Articles
- Page Path
- HOME > Acute Crit Care > Volume 35(2); 2020 > Article
- Case Report Right ventricular assist device with an oxygenator using extracorporeal membrane oxygenation as a bridge to lung transplantation in a patient with severe respiratory failure and right heart decompensation
-
Dong Kyu Oh1
 , Tae Sun Shim1, Kyung-Wook Jo1, Seung-Il Park2, Dong Kwan Kim2, Sehoon Choi2, Geun Dong Lee2, Sung-Ho Jung2, Pil-Je Kang2, Sang-Bum Hong1
, Tae Sun Shim1, Kyung-Wook Jo1, Seung-Il Park2, Dong Kwan Kim2, Sehoon Choi2, Geun Dong Lee2, Sung-Ho Jung2, Pil-Je Kang2, Sang-Bum Hong1 -
Acute and Critical Care 2019;35(2):117-121.
DOI: https://doi.org/10.4266/acc.2018.00416
Published online: April 8, 2019
1Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
2Department of Thoracic and Cardiovascular Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- Corresponding author Sang-Bum Hong Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea Tel: +82-2-3010-3893 Fax: +82-2-3010-6968 E-mail: hongsangbum@gmail.com
Copyright © 2020 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
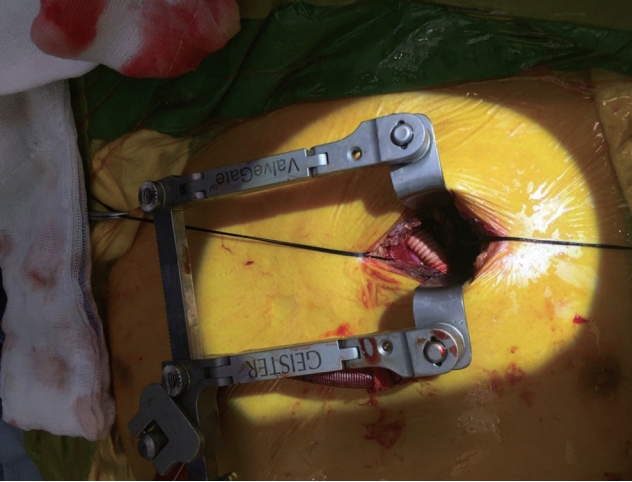
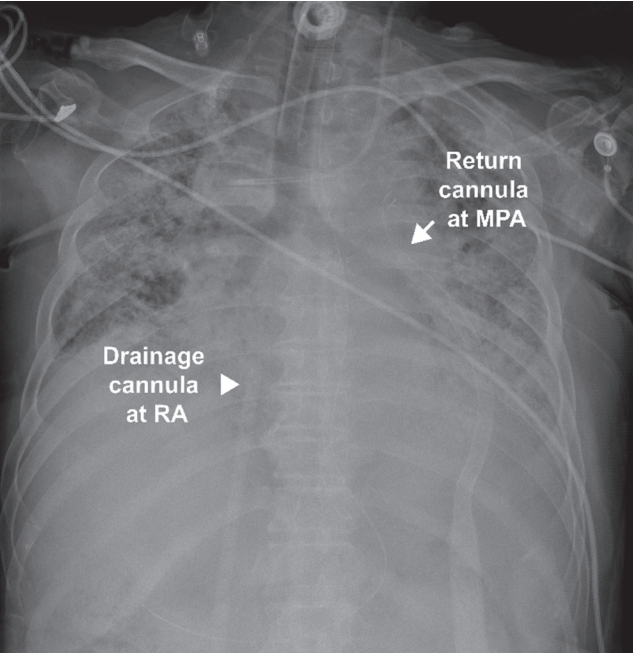
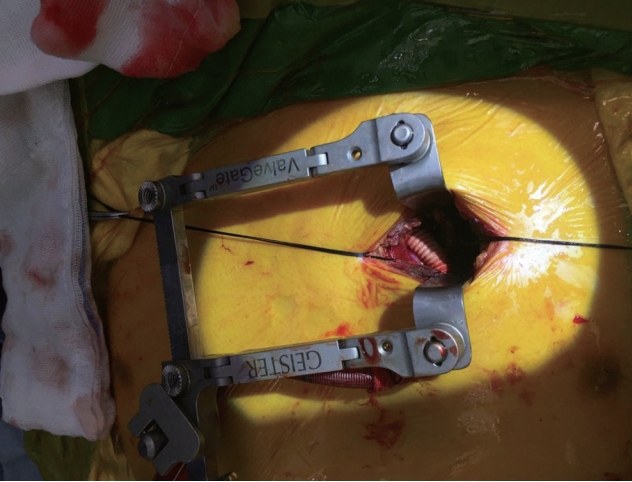
- Right heart decompensation is a fatal complication in patients with respiratory failure, particularly in those transitioned to lung transplantation using veno-venous extracorporeal membrane oxygenation (V-V ECMO). In these patients, veno-arterial (V-A ECMO) or veno-arterial-venous extracorporeal membrane oxygenation (V-AV ECMO) is used to support both cardiac and respiratory function. However, these processes may increase the risk of device-related complications such as bleeding, thromboembolism, and limb ischemia. In the present case, a 64-year-old male patient with idiopathic pulmonary fibrosis developed respiratory failure and commenced treatment with V-V ECMO as a bridge to lung transplantation. Unfortunately, the patient developed right heart decompensation and required both cardiac and respiratory support during treatment with V-V ECMO. Instead of adding arterial cannulation, he was switched to a novel configuration, a right ventricular assist device with an oxygenator (Oxy-RVAD) using ECMO, with drainage cannulation from the femoral vein and return cannulation to the main pulmonary artery. The patient was successfully bridged to lung transplantation without serious complications after 10 days of Oxy-RVAD support. To the best of our knowledge, this is an extreme rare and challenging case of Oxy-RVAD using ECMO in a patient successfully bridged to lung transplantation.
CASE REPORT
DISCUSSION
-
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: all. Data curation: all. Formal analysis: DKO, SBH. Methodology: DKO, SBH. Project administration: DKO, SBH. Visualization: DKO, SBH. Writing - original draft: DKO, SBH. Writing - review & editing: all.
NOTES

V-V ECMO: veno-venous extracorporeal membrane oxygenation; Oxy-RVAD: right ventricular assist device with an oxygenator; ICU: intensive care unit; TR: tricuspid valve regurgitation; DTI: doppler tissue imaging; S’: tricuspid lateral annulus doppler tissue imaging tricuspid annular peak systolic velocity; BNP: brain natriuretic peptide; AST: aspartate transaminase; ALT: alanine transaminase.
- 1. Kotloff RM, Thabut G. Lung transplantation. Am J Respir Crit Care Med 2011;184:159-71.ArticlePubMed
- 2. Valapour M, Skeans MA, Heubner BM, Smith JM, Schnitzler MA, Hertz MI, et al. OPTN/SRTR 2012 annual data report: lung. Am J Transplant 2014;14 Suppl 1:139-65.ArticlePubMed
- 3. Chiumello D, Coppola S, Froio S, Colombo A, Del Sorbo L. Extracorporeal life support as bridge to lung transplantation: a systematic review. Crit Care 2015;19:19. ArticlePubMedPMCPDF
- 4. Bunge JJ, Caliskan K, Gommers D, Reis Miranda D. Right ventricular dysfunction during acute respiratory distress syndrome and veno-venous extracorporeal membrane oxygenation. J Thorac Dis 2018;10(Suppl 5):S674-S82.ArticlePubMedPMC
- 5. Makdisi G, Wang IW. Extra corporeal membrane oxygenation (ECMO) review of a lifesaving technology. J Thorac Dis 2015;7:E166-76.PubMedPMC
- 6. Hoffman M, Chaves G, Ribeiro-Samora GA, Britto RR, Parreira VF. Effects of pulmonary rehabilitation in lung transplant candidates: a systematic review. BMJ Open 2017;7(2):e013445.ArticlePubMedPMC
- 7. Mohite PN, Sabashnikov A, De Robertis F, Popov AF, Simon AR. Oxy-RVAD: rescue in pulmonary complications after LVAD implantation. Perfusion 2015;30:596-9.ArticlePubMed
- 8. Noly PE, Kirsch M, Quessard A, Leger P, Pavie A, Amour J, et al. Temporary right ventricular support following left ventricle assist device implantation: a comparison of two techniques. Interact Cardiovasc Thorac Surg 2014;19:49-55.ArticlePubMedPDF
- 9. Biscotti M, Bacchetta M. The “sport model”: extracorporeal membrane oxygenation using the subclavian artery. Ann Thorac Surg 2014;98:1487-9.ArticlePubMed
- 10. Gregoric ID, Chandra D, Myers TJ, Scheinin SA, Loyalka P, Kar B. Extracorporeal membrane oxygenation as a bridge to emergency heart-lung transplantation in a patient with idiopathic pulmonary arterial hypertension. J Heart Lung Transplant 2008;27:466-8.ArticlePubMed
- 11. Seeger W, Adir Y, Barberà JA, Champion H, Coghlan JG, Cottin V, et al. Pulmonary hypertension in chronic lung diseases. J Am Coll Cardiol 2013;62(25 Suppl):D109-16.ArticlePubMed
References
Figure & Data
References
Citations
- The Role of Palliative Care in Cardiovascular Disease
John Arthur McClung, William H. Frishman, Wilbert S. Aronow
Cardiology in Review.2024;[Epub] CrossRef - Percutaneous Venopulmonary Extracorporeal Membrane Oxygenation as Bridge to Lung Transplantation
Asad Ali Usman, Audrey Elizabeth Spelde, Wasim Lutfi, Jacob T. Gutsche, William J. Vernick, Omar Toubat, Salim E. Olia, Edward Cantu, Andrew Courtright, Maria M. Crespo, Joshua Diamond, Mauer Biscotti, Christian A. Bermudez
ASAIO Journal.2024;[Epub] CrossRef - Right Ventricular Assist Device with an Oxygenator for the Management of Combined Right Ventricular and Respiratory Failure: A Systematic Review.
Juliette Beaulieu, Christine Vu, Sanjog Kalra, Hamza Ouazani Chahdi, Julie Cousineau, Alexis Matteau, Samer Mansour, E. Marc Jolicoeur, Sabrina Jacques, Bénédicte Nauche, Renata Podbielski, Pasquale Ferraro, Charles Poirier, Brian J. Potter
Canadian Journal of Cardiology.2024;[Epub] CrossRef - Early Mobilization for a Patient With a Right Ventricular Assist Device With an Oxygenator
Sheena MacFarlane, Vanessa Lee, Adrienne H. Simonds, Samantha Alvarez, Samantha Carty, Kevin H. Ewers, Victoria R. Kelly, Parker Linden, Amanda L. Moskal
Journal of Acute Care Physical Therapy.2023; 14(1): 45. CrossRef - A 35-month-old boy who ingested laundry detergent pods and underwent veno-pulmonary extracorporeal membrane oxygenation support
Hye-ji Han, Bongjin Lee, Won Jin Jang, Ji Won Lee, Jin Hee Kim, Sungkyu Cho, June Dong Park
Pediatric Emergency Medicine Journal.2023; 10(4): 175. CrossRef - Right Ventricular Assist Device With Extracorporeal Membrane Oxygenation for Bridging Right Ventricular Heart Failure to Lung Transplantation: A Single-Center Case Series and Literature Review
Jae Guk Lee, Chuiyong Pak, Dong Kyu Oh, Ho Cheol Kim, Pil-Je Kang, Geun Dong Lee, Se Hoon Choi, Sung-Ho Jung, Sang-Bum Hong
Journal of Cardiothoracic and Vascular Anesthesia.2022; 36(6): 1686. CrossRef - Advanced Circulatory Support and Lung Transplantation in Pulmonary Hypertension
Marie M. Budev, James J. Yun
Cardiology Clinics.2022; 40(1): 129. CrossRef - A Review of Pulmonary Arterial Hypertension Treatment in Extracorporeal Membrane Oxygenation: A Case Series of Adult Patients
Heather Torbic, Benjamin Hohlfelder, Sudhir Krishnan, Adriano R. Tonelli
Journal of Cardiovascular Pharmacology and Therapeutics.2022; 27: 107424842110690. CrossRef - A Comprehensive Review of Mechanical Circulatory Support Devices
Varunsiri Atti, Mahesh Anantha Narayanan, Brijesh Patel, Sudarshan Balla, Aleem Siddique, Scott Lundgren, Poonam Velagapudi
Heart International.2022; 16(1): 37. CrossRef - Comprehensive Monitoring in Patients With Dual Lumen Right Atrium to Pulmonary Artery Right Ventricular Assist Device
Asad A. Usman, Audrey E. Spelde, Michael Ibrahim, Marisa Cevasco, Christian Bermudez, Emily MacKay, Sameer Khandhar, Wilson Szeto, William Vernick, Jacob Gutsche
ASAIO Journal.2022; 68(12): 1461. CrossRef - Percutaneous Pulmonary Artery Cannulation to Treat Acute Secondary Right Heart Failure While on Veno-venous Extracorporeal Membrane Oxygenation
Kelly M. Ivins-O’Keefe, Michael S. Cahill, Arthur R. Mielke, Michal J. Sobieszczyk, Valerie G. Sams, Phillip E. Mason, Matthew D. Read
ASAIO Journal.2022; 68(12): 1483. CrossRef - The ProtekDuo for percutaneous V-P and V-VP ECMO in patients with COVID-19 ARDS
Ahmed M El Banayosy, Aly El Banayosy, Joseph M Brewer, Mircea R Mihu, Jaclyn M Chidester, Laura V Swant, Robert S Schoaps, Ammar Sharif, Marc O Maybauer
The International Journal of Artificial Organs.2022; 45(12): 1006. CrossRef - Critical Care Management of the Patient with Pulmonary Hypertension
Christopher J. Mullin, Corey E. Ventetuolo
Clinics in Chest Medicine.2021; 42(1): 155. CrossRef - Successful Lung Transplantation After 213 Days of Extracorporeal Life Support: Role of Oxygenator-Right Ventricular Assist Device
Jae Kyeom Sim, Kyeongman Jeon, Gee Young Suh, Suryeun Chung, Yang Hyun Cho
ASAIO Journal.2021; 67(7): e127. CrossRef - Oxy-right Ventricular Assist Device for Bridging of Right Heart Failure to Lung Transplantation
Sung Kwang Lee, Do Hyung Kim, Woo Hyun Cho, Hye Ju Yeo
Transplantation.2021; 105(7): 1610. CrossRef - Interventional and Surgical Treatments for Pulmonary Arterial Hypertension
Tomasz Stącel, Magdalena Latos, Maciej Urlik, Mirosław Nęcki, Remigiusz Antończyk, Tomasz Hrapkowicz, Marcin Kurzyna, Marek Ochman
Journal of Clinical Medicine.2021; 10(15): 3326. CrossRef - Intraoperative Management of Adult Patients on Extracorporeal Membrane Oxygenation: an Expert Consensus Statement From the Society of Cardiovascular Anesthesiologists—Part I, Technical Aspects of Extracorporeal Membrane Oxygenation
Michael A. Mazzeffi, Vidya K. Rao, Jeffrey Dodd-o, Jose Mauricio Del Rio, Antonio Hernandez, Mabel Chung, Amit Bardia, Rebecca M. Bauer, Joseph S. Meltzer, Sree Satyapriya, Raymond Rector, James G. Ramsay, Jacob Gutsche
Journal of Cardiothoracic and Vascular Anesthesia.2021; 35(12): 3496. CrossRef - Intraoperative Management of Adult Patients on Extracorporeal Membrane Oxygenation: An Expert Consensus Statement From the Society of Cardiovascular Anesthesiologists—Part I, Technical Aspects of Extracorporeal Membrane Oxygenation
Michael A. Mazzeffi, Vidya K. Rao, Jeffrey Dodd-o, Jose Mauricio Del Rio, Antonio Hernandez, Mabel Chung, Amit Bardia, Rebecca M. Bauer, Joseph S. Meltzer, Sree Satyapriya, Raymond Rector, James G. Ramsay, Jacob Gutsche
Anesthesia & Analgesia.2021; 133(6): 1459. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite