Quality of life among patients with supraventricular tachycardia post radiofrequency cardiac ablation in Jordan
Article information

Abstract
Background
Supraventricular tachycardia (SVT) is a common arrhythmia with associated symptoms such as palpitation, dizziness, and fatigue. It significantly affects patients’ quality of life (QoL). Radiofrequency cardiac ablation (RFCA) is a highly effective treatment to eliminate arrhythmia and improve patients’ QoL. The purpose of this study was to assess the level of QoL among patients with SVT and examine the difference in QoL before and after RFCA.
Methods
One group pre-posttest design with a convenience sample of 112 patients was used. QoL was assessed by 36-Item Short Form (SF-36). Data were collected at admission through face-to-face interviews and 1-month post-discharge through phone interviews.
Results
There was a significant difference between QoL before (33.7±17.0) and 1 month after (62.5±18.5) the RFCA. Post-RFCA patients diagnosed with atrioventricular nodal reentrant tachycardia had higher QoL than other types of SVT. Moreover, there were significant negative relationships between QoL and the number and duration of episodes pre- and post-RFCA. There were no significant differences in QoL based on: age, sex, working status, marital status, smoking, coronary artery disease, diabetes mellitus, and hypertension.
Conclusions
After RFCA, the QoL of patients with ST improved for both physical and mental component subscales.
INTRODUCTION
The occurrence of supraventricular tachycardia (SVT) is estimated at 36 per 100,000 individuals per year in the US population. There are nearly 89,000 new cases and 570,000 individuals with SVT each year [1]. In 2018 the prevalence of SVT was approximately 1.26 million individuals and the incidence rate was about 188,981 among U.S. population [2]. In the UK, more than a million people suffer from cardiac arrhythmias each year [3].
SVT occurrence according to age and sex compared to other cardiac disorders was previously studied [4]. Patients who had SVT without any cardiovascular disease were younger than patients with cardiovascular disease. The percentage of atrioventricular tachycardia (AVRT) patients decreases with age, while the rate of atrioventricular nodal reentrant tachycardia (AVNRT) and atrial tachycardia (AT) patients increases with age. Individuals more than 65 years of age have more than five times the likelihood of developing SVT than younger individuals, and the mean age of incidence is 45 years, with 62% occurring in women. Women are at double risk compared to men of developing SVT [4].
Besides non-invasive measures, radiofrequency cardiac ablation (RFCA) is a definitive cure for most SVTs and considered the last therapeutic choice for treatment in the chronic stage for SVT [5]. In addition to medical therapy, RFCA is a perfect option for potentially curative treatment targeting the origin of SVT without the need for chronic medical treatment [6]. All patients with severe clinical symptoms or frequent SVT episodes should be referred for electrophysiological studies (EPS) to consider the ablation procedure as a first-line treatment because it offers the potential for definite treatment. The effective rate of RFCA is 95%, the recurrence rate is less than 5%, and complications of the procedure include unintentional complete heart block in less than 1% of patients [7]. Moreover, deep vein thrombosis, bleeding, and femoral arteriovenous fistula could be the other complications [8]. In addition to that, heart disorders affect the multidimensional quality of life (QoL) relative to healthier people. It influences everyday life habits, including physical and social activities, and psychological fields such as being comfortable and pleased with living, financial, and satisfying relationships. The negative impact of heart disease on physical ability was the most common effect [9].
Several socio-demographics, physiological, and psychological influences have affected QoL in patients with heart disease [10]. Other factors influencing QoL include anxiety and depression, which are common in patients with heart disease. The prevalence rates of anxiety and depression in patients with heart disease are four to five times higher than in the general population [11].
The World Health Organization defined the QoL as “individuals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns” [12]. It is an important term that is influenced in multipart ways by the physical well-being, psychological condition, degree of freedom, social interactions, personal beliefs, and the interaction with their environment [13]. Due to the abrupt recurring symptoms of patients with SVT, their QoL might be affected [14, 15]. Most patients feel social isolation, postpone day-to-day tasks, have body pain, and decline in general health, whereas absence from work may exceed 12% in affected people [16].
The RFCA is the option treatment to improve QoL for these patients, and it is now the mainstay procedure for most arrhythmias. In addition, it can provide a better option and a permanent cure for those suffering from extreme arrhythmias to enhance QoL [17]. Many western countries have researched the effect of RFCA on QoL among patients with SVT. Results indicated that RFCA, which can successfully cure patients with SVT, dramatically increases physical, mental, and social health ratings by eliminating arrhythmia episodes and related signs of agitation in those patients irrespective of demographics and form SVT [18,19]. Therefore, the study's primary purpose was to assess QoL level and examine the difference in QoL pre and post-RFCA.
The study was designed specifically to answer the following research questions: (1) What is the baseline level of QoL for patients with SVT pre-RFCA? (2) Does the QoL of patients with SVT differ between pre and post RFCA? (3) Is there a difference in QoL according to socio-demographic and clinical characteristics among patients diagnosed with SVT post-RFCA?
MATERIALS AND METHODS
Design
One group pretest-posttest design examined the QoL among patients with SVT in Jordan pre and post RFCA.
Population
The target population was any patient diagnosed with SVT and undergoing EPS and RFCA procedures. The accessible population was patients who underwent EPS and RFCA procedures at Queen Alia Heart Institute (QAHI).
Sample and Sampling
Convenience sampling was used based on the following inclusion criteria: patients >18 years old, able to read and understand Arabic, medically diagnosed as SVT by a cardiologist, and Planned for RFCA. Exclusion criteria were patients with other cardiac arrhythmias.
Sample Size
The sample size was calculated using G Power software [20]. Taking into consideration the main purpose of the study and the main statistical analysis (independent samples t-test, paired samples t-test and analysis of variance [ANOVA]), assuming a power of 80%, a medium effect size of 0.5 and α level of 0.05, a total of 119 patients was sufficient to detect any statistically significant difference in the socio-demographics of the patients and their QoL pre and post RFCA. Around 10% of the measured sample size was added to compensate for any attrition.
Setting
This study was conducted in RMS at the cardiac health care center (QAHI) in Amman. The QAHI is a specialized healthcare center for all cardiac diseases and surgeries. The QAHI covers a wide range of patients, as it receives patients from both the private, governmental and the military sector in Jordan. It provides health care for all cardiac disease patients in Jordan and includes patients from neighboring countries and regions.
Data Collection Procedure
First, after getting ethical approval, the principal investigator gave the hospital complete information about the study, including its purpose, significance, and procedure. Second, after taking permission, the principal investigator invited the patients who met the inclusion criteria to participate in the study after a detailed explanation. Patients were told that the study will be done in two phases: the first phase, before the RFCA, face-to-face structured interview, and the second phase, 1 month after discharge, structured phone interview with the same questionnaire. Third, patients who accepted to participate signed a consent form.
Instruments
The socio-demographic and clinical characteristics included: age, sex, marital status, level of education, job condition, co-morbidities, the average number of episodes of fast heart rhythm last month, duration of an episode of rapid heart rhythm occurring the previous month in minutes, types of SVT, and use of antidysrhythmic drugs.
QoL was measured using 36-Item Short Form (SF-36) Survey version one, a multi-use, short-form health survey with 36 questions. This form was developed in 1992 and updated in 2000 [21,22]. The SF-36 helps assess public health, estimating the burden of various diseases, measuring clinical practice results, and evaluating treatment impact, and is widely regarded as the gold standard for QoL assessment [23,24]. The SF-36 consisted of eight domains of two component summary (Physical and Mental). Physical component summary (PCS) consists of physical functioning, role limitations due to physical health, body pain, and general health. Mental component summary (MCS) consists of role limitations due to emotional problems, energy/fatigue, emotional well-being, and social functioning.
The full scale and each health domain's scores are converted to a 0–100 scale to provide a consistent numerical measure. The higher the value of each health domain, the better the health status [25]. High scores reflect a stronger state of health and well-being and the absence of limitations and impairment [22]. Scoring the SF36 is a two-step process. First, each item is scored on a 0 to 100 range so that the lowest and highest possible scores are 0 and 100, respectively. Scores represent the percentage of total possible score achieved. In step 2, items in the same subscale are averaged together to create the subscale scores. Total scale scores represent the average for all items in the scale that the respondent answered ranges from 0 and 100. SF36 was used because the QoL is believed to include these concepts measured in the subscales of SF36. Moreover, SF36 was used previously in many articles focused on QoL in patients with cardiac diseases [22]. Using this scale made the comparison with previous literature more scientific. The Arabic version has been found to be reliable by several populations [26]. Cronbach’s alpha coefficients were between 0.7 and 0.9, which was boosted in other studies [23,24]. Moreover, the Arabic version of SF36 also showed good psychometric properties in a sample of Arab patients with heart failure [27]. Cronbach's alpha of SF-36 in this study was 0.87, while the value of the domains ranged between (0.61–0.79). Scores below 47 for each domain, PCS, and MCS were considered as poor QoL [27].
Ethical Consideration
Data was collected after getting approval from the Institutional Review Board from the ethical and scientific committee of the faculty of nursing, the deanship of academic research at the Applied Science Private University, the QAHI (No. 2020-2021-2-9). All methods were performed in accordance with the relevant guidelines and regulations of the committee and according to the Declaration of Helsinki. In this study, patients were informed that their participation was voluntary. All patients signed an informed consent form. Therefore, they could leave the study at any time without any influence on the quality of care for those patients. Furthermore, patients were informed about the privacy and confidentiality of the study. In addition, the questionnaires did not include patients’ names or personal information. Instead, each patient was given a numerical code number according to the guidelines to protect their identity.
Data Analysis
Statistical analysis was conducted using IBM SPSS ver. 21.0 (IBM Corp.). Descriptive statistics, including means, standard deviations, and percentages, were used to answer research question number 1 and describe the sample. A paired sample t-test was used to answer research question number 2. Finally, an independent sample t-test, one-way ANOVA, and Pearson r correlation were used to detect differences in mean scores pre- and post-RFCA according to question number 3.
RESULTS
Socio-demographic and Clinical Characteristics
A total of 126 patients scheduled for the RFCA procedure have been invited to participate in the study on the same day before the procedure. Unfortunately, two patients had their operations canceled, and four refused to participate. Finally, 120 patients completed the pre-procedure data collection (response rate before RFCA=95%), and they were asked to complete the participation through a phone interview 1 month after the RFCA. One month after the procedure, 112 patients completed the study through phone interviews (response rate after the procedure was 93%). Eight patients did not complete the phone interview (five were diagnosed with AF, and three had disconnected phones). The mean age was 41±13 years. More than half of them (54.2%) had a secondary school education, and 35.8% had a BSc. More than half (55%) were females, 56.7% were unemployed, and 73.3% were married. Around three fourth (72.5%) were nonsmokers. More than half of the patients had AVNRT (60%), and almost a quarter had AVRT (31.7%). The mean number of episodes of the fast heart rhythm in the last month was 5.2±3.1, and the mean duration of these symptoms was 33.4±16.2 minutes. Other demographic variables are shown in Table 1.
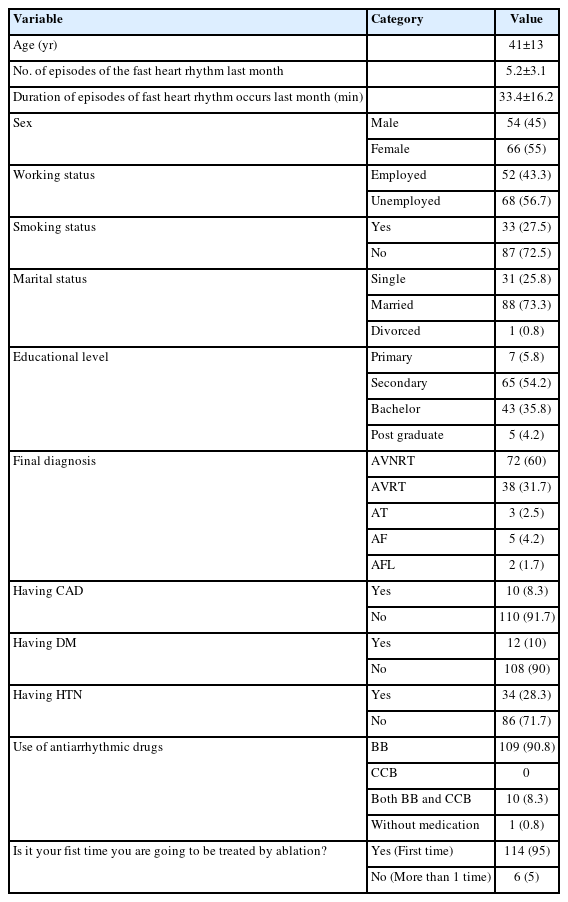
Description of socio-demographics and clinical variables before RFCA (n=120)
Levels of QoL before RFCA and differences in QoL before and after the ablation procedure
Patients with SVT had poor QoL because the total mean score of PCS was (37.4±17.9), MCS (30.6±18.6), and the total of both physical and mental components was (33.7±17.0) which are below 47. Table 2 showed statistically significant differences in all domains of physical and mental components before and after RFCA, indicating an improvement in QoL after the procedure. In addition, the number of episodes of rapid heartbeat attacks last month after ablation decreased from 5.2±3.1 to 0.7±1.1 times. Also, the duration of episodes of these symptoms decreased from 33.4±16.2 to 9.3±14.1 minutes. About 96 (80%) of the patients reported that the procedure met or exceeded their expectations, and only seven patients (5.8%) reported complications post-procedure.
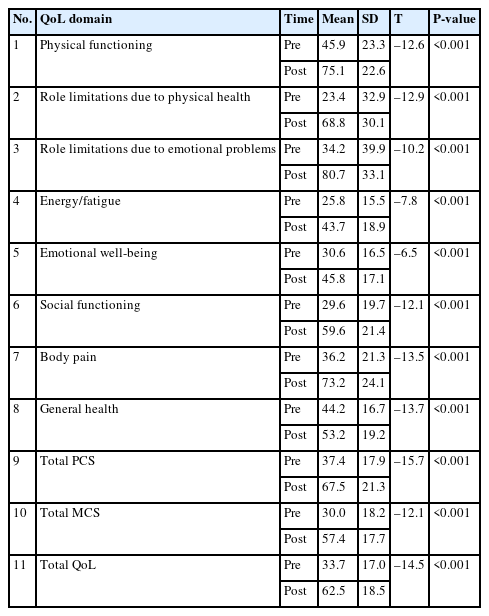
QoL domains before and after the RFCA
Difference in QoL according to the socio-demographic and clinical variables
There was a significant difference in the mean score of QoL based on whether the procedure's outcome met or exceeded patients’ expectations (t=17.47, P<0.001). Patients who reported that the procedure met their expectations had higher QoL (69.0±8.2) than those who did not (23.7±15.7). Also, there was a significant difference in the mean score of QoL based on the complications of the procedure (t=–5.95, P=0.003). Patients experienced complications had lower QoL (27.2±21.6) than those without complications (64.8±15.8). However, there were no significant differences in the mean scores of QoL based on sex, age, marital status, working status, smoking, coronary artery disease (CAD), diabetes mellitus (DM), and hypertension (HTN) after RFCA (Table 3). Also, there was a significant difference in the mean score of QoL based on final diagnosis (t=5.27, P=0.002). Post hock test showed that the mean of AVNRT (67.4) was more than the mean of AVRT (53.4), suggesting that the final diagnosis of the AVNRT category after the ablation procedure has higher QoL than the AVRT category. Results showed that there was a significant relationship between the total score of QoL and the number of episodes (r=–0.072, P<0.01) and duration of episodes (r=–0.777, P<001).
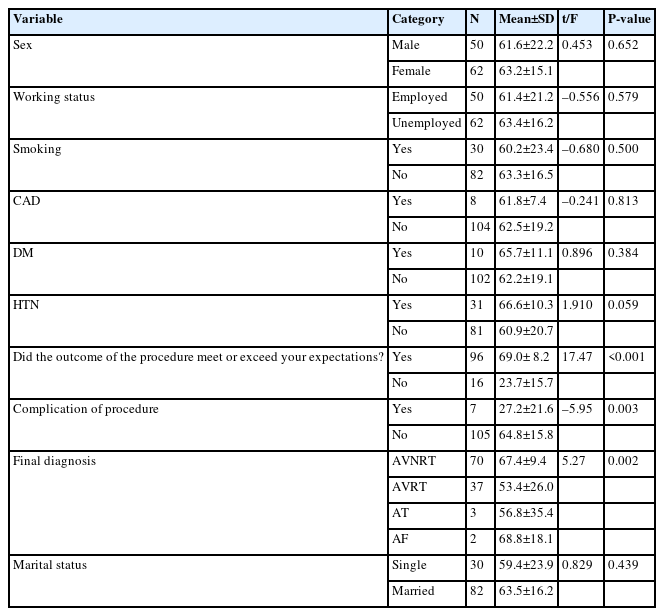
Difference in QoL after RFCA according to the socio-demographic and clinical variables (n=112)
DISCUSSION
Findings of the current study showed that before RFCA, patients reported poor QoL. Moreover, it was reported that the number of episodes of SVT and the duration of SVT episodes were high before the RFCA which affected the QoL for these patients. However, after the procedure there was a significant increase in all domains of QoL compared to baseline. Additionally, the study found that patients who reported that the procedure met/exceeded their expectations and those with fewer complications reported higher QoL than those who did not meet the outcome of the ablation procedure.
The current study showed that before RFCA, patients reported poor QoL. The result of this study was consistent with many studies that have similar characteristics to the present study [15,19,28-30]. Furthermore, the role limitation due to physical health and physical functioning showed the most significant decrease in mean score across all eight components in this study, which was also seen in most literature [16,28,31]. The rationale could be related to the patient’s fear that the episodes will come to them while working and they won't be able to complete the work and the usual daily tasks, and they may be forced to stop all their work. Also, the pain they experienced from the attack interfered with their ability to move freely [19].
The number of episodes of SVT and the duration of SVT episodes were high before the RFCA in the current study, which affected the QoL for these patients. These results were in line with previous literature [32-34]. From the researchers' point of view, the more episodes of SVT, the more impaired they are to do their daily tasks, more visits to the emergency room, and a decrease in their daily activity level. Furthermore, the longer the duration of SVT episodes, the more impaired the roles that rely on physical health and physical functioning and the feeling of being afraid and thinking about the attack, all of which may impact QoL in these SVT patients [33].
In this study, the QoL was assessed before and 1 month after the procedure, and there was a significant increase in all domains compared to baseline. This result is similar to previous studies [16,19,28,29,32-34]. These improvements were further confirmed by the outcomes of SF-36 measurements, according to which patients declared fewer symptoms, limited duration, and decreased frequency of episodes at the second measurement. It is worth noting that previously published research has also documented the statistical superiority of RFCA in improving QoL [5,31,35].
In this study, less than a quarter of the patients reported that they did not meet the expectations of the ablation procedure. The rationale could be related to the complications after the ablation procedure, the remaining use of the antidysrhythmic drugs after the procedure, and the bad experience from the first ablation procedure, which was scheduled to repeat the procedure for a recurrent SVT episode [36].
Results of the current study showed no significant difference in the mean score of QoL based on age, sex, working status, and smoking, as well as co-morbidities like CAD, DM, and HTN of the patients. Previous studies reported different points of view. On one hand, the results were in line with previous studies [33,36]. On the other hand, male sex was significantly associated with less QoL improvement than women after the Greek population's ablation procedure [16]. Also, the results of existing studies are discordant; researchers reported in Poland a higher severity of symptoms in the female sex compared to males, both at baseline and 2 months after the ablation [13].
This study found a significant difference in the mean score of QoL based on whether the outcome of the procedure met or exceeded the expectations. More than three-quarters of patients met their expectations of the ablation procedure. RFCA is considered a safe and effective procedure. This is consistent with much of the literature [5,28,29,35]. The patients who had a successful ablation, declared fewer symptoms, had no complications, resumed working freely without fearing an episode attack of SVT, and had a higher QoL than patients who did not meet the outcome of the ablation procedure.
Findings of this study showed a significant difference in the mean score of QoL based on complications of the ablation procedure and the most common reported complication was hematoma. Previous studies reported that although the ablation procedure had a safe and minimal complication rate, the most common complications were hematoma, pneumothorax, bleeding, unintentional heart block, and vessel trauma, as presented in most literature [35-38].
In this study, there was a significant difference in the mean score of QoL based on the final diagnosis. The AVNRT was associated with a higher QoL post-ablation procedure than other SVT types. This result is consistent with a study that reported a higher QoL among AVNRT than different SVT types [28]. On the other hand, a contrary result was found that SVT type scores' impact was lower for AT patients than for those with AVNRT and AVRT. Although the QoL of patients has improved, patients with AT who had RFCA continued to have symptoms, and their QoL was lower than AVNRT or AVRT patients [36]. Such a difference in the literature could be related to the different mechanisms of AT and AVRT since this type of SVT has more pathways for conduction of the electrical pulse and multiple locations for AT. Also, the duration of ablation procedures for this type of SVT could be longer than AVNRT [39].
The current study showed that age was not related to changes in QoL after the ablation. This is consistent with multiple studies showing that patients having EPS and RFCA for SVTs, regardless of age, have outstanding social, emotional, psychological, and physical ratings, as well as much lower levels of anxiety [18,28,40] However, another study found a contrary result and reported that older patients were more likely to have low QoL and report more symptoms [32].
This study showed a negative relationship between the total score of QoL and the number and duration of SVT episodes. Patients who suffer from recurrent and frequent arrhythmia episodes have a poor QoL after ablation because they never know when the next attack will occur. Many researchers reported similar results [13,16,29,31,34]. It might be expected to have a low QoL for patients with SVT related to recurrent episodes and long-term episodes. These interferences in patients' daily lives include deteriorated living situations, reduced physical ability, inability to work and perform daily activities tasks, and the avoidance of planning for many things like travel or leisure activities.
SVT is a common tachyarrhythmia that causes low QoL in multiple dimensions. The current study found that QoL was low at baseline for patients with SVT. Therefore, the pre-ablation procedure level of QoL should be assessed and considered in deciding to go for it, as well as psychological indicators and physical outcomes. Furthermore, the current study found a statistically significant difference in QoL post-RFCA. Therefore, post-ablation QoL level should be assessed and measured as a short and long-term outcome for this procedure. Interventions to improve QoL and decrease the incidence of attack episodes of SVT should be included in planning for the care of patients post RFCA procedure. The associated factors that affect QoL should be considered and assessed based on a guideline or protocol to detect these outcomes and work on preventing deterioration in QoL post-ablation.
The short follow-up time in the current study was one of the limitations. Nonetheless, it has been documented that the RFCA improves QoL in patients with SVT. As a result, this study included a short follow-up duration to prevent recall bias in observational studies with longer follow-up periods. On the other hand, the literature supported a short-term follow-up period of 1 to 6 months. It is recommended that you follow up in the medium and long term. As a result, any dysrhythmic episodes that occurred after that time went unnoticed. A convenience sampling technique and a self-reported questionnaire for data collection could affect the generalizability of the results to some extent.
Data was collected from one of Jordan's largest specialized cardiac health centers. Although this center offers cardiac health treatment to many cardiac disease patients in Jordan and other countries, other Jordanian centers should be included in future research. So, this could limit the generalizability of the results.
The findings of this study added to the expanding body of evidence that supports the critical role of healthcare providers in improving QoL levels after RFCA, identifying variables that impact QoL, and minimizing complications that impair QoL. Because most patients will have stopped using antidysrhythmic drugs by the time they arrive, monitoring for cardiac arrhythmias should be a priority. Moreover, educational and training programs related to management skills will provide a high QoL for these patients. The programs' goals would be to enhance patients' understanding of disease-specific arrhythmia issues, improve patients' ability to self-care, reduce arrhythmia burden, reduce patients' worry and anxiety about arrhythmia, as well as improve QoL.
The EPS clinic and physicians must inform the patients of the benefits of EPS and RFCA while also reassuring them about the procedure's safety. For some patients, medical therapy alone may appear to be a more attractive option, but elucidating the long-term adverse events of medical treatment, especially the negative impact on one’s physical well-being and social life, will further strengthen the case in favor of EPS and RFCA.
KEY MESSAGES
▪ Cardiac ablation contributes to improvement in quality of life in patient with heart diseases.
▪ Patients should be informed about the benefits and safety of cardiac ablation.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualization: MTA, RM, HB, MEA. Methodology: MTA. Formal analysis: RM, SHH. Data curation: MTA. Writing–original draft: MTA, RM, SHH. Writing–review & editing: SHH, HB, MEA.
Acknowledgements
The authors are grateful to the Applied Science Private University, Amman, Jordan, for the research award granted to this research project.