive ventilation for more than 1 hour (https://clinicaltrials.gov/ct2/show/record/NCT02731898). Patients who were ventilated with PCV on day 1 were included in this study.
Data Collection Time
According to the parent study protocol, the day of initiation of mechanical ventilation was considered day 0, and the next day was considered day 1. Data were collected for the duration of mechanical ventilation or until day 28. For patients with invasive mechanical ventilation, blood gas analysis, ventilator mode and settings, and co-adjuvant therapies (sedatives, analgesics, NMBAs) were recorded daily at 8 am from day 1 (on day 0, data were collected within the first hour of starting mechanical ventilation). Documented ventilator settings were as follows: total and ventilator respiratory rates (per minute), tidal volume (mL), peak pressure (cm H2O), plateau pressure (cm H2O), and applied positive end-expiratory pressure (PEEP; cm H2O). We extracted and analyzed the day 1 data. Basal demographics, primary reasons for invasive mechanical ventilation, and discharge status were also collected.
Calculation of MP
We calculated the MP of patients under PCV using Becher’s simplified equation:
MPPCV=0.098 ∙ RR ∙ VT ∙ (ΔPinsp + PEEP),
where ΔPinsp is the change in airway pressure during inspiration (cm H2O), RR is respiratory rate (per minute), VT is tidal volume (L), and 0.0998 is a correction factor to convert the units to J/min [13]. If the total respiratory rate and ventilator respiratory rate were different, the total respiratory rate value was entered in the RR term of the equation. Peak pressure was substituted for the last term of the equation.
Statistical Analysis
Patients were divided into survivors and non-survivors. Categorical variables are reported as number and percentage and were compared using Fisher’s exact test or the chi-square test. Continuous variables are reported as median with interquartile range and were compared using the t-test or Mann-Whitney U-test, as appropriate. The normality of distributions was examined by the Kolmogorov-Smirnov test. Multivariable logistic regression analysis was performed to identify factors associated with ICU mortality. Variables with P-value less than 0.2 in univariable analysis and clinical variables shown to be important in previous studies (age and sex) were included in the multivariable analysis to investigate prognostic factors for ICU mortality. We also analyzed the interaction between MPPCV and the use of NMBA to investigate an effect on the association between MPPCV and ICU mortality. Multivariable logistic regression analysis for ICU mortality was conducted and included the interaction term of MPPCV and NMBA use. In addition, we conducted subgroup analysis by categorizing patients based on the presence or absence of spontaneous breathing effort, using respiratory rate as the criterion. When the ventilator respiratory rate was equal to the total respiratory rate, this was considered absence of spontaneous breathing effort (controlled ventilation group). Conversely, if the total respiratory rate was higher than the ventilator respiratory rate, this was considered presence of spontaneous breathing effort (spontaneous breathing group). The logistic regression results are reported as odds ratio (OR) of each variable with 95% confidence interval (CI). All tests were two-sided, and a P-value less than 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS ver. 20.0 (IBM Corp.) and SAS ver. 9.4 (SAS Institute Inc.).
RESULTS
Two hundred twenty-three patients were treated with invasive mechanical ventilation on day 1, and PCV mode was applied to 160 of them. MPPCV could be obtained for 125 patients. Of these, 87 survived and 38 died in the ICU (Figure 1). Overall, baseline characteristics were comparable between survivors and non-survivors (Table 1). Median age was 68 years, and two-thirds of patients were male. The majority of patients received mechanical ventilation owing to acute respiratory failure. The use of analgesics was more frequent in non-survivors (72.4 % vs 92.1%, P=0.014). NMBA was used twice as frequently in non-survivors than survivors, but this difference was not significant (11.5% vs. 23.7%, P=0.081).
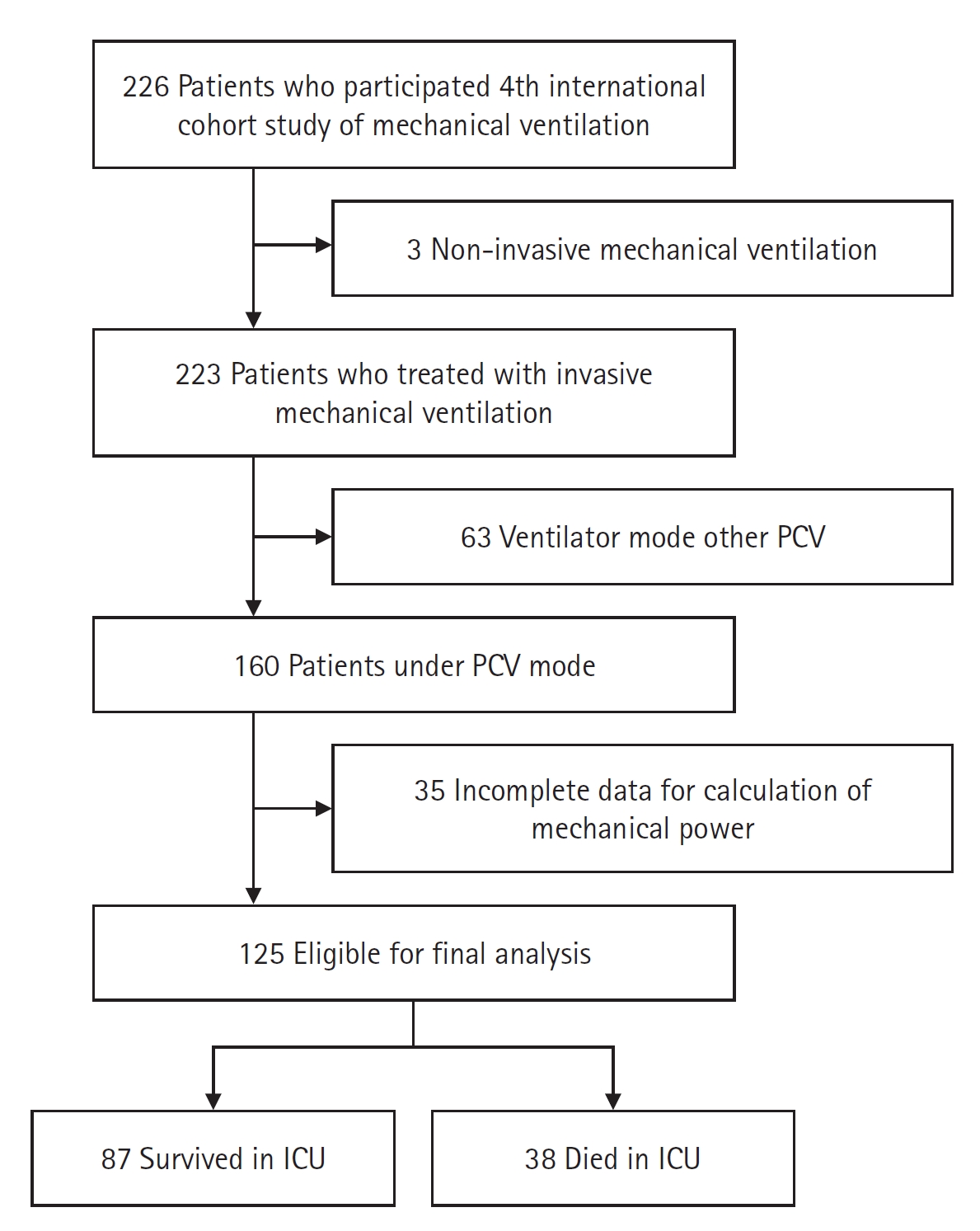
Study flowchart. PCV: pressure-controlled ventilation; ICU: intensive care unit.

Baseline characteristics
MPPCV in the whole study population was 21.7 J/min and was significantly higher in non-survivors than survivors (17.6 J/min vs. 26.3 J/min, P<0.001). Overall tidal volume per predicted body weight (VT/PBW) was 7.2 mL/kg and was higher in non-survivors than survivors (7.0 ml/kg vs. 8.2 ml/kg, P=0.025). PEEP was similar in the two groups (Table 2).

Comparison of day 1 ventilator variables between survivors and non-survivors
Table 3 shows the results of logistic regression analysis. Analgesic use, MPPCV, and VT/PBW were significantly associated with ICU mortality in univariable analysis and were included in the multivariable analysis. Age, sex, and other variables with p-value less than 0.2 in the univariable analysis were also included in multivariable analysis. Among them, only MPPCV was significantly associated with ICU mortality (OR, 1.090; 95% CI, 1.029–1.155; P=0.003).

Logistic regression analysis for intensive care unit mortality
Regarding ICU mortality, there was no significant interaction between the MPPCV and the use of NMBA (P=0.579). In patients who were not treated with NMBA, MPPCV was significantly associated with ICU mortality (OR, 1.081; 95% CI, 1.017–1.149; P=0.013). In patients who received NMBA, ICU mortality also tended to increase with higher MPPCV, although significance was not achieved (OR, 1.125; 95% CI, 0.987–1.283; P=0.078) (Table 4).

Association between MPPCV and intensive care unit mortality according to the use of neuromuscular blocking agents.
In subgroup analysis, 51 patients (42.5%) were assigned to the controlled ventilation group. The MPPCV was higher in non-survivors than survivors (21.6 J/min vs. 26.7 J/min, P=0.045) in the controlled ventilation group (Supplementary Table 1). In multivariable analysis, we observed a significant association between high MPPCV and an increase in ICU mortality rate (OR 1.177, 95% CI, 1.030–1.344; P=0.016) (Supplementary Table 2). Similar results were found in the spontaneous breathing group (Supplementary Tables 3 and 4).
DISCUSSION
In the present study, we found that MPPCV, which can be calculated with universally monitored parameters at the bedside, was significantly associated with ICU mortality. In fact, MPPCV was the only independent predictor of ICU mortality in the multivariable logistic regression analysis. In addition, the association between MPPCV and ICU mortality was not affected by the use of NMBA, which suggests MPPCV as a predictor of mortality regardless of the use of NMBA.
One of the most important findings in this study is that MPPCV was associated with poor outcomes in Korean patients undergoing mechanical ventilation in PCV mode for respiratory failure. Although several studies have investigated the associations between MP and clinical outcomes, most of the studies have enrolled patients undergoing ventilation in volume-controlled mode and calculated MP using Gattinoni’s equation. For example, in one study that reported an association between poor outcome and MP calculated with Gattinoni’s equation, 90% of patients were treated with volume-controlled ventilation [16]. Other large-scale studies either did not provide information on ventilation modes [9,17,18] or included some patients who were ventilated in PCV mode [19] but used Gattinoni’s equation to calculate MP. Since the use of pressure-regulated ventilation is increasing globally, especially in Korea, the results of our study can be clinically helpful [10,14,20]. Moreover, we used Becher's simplified equation, which is easy to calculate at the bedside because it incorporates only variables that are readily obtained from the ventilator.
Another notable aspect of this study is that we analyzed the effect of NMBA on the relationship between MP and ICU mortality. If we want to use MP as a surrogate for risk for VILI, it should be calculated with patients under passive conditions because published equations for MP cannot account for changes in values induced by spontaneous effort of the patient. In Becher’s equation, the effect of spontaneous breathing efforts on calculated MPPCV can be variable. Tidal volume should increase if there is spontaneous breathing effort at the same peak inspiratory pressure; at the same time, lower peak inspiratory pressure is needed to achieve the same tidal volume when the patient has spontaneous breathing efforts. However, only a subset of patients treated with mechanical ventilation receives NMBA, and this proportion is gradually decreasing [10,21], which would lessen the clinical usefulness of MP as a bedside monitoring tool or ventilator-adjustment target if it has value only in passive patients. Indeed, only 15% of participants received NMBA in our study. Previous studies on the association between MP and clinical outcomes have either tried to exclude patients with spontaneous efforts by excluding patients with a higher measured respiratory rate than the set respiratory rate [18,19] or included patients with spontaneous breathing in their analysis as well [17]. Our study is meaningful in that we assessed spontaneous breathing (or paralysis) based on NMBA use and subsequently analyzed the impact of NMBA use on the association between MP and clinical outcomes. We demonstrated that MPPCV was independently associated with ICU mortality irrespective of the use of NMBA. Serpa Neto et al. [9] also found no interaction between NMBA use and clinical outcomes, although they used the MP equation, which is based on volume-controlled ventilation.
Interestingly, MPPCV was the only variable associated with ICU mortality in multivariable analysis. VT/PBW was significantly higher in non-survivors than survivors and was significantly associated with ICU mortality in univariable analysis, but this significance did not persist in multivariable analysis. This should not be interpreted to mean that VT/PBW does not affect clinical outcomes. It is well-known that different variables used to calculate MP have different impacts on MP, and tidal volume is one of the variables with the strongest influence. For example, tidal volume, PEEP, and respiratory rate can all contribute to MP; however, when each respective value is doubled, MP increases by 4 times, 2 times, and 1.4 times [5]. Moreover, the effect of VT/PBW would be diluted in studies involving a relatively small number of patients if a low tidal volume ventilation strategy is being universally applied [21].
There are several limitations to this study. First and foremost, MPPCV as calculated by Becher’s equation may not represent the true MP delivered to the patient by the ventilator. Since Becher’s equation calculates MP under the assumption of an ideal “square wave,” this assumption may not hold true in a spontaneously breathing patient. Moreover, as spontaneous efforts increase, the airway pressure will tend to deviate increasingly from this assumption. Also when there is spontaneous effort, tidal volume will increase at the fixed inspiratory pressure, which might result in overestimation of the MP delivered by the ventilator. However, distending pressure and tidal volumes created by spontaneous effort could also be damaging [22], and MPPCV calculated by Becher’s equation may prove to have prognostic significance even in spontaneously breathing patients, as was shown in this study. Further studies are needed on this subject. Second, since this was a retrospective study, we are not able to exclude the possibility of residual confounding factors. Third, only MPPCV on day 1 was used for analysis. Thus, we did not evaluate MPPCV on days other than day 1 or changes in MPPCV and their potential impact on patient outcomes. Fourth, due to the relatively small size of the study population, caution should be used when generalizing the results, as there may be other potentially important differences that were not found due to lack of statistical power. However, all patients starting mechanical ventilation were prospectively included from 18 Korean ICUs during the study period according to an established protocol. Fifth, the presence or absence of NMBA use may not completely distinguish passive ventilation and spontaneous breathing. Finally, we did not compare the equation to calculate MP in this study with other equations proposed to calculate MP in PCV mode [13,23,24]. However, other equations are more complex, and we wanted to evaluate the usefulness of Becher’s simplified equation because it can be readily applied at the bedside.
In conclusion, MPPCV was associated with ICU mortality in patients mechanically ventilated with PCV mode regardless of NMBA use. High MPPCV during the initial phase of mechanical ventilation could be predictive of a poor prognosis. Further prospective studies are needed to establish a specific cut-off value and to confirm that MPPCV can serve as a monitoring index or therapeutic target.
KEY MESSAGES
▪ Mechanical power calculated using Becher’s simplified equation (MPPCV) was significantly associated with intensive care unit (ICU) mortality in Korean patients on pressure-controlled ventilation.
▪ The association between MPPCV and ICU mortality was not affected by the use of neuromuscular blocking agent.
Notes
CONFLICT OF INTEREST
Kwangha Lee is an editorial board member of the journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflict of interest relevant to this article was reported.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualization: JKS, GYS. Data curation: all authors. Formal analysis: JKS, GYS. Visualization: JKS. Supervision: GYS. Writing–original draft: JKS. Writing–review & editing: SML, HKK, KCK, YSK, YSK, WYL, SP, SYP, JHP, YSS, KL, YJL, JHL, HBL, CML, WIC, JYH, WJS, GYS. All authors read and agreed to the published version of the manuscript.
Acknowledgements
Part of this work was presented at the 26th Congress of the Asian Pacific Society of Respirology (APSR 2022).
The authors would like to thank all members of the Korean Study Group on Respiratory Failure (KOSREF). They would also like to thank Soon-Young Hwang from the Department of Biostatistics at Korea University College of Medicine for providing valuable advice on statistical analysis.
SUPPLEMENTARY MATERIALS
Supplementary materials can be found via https://doi.org/10.4266/acc.2023.00871.
Comparison of day 1 ventilator variables between survivors and non-survivors in controlled ventilation group
acc-2023-00871-Supplementary-Table-1.pdfLogistic regression analysis for intensive care unit mortality in controlled ventilation group
acc-2023-00871-Supplementary-Table-2.pdfComparison of day 1 ventilator variables in patients with spontaneous breathing in spontaneous breathing group
acc-2023-00871-Supplementary-Table-3.pdfLogistic regression analysis for intensive care unit mortality in spontaneous breathing group
acc-2023-00871-Supplementary-Table-4.pdf