Vitamin C and corticosteroids in viral pneumonia
Article information

Dear Editor:
The current coronavirus disease 2019 (COVID-19) pandemic has re-ignited interest in using adjunctive agents—including corticosteroids and vitamin C—to attenuate the severity of viral pneumonia and acute lung injury [1,2]. Although the efficacy of dexamethasone on COVID-19 seems convincing, the role of corticosteroids with and without vitamin C in other viral pneumonia remains contentious and unclear. We hypothesised that high dose intravenous vitamin C (6 g/day) used in conjunction with corticosteroids could improve oxygenation in non–COVID-19 viral pneumonia.
The 2019 winter season was expected to have a significant outbreak of influenza pneumonia, and in planning for this, the intensive care unit (ICU) clinicians at the Sir Charles Gairdner Hospital decided that based on the favourable safety profile and potential benefit of vitamin C, it could be provided to any patients with presumed severe viral pneumonia based on the combination of the prodromal symptoms, acute onset, and bilateral (non-consolidative) infiltrates on chest X-rays, at the discretion of the treating clinician. Intravenous vitamin C (Rotexmedica, Trittau, Germany; 1.5 g four times a day [qid] for 72 hours) was administered within 12 hours of admission. The dose was extrapolated from that used in previous studies [3]. Hydrocortisone (50 mg qid) was also given for those who vasopressor-dependent shock until clinical improvement. The patients with presumed viral pneumonia who were not given either vitamin C or corticosteroids were used as a comparator group. Hypothesising that, if vitamin C was to have an effect on oxygenation, it would occur within 24 hours, the primary outcome was difference in arterial oxygen tension (PaO2) to inspired oxygen concentration (FiO2) ratio (P/F ratio) in the 24 hours following the administration of vitamin C. Secondary outcomes were mortality, length of mechanical ventilation and ICU stay. Study design and data collection was prospective.
Table 1 outlines the demographic and clinical characteristics of the 16 patients. There was no significant difference in Acute Physiology and Chronic Health Evaluation (APACHE) II between groups receiving corticosteroids or vitamin C. Nine and seven patients were invasively and noninvasively ventilated, respectively, 11 (69%) required vasopressor support, 9 (56%) received vitamin C, 11 (69%) received corticosteroids, and 7 (44%) received both agents. Influenza A, influenza B and respiratory syncytial virus were detected by viral polymerase chain reaction in seven, one, and four patients, respectively. Fourteen patients (88%) received oseltamivir, and seven patients had concomitant bacterial or fungal pathogens detected in their sputum samples and were treated accordingly.
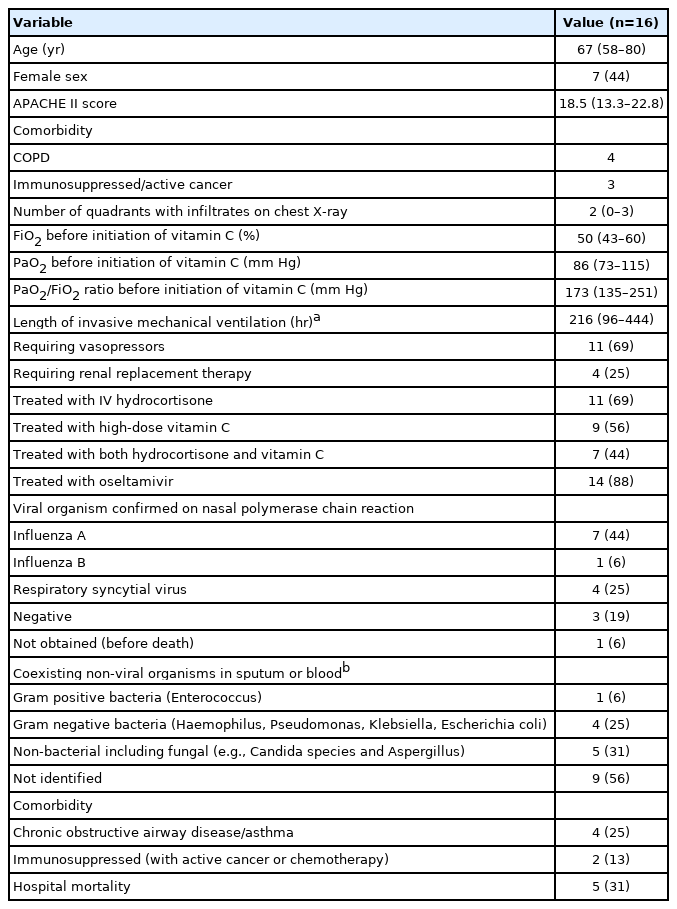
Characteristics of the patients
There was no statistically significant difference in the P/F ratio in the first 24 hours between those who received and not received vitamin C. The P/F ratios within the first 24 hours between those who received both vitamin C and corticosteroids and those who did not receive both agents were also not significantly different (P = 0.860), but the post-hoc comparison of PF ratios between the two groups at 24 hours were significantly different (P = 0.039) (Figure 1). Five patients (31%) died in hospital and there was a significant difference in survival between those who received corticosteroids (10/11 survived) and those who did not (1/5, unadjusted chi-square test: P = 0.001; after adjustment by multiple permutations: chi-square test: 8.045, P = 0.012), whereas use of vitamin C alone (6/9 survived) or both agents (6/7 survived) did not reach significance in survival compared to no vitamin C or not using both agents, respectively. Length of mechanical ventilation or duration of ICU stay was not statistically different between the groups received both vitamin C and corticosteroids, and without both, or between patients received vitamin C alone and those without vitamin C.

Comparison in PaO2/FiO2 ratio over time (at baseline, 6 hours, and 24 hours) between the groups who received vitamin C (Vit C) and corticosteroids and those who did not for viral pneumonia. PaO2: arterial oxygen tension; FiO2: inspired oxygen concentration.
This small prospective cohort study showed that corticosteroids may be useful for patients with viral pneumonia other than COVID-19 [1], and administration of vitamin C alone did not improve oxygenation in patients with viral pneumonia, consistent with previous studies [4]. It is possible that a higher dose of vitamin C may offer more benefits than the dose that we used, or it works only when combined with corticosteroids as shown in our post-hoc analysis [5]. Nonetheless, this was not a randomised-controlled study and our results could be, at least in part, explained by type I error and confounding. Furthermore, the viral pathogens were not the same for all patients, making generalisability difficult. In summary, our results showed that corticosteroids might also be effective for viral pneumonia other than COVID-19, but vitamin C was not. However, an adequately powered randomised-controlled trial is needed to assess whether adding vitamin C to corticosteroids will improve oxygenation in viral pneumonia.
Approval for the study was granted as a quality improvement project for monitoring of outcomes of patients with presumed viral pneumonia admitted to the intensive care (SCGH # 32985), with a waiver for ethics approval.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.