Abstract
-
Background
- The guidelines recommend the use of dexamethasone 6 mg or an equivalent dose in patients with coronavirus disease 2019 (COVID-19) who require supplemental oxygen. Given that the severity of COVID-19 varies, we investigated the effect of a pulse dose of corticosteroids on the clinical course of critically ill patients with COVID-19.
-
Methods
- This single-center, retrospective cohort study was conducted between September and December 2021, which was when the Delta variant of the COVID-19 virus was predominant. We evaluated the mortality and oxygenation of severe to critical COVID-19 cases between groups that received dexamethasone 6 mg for 10 days (control group) and methylprednisolone 250 mg/day for 3 days (pulse group).
-
Results
- Among 44 patients, 14 and 30 patients were treated with control steroids and pulse steroids, respectively. There was no difference in disease severity, time from COVID-19 diagnosis to steroid administration, or use of remdesivir or antibacterial agents between the two groups. The pulse steroid group showed a significant improvement in oxygenation before and after steroid treatment (P<0.001) compared with the control steroid group (P=0.196). There was no difference in in-hospital mortality (P=0.186); however, the pulse steroid group had a lower mortality rate (23.3%) than the control steroid group (42.9%). There was a significant difference in the length of hospital stay between both two groups (P=0.039).
-
Conclusions
- Pulse steroids showed no mortality benefit but were associated with oxygenation improvement and shorter hospital stay than control steroids. Hyperglycemia should be carefully monitored with pulse steroids.
-
Keywords: COVID-19; dexamethasone; drug pulse therapy; methylprednisolone; steroid
INTRODUCTION
Coronavirus disease 2019 (COVID-19), which is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a disease that causes severe pneumonia and critical acute respiratory failure (ARF) with high mortality [1,2]. COVID-19 has been shown to cause cytokine storm syndrome by elevating proinflammatory cytokine levels and inducing a hyperinflammatory state [3]. Corticosteroids are known to alleviate cytokine storm syndrome and have been suggested as a treatment option for severe and critical COVID-19 [4]. There are a number of various immunologic approaches for treating COVID-19, of which steroids are an important axis.
The 2021 Surviving Sepsis Campaign recommended the use of corticosteroids, particularly dexamethasone, in critical or severe COVID-19 cases [5]. This recommendation is based on the results of the Randomised Evaluation of COVID-19 Therapy (RECOVERY) study [6], wherein the administration of dexamethasone 6 mg for 10 days (defined as a control steroid) improved 28-day mortality in hospitalized patients diagnosed with COVID-19 receiving oxygen or mechanical ventilation. As indicated in this guideline, the group that was administered dexamethasone 6 mg for 10 days had the highest number of cases, and the effect size on 28-day mortality was large, thus leading to this conclusion; however, it is not a definite conclusion about the comparative efficacy of other corticosteroids [5]. Meanwhile, studies using other corticosteroids, such as hydrocortisone [7,8] or methylprednisolone [9], have limited analyses because they were prematurely stopped [10] or showed no clear effect owing to the small number of study participants [11].
A meaningful message from these studies is that the role of corticosteroids is important because COVID-19 pathophysiology involves the overproduction of proinflammatory cytokines, which can lead to vascular hyperpermeability and often triggers ARF [12]. Therefore, corticosteroids are thought to downregulate systemic and pulmonary inflammation, especially in severe cases [13].
Owing to the varying severity of COVID-19 in patients, we believe that it is impossible to uniformly use a conventional corticosteroid, namely, dexamethasone 6 mg, in severe or critical COVID-19. Therefore, we aimed to study how higher doses of corticosteroids might affect the course of severe or critical COVID-19 illness compared with control corticosteroids.
MATERIALS AND METHODS
Study Design
This single-center retrospective cohort study enrolled patients with critical or severe COVID-19 hospitalized and treated in the intensive care unit (ICU) of a tertiary teaching hospital, South Korea. We retrospectively reviewed the medical records of patients who were confirmed positive for SARS-CoV-2 by using reverse transcription polymerase chain reaction (RT-PCR) on nasopharyngeal swabs or sputum samples from September 2021 to December 2021. Currently, the Delta variant of SARS-CoV-2 is prevalent.
This study was approved by the Institutional Review Board of Daegu Catholic University Medical Center (No. CR-22-060). The study was conducted in accordance with the tenets of the Declaration of Helsinki, and the requirement for informed consent was waived owing to the retrospective design of the study.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) age ≥18 years; (2) critical or severe COVID-19 illness using the World Health Organization (WHO) definition [5]: “critical” includes acute respiratory distress syndrome (ARDS) or ARF requiring ventilation, sepsis, or septic shock, and “severe” includes the presence of clinical signs of pneumonia and respiratory rate >30 breaths/min, severe respiratory distress, or oxygen saturation <90% on room air; (3) partial pressure of oxygen in arterial blood/fraction of inspired oxygen ratio (PF ratio) ≤300; (4) SARS-CoV-2 infection confirmation using an RT-PCR assay of upper or lower respiratory samples; (5) presence of bilateral lung infiltration in chest images; (6) admission in the ICU; and (7) administration of corticosteroids.
The exclusion criteria were as follows: (1) patients who refused intubation with a do-not-resuscitate order, (2) patients who died within 24 hours of admission, and (3) patients who did not use corticosteroids or were unable to use corticosteroids (Figure 1).
Use of Corticosteroids
In Korea, a sporadic increase in the incidence of COVID-19 began in September 2021 and then increased rapidly toward the end of 2021 [14]. In total, 44 of the 54 patients hospitalized for COVID-19 pneumonia met the above criteria and were included. If pneumonia was detected on chest radiography and computed tomography (CT) and if the PF ratio was ≤300, an intravenous daily injection of dexamethasone 6 mg was administered for 10 days in accordance with the criteria for critical or severe COVID-19 treatment of the WHO definition while administering oxygen [5]. However, in the case of shock, hydrocortisone 200 mg/day was used in one case, and methylprednisolone was used as a 1 mg/kg daily intravenous injection in four cases. As the number of patients with the Delta variant of SARS-CoV-2 rapidly increased, the incidence of severe pneumonia or critical ARF also increased. From November 2021, methylprednisolone 250 mg was intravenously injected daily for 3 days followed by daily tapering until the 10th day.
Definition of Terms
The control steroid group was defined as the group with 10 days of corticosteroid administration with methylprednisolone ≤1 mg/kg/day or dexamethasone ≤0.2 mg/kg/day. The pulse steroid group was defined as the group administered with 250 mg/day of methylprednisolone for 3 days followed by daily tapering until the 10th day. We checked the steroid starting dose by converting it to the methylprednisolone dose [15] and then checked the period of use and total accumulation dose. The accumulated dose was defined as the sum of the doses of intravenous corticosteroids over the entire period of use. “Pre-steroid” was defined as the time before corticosteroid administration, and “post-steroid” was defined as the 10th day after corticosteroid administration.
We adopted the Berlin definition of ARDS [16] for the hypoxia severity groups in the current study: severe ARDS group, PF ratio of 100 or less; moderate ARDS group, PF ratio of over 100 to 200; mild ARDS group, PF ratio of over 200 to 300; and PF ratio >300, regardless of positive end-expiratory pressure. The length of hospital stay was defined as the interval from the date of hospitalization to the date of death or discharge.
We used the Radiographic Assessment of Lung Edema (RALE) score in the chest X-ray evaluation. The RALE score evaluates the extent and density of alveolar opacities on chest X-ray. The RALE score can be used as a non-invasive monitoring measurement of ARDS severity, response to therapy, and extent of pulmonary edema [17].
Clinical Management
Except for the corticosteroid dose, all treatments were performed identically. The patients received antibiotic treatment and antiviral agents, such as remdesivir. In the case of pulse steroid use, the patients were given pneumocystis pneumonia prophylaxis, preventive anticoagulation, and gastrointestinal (GI) protection. If necessary, renal replacement therapy, high-flow nasal cannula oxygen therapy, mechanical ventilation, extracorporeal membrane oxygenation, and prone positioning were performed.
The patient was placed in a prone position by using awake prone positioning. If the patient cannot tolerate the prone position, the lateral decubitus position was allowed. The target duration of prone positioning was more than 15 hours a day. We counted the time of strict prone positioning, and the sum of those times was defined as the “prone duration.”
Data Assessment
During hospitalization, we investigated the blood tests, vital signs, disease severity classification score such as the Acute Physiology and Chronic Health Evaluation (APACHE) II score, pneumonia severity score such as the CURB-65 (confusion, uremia, respiratory rate, BP, age ≥ 65 years) score, comorbidity, and chest images. Blood gas analysis was performed to determine the PF ratio immediately before corticosteroid administration and on the 10th day after corticosteroid administration. We compared the clinical characteristics, PF ratio, laboratory results, length of hospital stay, and mortality between the control and pulse steroid groups. Our primary outcome was mortality, and the secondary outcomes were the length of hospital stay, oxygen status such as PF ratio, and steroid-related complications.
Statistical Analyses
The results are presented as absolute values and percentages. Continuous variables were not normally distributed; therefore, medians and interquartile ranges were presented. The Mann-Whitney U-test and Pearson’s chi-square test were used to compare the continuous and categorical data between both groups. To identify the risk factors affecting the pulse steroid group, univariate and multivariable logistic regression models were expressed as odds ratios and 95% confidence intervals. Statistical significance was set at P<0.05. Statistical analyses were performed using IBM SPSS ver. 25.0 (IBM Corp.).
RESULTS
Baseline and Steroid-Related Characteristics between the Control and Pulse Steroid Groups
Among the 44 patients, 14 and 30 were treated with control steroids and pulse steroids, respectively. There were no differences in age, CURB-65 score, and APACHE II score between the two groups. There was a significant difference between sex and malignancy as an underlying disease (P=0.005 and P=0.034, respectively). Furthermore, there was no difference between the two groups in the time interval from the onset of dyspnea to hospitalization or in the time interval from the diagnosis of COVID-19 to steroid administration.
There was a difference in the type of steroid used between the two groups. The control steroid group used dexamethasone the most (8 cases, 57.1%), whereas the pulse steroid group used methylprednisolone the most (29 cases, 96.7%) (P<0.001). When the starting dose of steroids was converted into methylprednisolone, the control steroid group had a median dose of 32 mg, and the pulse steroid group had a median dose of 250 mg (P<0.001). The total duration of corticosteroid use was 10 days in the control steroid group and 9 days in the pulse steroid group, with no difference between the two groups. Chest X-ray showed improvement of the RALE score in both groups without statistical difference. Chest CT was performed in 13 patients in the control steroid group and 19 patients in the pulse steroid group. All of them had bilateral pulmonary infiltrates. (Table 1).
ARDS Severity and Laboratory Findings between the Control and Pulse Steroid Groups
There was no statistical difference in ARDS severity between the two groups before steroid use, but severe ARDS (PF ratio ≤100) was more common in the pulse steroid group. In addition, after steroid use, there was no statistically significant difference in the ARDS severity group between the two groups. However, the control steroid group had a moderate ARDS (100< PF ratio ≤ 200) of 50%, whereas the pulse steroid group had a mild ARDS (200< PF ratio ≤300) of 50%.
Vital signs; PF ratio before steroid administration; and laboratory data, including glucose, were not different between the two groups. On the 10th day after steroid administration, the C-reactive protein (CRP), total bilirubin, potassium, and glucose levels were significantly different between the two groups. CRP and glucose levels were significantly higher in the pulse steroid group than in the control steroid group (P=0.021 and P=0.003, respectively), and total bilirubin and potassium levels were significantly lower in the pulse steroid group than in the control steroid group (P=0.003 and P=0.022, respectively) (Table 2).
Changes in ARDS Severity According to the Control and Pulse Steroid Groups
When comparing the ARDS groups before and after steroid treatment in the control steroid group, the severe ARDS group decreased from 35.7% to 14.3%, and the moderate ARDS group decreased from 57.1% to 50.0%; the oxygenation improvement with a PF ratio >300 was 21.4%. However, this difference was not statistically significant (P=0.196). In the pulse steroid group, the severe ARDS group decreased from 50% to 10%, the moderate ARDS group decreased from 43.3% to 23.3%, and the oxygenation improvement with a PF ratio >300 was 16.7%, which was statistically significant (P<0.001) (Figure 2).
Although there was no statistical significance, the pulse steroid group had more improvement in the RALE score than the control group. Figure 3 shows the chest X-ray improvement in three cases between pre- and post-steroid treatment in the pulse steroid group.
Treatment and Prognosis between the Control and Pulse Steroid Groups
All patients were treated with antibiotics and remdesivir, but there was a difference in the use of interleukin-6 receptor antagonist, tocilizumab, and baricitinib between the two groups. Tocilizumab and baricitinib were initially not recommended in the guideline [4] and were not used in some cases because they were not prepared at that time. There was no difference in mechanical ventilation in 28.6% and 20.0% of the two groups, and the median ventilator duration was 18 days in the control steroid group compared with 8 days in the pulse steroid group. There was no statistically significant difference; however, the duration of mechanical ventilation in the control steroid group was longer than that in the pulse steroid group (P=0.063).
There was no difference in in-hospital mortality or 28-day mortality between the two groups (P=0.186 and P=0.390, respectively), but the pulse steroid group had a lower mortality rate (23.3%) than the control steroid group (42.9%). Survival trend was better in the moderate and mild ARDS groups (P=0.088) than in the severe ARDS group (P=0.933). There was a significant difference in the length of hospital stay between the two groups. Therefore, it was confirmed that the hospital stay of the control steroid group was 14 days longer than that of the pulse steroid group at 11 days (P=0.039). There was one case of Candida infection in the blood and two cases of uncontrolled hyperglycemia in the pulse steroid group. There was one case of GI bleeding in the control steroid group. There was no significant difference between the two groups (P=0.295) (Table 3). Regardless of steroid use, the prone position group had a survival rate of 82.1%, which was significantly better than the 50.0% survival rate of the non-prone position group (P=0.025, data not shown).
DISCUSSION
The pulse steroid group did not show a statistically significant improvement in 28-day mortality or in-hospital mortality compared with the control steroid group, but in-hospital mortality was lower in the pulse steroid group than in the control steroid group. According to the current COVID-19 guidelines, systemic corticosteroids should be considered for adults with critical or severe COVID-19, thus indicating that dexamethasone should be used rather than other corticosteroids. If dexamethasone is not available, it is recommended to use other corticosteroids that are equivalent to dexamethasone 6 mg daily for 10 days [5]. This recommendation is based on the RECOVERY study [6], and most meaningful studies known to date and other meta-analyses [11,18,19] support this suggestion. This conclusion was reached because the RECOVERY study had a large effect size. However, some articles [20-22] have discussed the benefits of a higher corticosteroid dose. There was no difference in the 28-day all-cause mortality compared to the usual care or control steroid group [11], but a trend toward improvements, such as ventilator-free days [21] and more days alive without life support [22], was observed. One retrospective cohort study [23] reported that there was a mortality benefit in the group using a moderate-to-high-dose corticosteroid (any dose higher than the low-dose steroid definition below) compared with the group using a low-dose steroid (methylprednisolone <1 mg/kg/day) in patients with critical COVID-19. In a severe COVID-19 pneumonia clinical trial [24], the clinical improvement and survival of patients treated with methylprednisolone 250 mg per day for 3 days were significantly higher than those in the standard care group when steroids were used at the beginning of the early pulmonary phase of illness. This study used the steroid dose most similar to that used in the current study, except that the inclusion criteria were COVID-19 patients with hypoxia excluding ARDS. These above studies used various doses and types of corticosteroids under various clinical conditions. Therefore, although the current guidelines recommend the use of conventional corticosteroids, it is difficult to uniformly apply dexamethasone 6 mg to various COVID-19 severities because of the variety in steroid type, dosage, and administration duration in different studies [11,25].
The meta-analysis by Sterne et al. [11], which was our most referenced study, did not include all data because some studies [7,8,21] were prematurely stopped. Therefore, comparative studies using higher corticosteroids and flexible corticosteroid applications are considered necessary in the future [10]. One study [23] found that using steroids in critical COVID-19 cases was not effective in women who are at a lower risk of death or in those with greater risk or severity, such as cancer, diabetes, and APACHE II >14; therefore, patient characteristics should be assessed before prescribing corticosteroids. Determining which patients to use corticosteroids selectively will remain a challenge in the future.
In this study, in the moderate and mild ARDS groups, the pulse steroid group appeared to have lower in-hospital mortality than the control steroid group (Table 3). Pulse steroid therapy seemed to have a positive effect on the hyperinflammatory state due to COVID-19. However, in the severe ARDS group, there was no difference in mortality according to the steroid dose. COVID-19 related severe ARDS has a high mortality rate from diffuse alveolar damage alone and is a severe hyperinflammatory state with systemic inflammation [12,26]. Given this condition, improving mortality seems to be difficult by using different steroid doses only. Therefore, in Edalatifard et al. [24], the pulse dosing of steroids was used in patients with COVID-19 pneumonia without ARDS.
The most significant point in our study is that improvement in oxygenation appears to be evident in patients with critical or severe COVID-19 (Figure 2). Evidence that corticosteroid use improves hypoxia in non-COVID-19 ARDS has been consistently reported [25,27-30]. In COVID-19 infection, hypoxia is already known as an important sign of poor outcome [31]. However, in COVID-19, many corticosteroid studies have focused on mortality, but only a few studies have reported on hypoxia improvement. A retrospective study [32] reported a significant improvement in oxygenation in severe COVID-19 ARDS by using high-dose dexamethasone (20 mg daily for 5 days followed by 10 mg for 5 days). Although this is another case report, hypoxia improvement and survival were shown in a case using immunosuppressive therapy and steroid half-pulse therapy (methylprednisolone 500 mg for 3 days) in severe COVID-19 pneumonia, especially in the Delta variant of SARS-CoV-2 [33]. This is a very severe case of COVID-19 pneumonia, thus suggesting that the selective use of pulse steroids in COVID-19 pneumonia, which is thought to be a hyperinflammatory state with severe hypoxia, may affect a patient’s hypoxia correction and survival.
In our study, the length of hospital stay was significantly shorter in the pulse steroid group than in the control steroid group. Although the duration of mechanical ventilation was not statistically significant, it was shorter in the pulse steroid group (Table 3). Similar results were found in non-COVID-19 ARDS [28,29,34] and severe COVID-19 cases [23,35], thus suggesting the possibility that steroids may be helpful in disease recovery. For early steroid use (i.e., receiving a steroid dose within the first 48 hours after ICU admission) in the severe COVID-19 study, moderate-to-high steroid doses (any dose higher than low dose) were associated with improved length of ICU stay compared with a low dose of methylprednisolone (<1 mg/kg/day) [23]. The current study may also have shown a decrease in the length of hospital stay because corticosteroids were administered early on the first day (median) after hospitalization.
In our study, the CRP and glucose levels were significantly higher in the pulse steroid group than in the control steroid group. In the Jeronimo study [9], glucose elevation was higher with methylprednisolone use (methylprednisolone 0.5 mg/kg bid) than with placebo, and the systemic inflammatory status, such as CRP, was more evident; these findings were similar to those of the current study. When a high steroid dose is used, caution is required during infection and hyperglycemia.
In conclusion, pulse steroids did not significantly improve mortality compared with control steroids in critical or severe COVID-19 cases. However, the pulse steroid group showed significant improvement in oxygenation and a shorter length of hospital stay than the control steroid group. The glucose levels were higher in the pulse steroid group than in the control steroid group.
This study had several limitations. First, this was a single-center retrospective study, and there are limitations to this observational study. Second, the sample size was small. Third, the fact that the steroid types used in the control steroid group and the pulse steroid group was different can be a problem. It is difficult to exclude the possibility that the minimal mineralocorticoid effect of methylprednisolone has a negative effect on severe pneumonia because of the difference in steroid types between the control and pulse steroid groups. Fourth, in our study, the prone position was implemented when necessary, and interference with the prone position was possible. Finally, the timing of corticosteroid administration has not been studied.
KEY MESSAGES
▪ A pulse dose of methylprednisolone 250 mg a day for 3 days may be associated with oxygenation improvement and shorter hospital stay in critically ill coronavirus disease 2019 (COVID-19) patients.
▪ Hyperglycemia should be carefully monitored with pulse steroid therapy.
NOTES
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: KCK, EJK. Data curation: KJC, SKJ, EJK. Formal analysis: EJK. Methodology: EJK. Project administration: EJK. Visualization: SKJ, EJK. Writing–original draft: EJK. Writing–review & editing: all authors.
Acknowledgments
None.
Figure 1.Flowchart of critical or severe COVID-19 cases with control and pulse steroid groups. COVID-19: coronavirus disease 2019; ICU: intensive care unit; ARDS: acute respiratory distress syndrome.

Figure 2.Changes in the acute respiratory distress syndrome (ARDS) severity of the control and pulse steroid groups, which include patients with critical or severe coronavirus disease 2019 (COVID-19) cases. ARDS severity was adopted from the Berlin definition [16]: severe, PF ratio ≤100; moderate, 100< PF ratio ≤200; mild, 200< PF ratio ≤300. PF ratio, partial pressure of oxygen in arterial blood/fraction of inspired oxygen ratio.
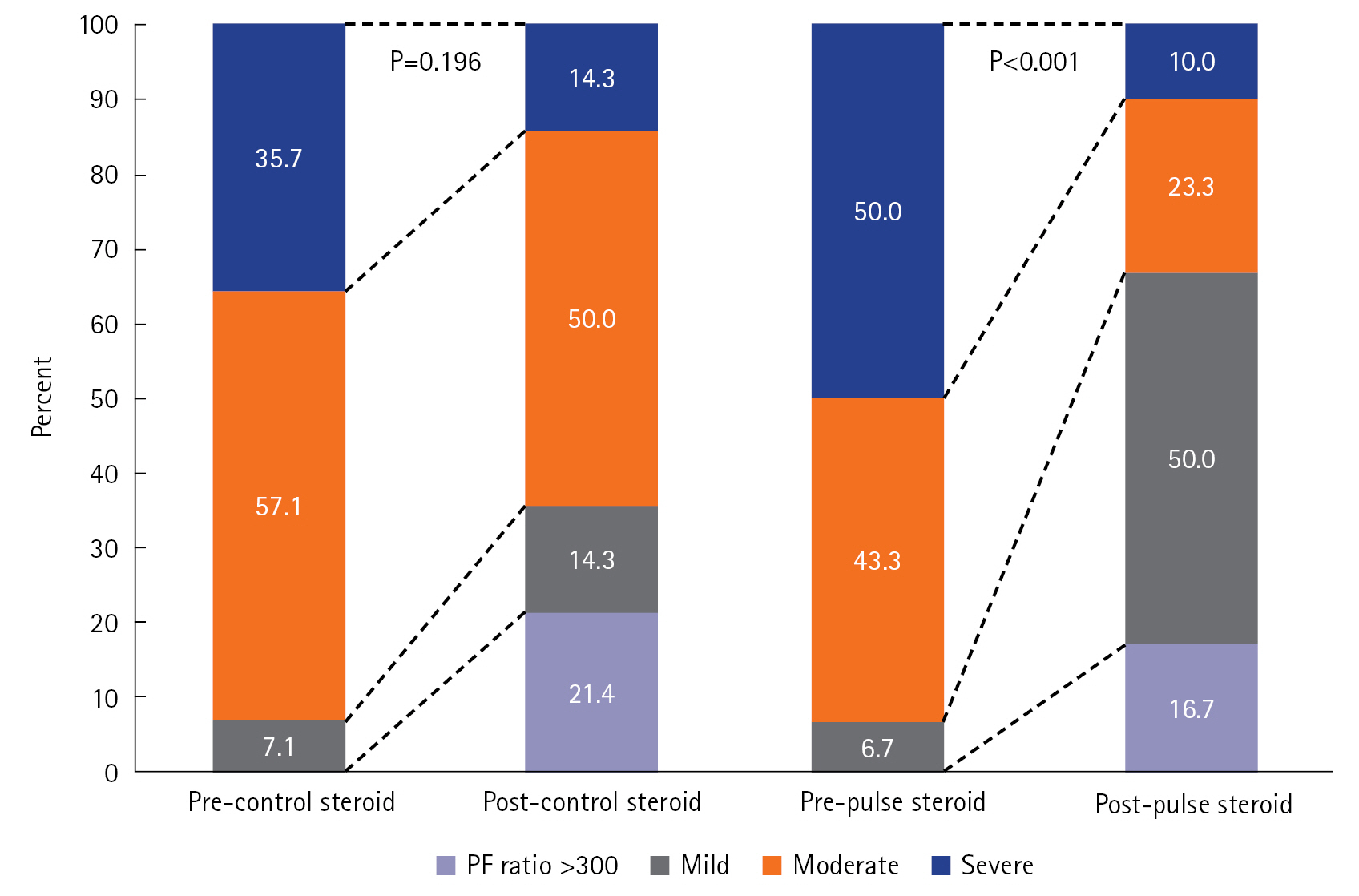
Figure 3.Changes in chest X-ray between pre- and post-steroid treatment in the pulse steroid group. (A-C) These examples were three cases of chest X-ray improvement after pulse steroid administration.

Table 1.Baseline demographic, clinical and steroid-related characteristics of critical or severe COVID-19 cases with control and pulse steroid groups
|
Variable |
Control steroid (n=14) |
Pulse steroid (n=30) |
Total (n=44) |
P-value |
|
Age (yr) |
72 (64–76) |
70 (65–76) |
71 (64–81) |
0.860 |
|
Male:female |
12:2 |
12:18 |
24:20 |
0.005d)
|
|
CURB-65 scorea)
|
1 (1–2) |
2 (1–3) |
1 (1–2) |
0.305 |
|
APACHE II score |
10 (9–14) |
12 (9–15) |
11 (9–15) |
0.383 |
|
Day from symptom onset to hospitalization |
4 (1–8) |
6 (3–7) |
6 (3–8) |
0.541 |
|
Day from dyspnea onset to hospitalization |
1 (1–2) |
1 (1–3) |
1 (1–3) |
0.313 |
|
Day from diagnosis to steroid administration |
1 (0–4) |
1 (0–3) |
1 (0–4) |
0.843 |
|
Day from hospitalization to steroid administration |
1 (0–4) |
1 (0–3) |
1 (0–4) |
0.843 |
|
Type of corticosteroids |
|
|
|
<0.001d)
|
|
Methylprednisolone |
5 (35.7) |
29 (96.7) |
34 (77.3) |
|
|
Dexamethasone |
8 (57.1) |
1 (3.3) |
9 (20.5) |
|
|
Hydrocortisone |
1 (7.1) |
0 |
1 (2.3) |
|
|
Starting doseb) (mg) |
32 (32–62) |
250 (250–272) |
250 (91–267) |
<0.001e)
|
|
Accumulation doseb) (mg) |
465 (352–620) |
1,462 (1,313–1,745) |
1,313 (680–1,635) |
<0.001e)
|
|
Duration of steroid administration (day) |
10 (10–10) |
9 (7–11) |
10 (8–11) |
0.076 |
|
Underlying disease |
|
|
|
|
|
Hypertension |
7 (50.0) |
19 (63.3) |
26 (59.1) |
0.402 |
|
Diabetes mellitus |
3 (21.4) |
8 (26.7) |
11 (25.0) |
0.709 |
|
Cerebrovascular disease |
4 (28.6) |
5 (16.7) |
9 (20.5) |
0.362 |
|
Chronic lung disease |
2 (14.3) |
5 (16.7) |
7 (15.9) |
0.841 |
|
Cardiovascular disease |
1 (7.1) |
3 (10.0) |
4 (9.1) |
0.759 |
|
Chronic liver disease |
2 (14.3) |
1 (3.3) |
3 (6.8) |
0.179 |
|
Malignancy |
2 (14.3) |
0 |
2 (4.5) |
0.034d)
|
|
Immune suppressionc)
|
1 (7.1) |
1 (3.3) |
2 (4.5) |
0.572 |
|
Dementia |
0 |
1 (3.3) |
1 (2.3) |
0.490 |
|
Connective tissue disease |
0 |
1 (3.3) |
1 (2.3) |
0.490 |
|
Chronic kidney disease |
0 |
1 (3.3) |
1 (2.3) |
0.490 |
|
Confusion at hospitalization |
4 (28.6) |
9 (30.0) |
13 (29.5) |
0.923 |
|
Chest X-ray |
|
|
|
|
|
Pre-steroid RALE score |
14 (11–19) |
16 (13–20) |
15 (12–20) |
0.117 |
|
Post-steroid RALE score |
10 (5–12) |
8 (7–11) |
9 (7–12) |
0.919 |
Table 2.ARDS severity and laboratory findings of critical or severe COVID-19 cases with control and pulse steroid groups
|
Variable |
Control steroid (n=14) |
Pulse steroid (n=30) |
Total (n=44) |
P-value |
|
Pre-steroid ARDS severitya)
|
|
|
|
0.666 |
|
Severe |
5 (35.7) |
15 (50.0) |
20 (45.5) |
|
|
Moderate |
8 (57.1) |
13 (43.3) |
21 (47.7) |
|
|
Mild |
1 (7.1) |
2 (6.7) |
3 (6.8) |
|
|
Post-steroid ARDS severitya)
|
|
|
|
0.135 |
|
Severe |
2 (14.3) |
3 (10.0) |
5 (11.4) |
|
|
Moderate |
7 (50.0) |
7 (23.3) |
14 (31.8) |
|
|
Mild |
2 (14.3) |
15 (50.0) |
17 (38.6) |
|
|
PF ratio >300 |
3 (21.4) |
5 (16.7) |
8 (18.2) |
|
|
Pre-steroid PF ratio |
130 (87–150) |
103 (71–130) |
112 (74–140) |
0.166 |
|
Post-steroid PF ratio |
184 (144–277) |
219 (181–253) |
214 (156–257) |
0.496 |
|
Pre-steroid lab |
|
|
|
|
|
Leukocyte (×103/ul) |
9.0 (8.1–11.4) |
9.3 (5.8–12.3) |
9.2 (5.9–12.3) |
0.920 |
|
Neutrophil (%) |
85 (78–92) |
86 (77–93) |
85 (77–93) |
0.830 |
|
Lymphocyte (%) |
7 (4–11) |
8 (3–14) |
8 (4–14) |
0.632 |
|
Hematocrit (%) |
38 (35–44) |
38 (35–39) |
38 (35–39) |
0.427 |
|
Platelet (×103/ul) |
158 (118–224) |
192 (154–219) |
175 (140–223) |
0.231 |
|
CRP (mg/l) |
105 (44–139) |
95 (49–155) |
95 (45–145) |
0.980 |
|
Procalcitonin (ng/ml) |
0.34 (0.10–0.46) |
0.14 (0.08–0.50) |
0.17 (0.08–0.49) |
0.313 |
|
Lactate (mmol/L) |
1.9 (1.5–2.2) |
1.7 (1.3–2.2) |
1.8 (1.3–2.2) |
0.631 |
|
BUN (mg/dl) |
17 (13–23) |
19 (15–25) |
19 (14–25) |
0.715 |
|
Total bilirubin (mg/dl) |
0.6 (0.4–0.8) |
0.5 (0.3–0.8) |
0.5 (0.3–0.8) |
0.315 |
|
Potassium (mmol/L) |
4.1 (3.6–4.8) |
4.1 (3.8–4.3) |
4.1 (3.7–4.4) |
0.920 |
|
Glucose (mg/dl) |
137 (114–210) |
153 (131–184) |
153 (124–201) |
0.900 |
|
Post-steroid lab |
|
|
|
|
|
Leukocyte (103/ul) |
8.8 (5.6–15.5) |
8.1 (6.9–10.2) |
8.7 (6.4–12.0) |
0.579 |
|
Neutrophil (%) |
82 (74–89) |
87 (82–90) |
86 (79–90) |
0.252 |
|
Lymphocyte (%) |
10 (3–15) |
7 (4–12) |
7 (4–13) |
0.435 |
|
Hematocrit (%) |
39 (30–42) |
36 (34–39) |
36 (34–39) |
0.650 |
|
Platelet (×103/ul) |
207 (117–263) |
233 (166–304) |
217 (159–282) |
0.445 |
|
CRP (mg/l) |
4 (1–28) |
16 (6–36) |
12 (4–33) |
0.021b)
|
|
Procalcitonin (ng/ml) |
0.06 (0.02–0.16) |
0.05 (0.03–0.16) |
0.05 (0.02–0.16) |
0.607 |
|
Lactate (mmol/L) |
1.6 (1.2–2.4) |
2.2 (1.8–2.6) |
2.1 (1.5–2.5) |
0.056 |
|
BUN (mg/dl) |
28 (21–29) |
34 (21–35) |
26 (21–35) |
0.910 |
|
Total bilirubin (mg/dl) |
0.8 (0.7–1.0) |
0.6 (0.4–0.7) |
0.7 (0.5–0.9) |
0.003b)
|
|
Potassium (mmol/L) |
4.1 (3.5–4.7) |
3.7 (3.3–3.9) |
3.7 (3.4–4.2) |
0.022b)
|
|
Glucose (mg/dl) |
136 (106–216) |
247 (197–302) |
220 (139–299) |
0.003b)
|
Table 3.Treatment and prognosis in critical or severe COVID-19 cases with control and pulse steroid groups
|
Variable |
Control steroid (n=14) |
Pulse steroid (n=30) |
Total (n=44) |
P-value |
|
High flow nasal cannula oxygen |
14 (100) |
29 (96.7) |
43 (97.7) |
0.490 |
|
Mechanical ventilation |
4 (28.6) |
6 (20.0) |
10 (22.7) |
0.527 |
|
Duration of mechanical ventilation (day) |
18 (11–33) |
8 (4–10) |
10 (6–8) |
0.063 |
|
Other treatmenta)
|
1 (7.1) |
3 (10.0) |
4 (9.1) |
0.759 |
|
Prone positionb)
|
7 (50.0) |
21 (70.0) |
28 (63.6) |
0.199 |
|
In-hospital mortality |
6 (42.9) |
7 (23.3) |
31 (70.5) |
0.186 |
|
In-hospital mortality among moderate and mild ARDS groups |
4 (44.4) |
2 (13.3) |
6 (25.0) |
0.088 |
|
In-hospital mortality among severe ARDS group |
2 (40.0) |
5 (33.3) |
7 (35.0) |
0.933 |
|
28-Day mortality |
5 (35.7) |
7 (23.3) |
32 (72.7) |
0.390 |
|
Cause of death |
|
|
|
0.255 |
|
Respiratory failure |
4 (28.6) |
5 (16.7) |
9 (20.5) |
|
|
Hepatic failure |
2 (14.3) |
0 |
2 (4.5) |
|
|
Arrhythmia |
0 |
1 (3.3) |
1 (2.3) |
|
|
Renal failure |
0 |
1 (3.3) |
1 (2.3) |
|
|
Length of hospital stay (day) |
14 (12–24) |
11 (9–16) |
11 (8–17) |
0.039d)
|
|
Complication after steroid use |
1 (7.1) |
3 (9.9) |
4 (9.0) |
0.295 |
|
Uncontrolled hyperglycemia |
0 |
2 (6.7) |
2 (4.8) |
|
Othersc)
|
1 (7.1) |
1 (3.3) |
2 (4.8) |
References
- 1. Gibson PG, Qin L, Puah SH. COVID-19 acute respiratory distress syndrome (ARDS): clinical features and differences from typical pre-COVID-19 ARDS. Med J Aust 2020;213:54-6.PubMedPMC
- 2. Gattinoni L, Gattarello S, Steinberg I, Busana M, Palermo P, Lazzari S, et al. COVID-19 pneumonia: pathophysiology and management. Eur Respir Rev 2021;30:210138. ArticlePubMedPMC
- 3. England JT, Abdulla A, Biggs CM, Lee AY, Hay KA, Hoiland RL, et al. Weathering the COVID-19 storm: lessons from hematologic cytokine syndromes. Blood Rev 2021;45:100707. ArticlePubMedPMC
- 4. Alhazzani W, Møller MH, Arabi YM, Loeb M, Gong MN, Fan E, et al. Surviving Sepsis Campaign: guidelines on the management of critically ill adults with coronavirus disease 2019 (COVID-19). Intensive Care Med 2020;46:854-87.ArticlePubMedPMCPDF
- 5. Alhazzani W, Evans L, Alshamsi F, Møller MH, Ostermann M, Prescott HC, et al. Surviving Sepsis Campaign guidelines on the management of adults with coronavirus disease 2019 (COVID-19) in the ICU: first update. Crit Care Med 2021;49:e219-34.ArticlePubMed
- 6. RECOVERY Collaborative Group; Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, et al. Dexamethasone in hospitalized patients with COVID-19. N Engl J Med 2021;384:693-704.ArticlePubMedPMC
- 7. Dequin PF, Heming N, Meziani F, Plantefève G, Voiriot G, Badié J, et al. Effect of hydrocortisone on 21-day mortality or respiratory support among critically ill patients with COVID-19: a randomized clinical trial. JAMA 2020;324:1298-306.ArticlePubMedPMC
- 8. Angus DC, Berry S, Lewis RJ, Al-Beidh F, Arabi Y, van Bentum-Puijk W, et al. The REMAP-CAP (Randomized Embedded Multifactorial Adaptive Platform for Community-acquired Pneumonia) Study: rationale and design. Ann Am Thorac Soc 2020;17:879-91.ArticlePubMedPMC
- 9. Jeronimo CM, Farias ME, Val FF, Sampaio VS, Alexandre MA, Melo GC, et al. Methylprednisolone as adjunctive therapy for patients hospitalized with coronavirus disease 2019 (COVID-19; Metcovid): a randomized, double-blind, phase IIb, placebo-controlled trial. Clin Infect Dis 2021;72:e373-81.PubMed
- 10. De Backer D, Azoulay E, Vincent JL. Corticosteroids in severe COVID-19: a critical view of the evidence. Crit Care 2020;24:627. ArticlePubMedPMCPDF
- 11. WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group; Sterne JA, Murthy S, Diaz JV, Slutsky AS, Villar J, et al. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: a meta-analysis. JAMA 2020;324:1330-41.PubMed
- 12. Jose RJ, Manuel A. COVID-19 cytokine storm: the interplay between inflammation and coagulation. Lancet Respir Med 2020;8:e46-7.ArticlePubMed
- 13. Umberto Meduri G, Bell W, Sinclair S, Annane D. Pathophysiology of acute respiratory distress syndrome: glucocorticoid receptor-mediated regulation of inflammation and response to prolonged glucocorticoid treatment. Presse Med 2011;40(12 Pt 2):e543-60.ArticlePubMedPMC
- 14. Jang J, Park SY, Ahn SH, Yang S, Kim SS, Park SB, et al. One-year report of COVID-19 outbreak in the Republic of Korea, January-December 2021. Public Health Wkly Rep 2022;15:225-34.
- 15. Meikle AW, Tyler FH. Potency and duration of action of glucocorticoids: effects of hydrocortisone, prednisone and dexamethasone on human pituitary-adrenal function. Am J Med 1977;63:200-7.PubMed
- 16. ARDS Definition Task Force; Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA 2012;307:2526-33.PubMed
- 17. Warren MA, Zhao Z, Koyama T, Bastarache JA, Shaver CM, Semler MW, et al. Severity scoring of lung oedema on the chest radiograph is associated with clinical outcomes in ARDS. Thorax 2018;73:840-6.ArticlePubMedPMC
- 18. Hasan SS, Kow CS, Mustafa ZU, Merchant HA. Does methylprednisolone reduce the mortality risk in hospitalized COVID-19 patients?: a meta-analysis of randomized control trials. Expert Rev Respir Med 2021;15:1049-55.ArticlePubMed
- 19. Wagner C, Griesel M, Mikolajewska A, Mueller A, Nothacker M, Kley K, et al. Systemic corticosteroids for the treatment of COVID-19. Cochrane Database Syst Rev 2021;8:CD014963. ArticlePubMedPMC
- 20. Villar J, Añón JM, Ferrando C, Aguilar G, Muñoz T, Ferreres J, et al. Efficacy of dexamethasone treatment for patients with the acute respiratory distress syndrome caused by COVID-19: study protocol for a randomized controlled superiority trial. Trials 2020;21:717. ArticlePubMedPMCPDF
- 21. Tomazini BM, Maia IS, Cavalcanti AB, Berwanger O, Rosa RG, Veiga VC, et al. Effect of dexamethasone on days alive and ventilator-free in patients with moderate or severe acute respiratory distress syndrome and COVID-19: the CoDEX randomized clinical trial. JAMA 2020;324:1307-16.ArticlePubMedPMC
- 22. COVID STEROID 2 Trial Group; Munch MW, Myatra SN, Vijayaraghavan BK, Saseedharan S, Benfield T, et al. Effect of 12 mg vs 6 mg of dexamethasone on the number of days alive without life support in adults with COVID-19 and severe hypoxemia: the COVID STEROID 2 randomized trial. JAMA 2021;326:1807-17.PubMed
- 23. Monedero P, Gea A, Castro P, Candela-Toha AM, Hernández-Sanz ML, Arruti E, et al. Early corticosteroids are associated with lower mortality in critically ill patients with COVID-19: a cohort study. Crit Care 2021;25:2. ArticlePubMedPMCPDF
- 24. Edalatifard M, Akhtari M, Salehi M, Naderi Z, Jamshidi A, Mostafaei S, et al. Intravenous methylprednisolone pulse as a treatment for hospitalised severe COVID-19 patients: results from a randomised controlled clinical trial. Eur Respir J 2020;56:2002808. ArticlePubMedPMC
- 25. Chaudhuri D, Sasaki K, Karkar A, Sharif S, Lewis K, Mammen MJ, et al. Corticosteroids in COVID-19 and non-COVID-19 ARDS: a systematic review and meta-analysis. Intensive Care Med 2021;47:521-37.ArticlePubMedPMCPDF
- 26. Buicu AL, Cernea S, Benedek I, Buicu CF, Benedek T. Systemic inflammation and COVID-19 mortality in patients with major noncommunicable diseases: chronic coronary syndromes, diabetes and obesity. J Clin Med 2021;10:1545. ArticlePubMedPMC
- 27. Meduri GU, Headley AS, Golden E, Carson SJ, Umberger RA, Kelso T, et al. Effect of prolonged methylprednisolone therapy in unresolving acute respiratory distress syndrome: a randomized controlled trial. JAMA 1998;280:159-65.ArticlePubMed
- 28. Meduri GU, Golden E, Freire AX, Taylor E, Zaman M, Carson SJ, et al. Methylprednisolone infusion in early severe ARDS: results of a randomized controlled trial. Chest 2007;131:954-63.ArticlePubMed
- 29. Steinberg KP, Hudson LD, Goodman RB, Hough CL, Lanken PN, Hyzy R, et al. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome. N Engl J Med 2006;354:1671-84.ArticlePubMed
- 30. Confalonieri M, Urbino R, Potena A, Piattella M, Parigi P, Puccio G, et al. Hydrocortisone infusion for severe community-acquired pneumonia: a preliminary randomized study. Am J Respir Crit Care Med 2005;171:242-8.ArticlePubMed
- 31. Xie J, Covassin N, Fan Z, Singh P, Gao W, Li G, et al. Association between hypoxemia and mortality in patients with COVID-19. Mayo Clin Proc 2020;95:1138-47.ArticlePubMedPMC
- 32. Vecchié A, Batticciotto A, Tangianu F, Bonaventura A, Pennella B, Abenante A, et al. High-dose dexamethasone treatment for COVID-19 severe acute respiratory distress syndrome: a retrospective study. Intern Emerg Med 2021;16:1913-9.ArticlePubMedPMCPDF
- 33. Muramatsu KI, Ishikawa K, Komatsu A, Jitsuiki K, Yanagawa Y. Severe COVID-19 pneumonia treated by intensive immune suppression therapy with a combination of steroid pulse and tocilizumab followed by a tapering dose of steroid therapy during the Delta (B.1.617.2) variant outbreak: a successfully treated case. Cureus 2021;13:e19340.ArticlePubMedPMC
- 34. Mammen MJ, Aryal K, Alhazzani W, Alexander PE. Corticosteroids for patients with acute respiratory distress syndrome: a systematic review and meta-analysis of randomized trials. Pol Arch Intern Med 2020;130:276-86.ArticlePubMed
- 35. Pinzón MA, Ortiz S, Holguín H, Betancur JF, Cardona Arango D, Laniado H, et al. Dexamethasone vs methylprednisolone high dose for COVID-19 pneumonia. PLoS One 2021;16:e0252057.ArticlePubMedPMC
Citations
Citations to this article as recorded by


 , Soo Kyun Jung
, Soo Kyun Jung

 PubReader
PubReader ePub Link
ePub Link Cite
Cite



