Articles
- Page Path
- HOME > Acute Crit Care > Volume 34(2); 2019 > Article
-
Image in Critical Care
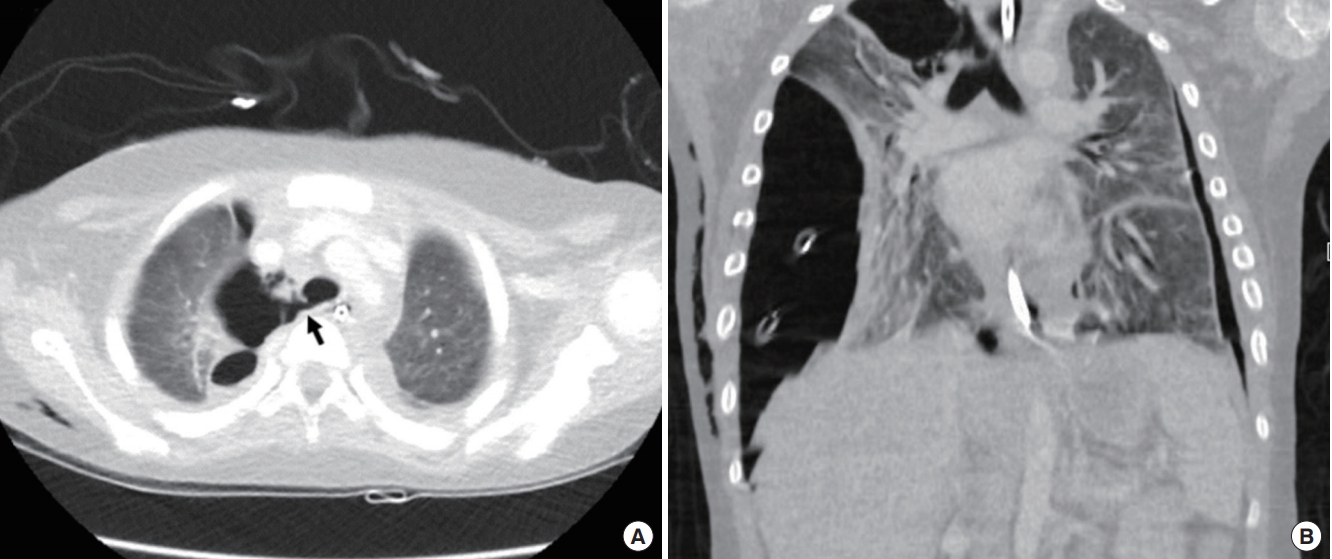
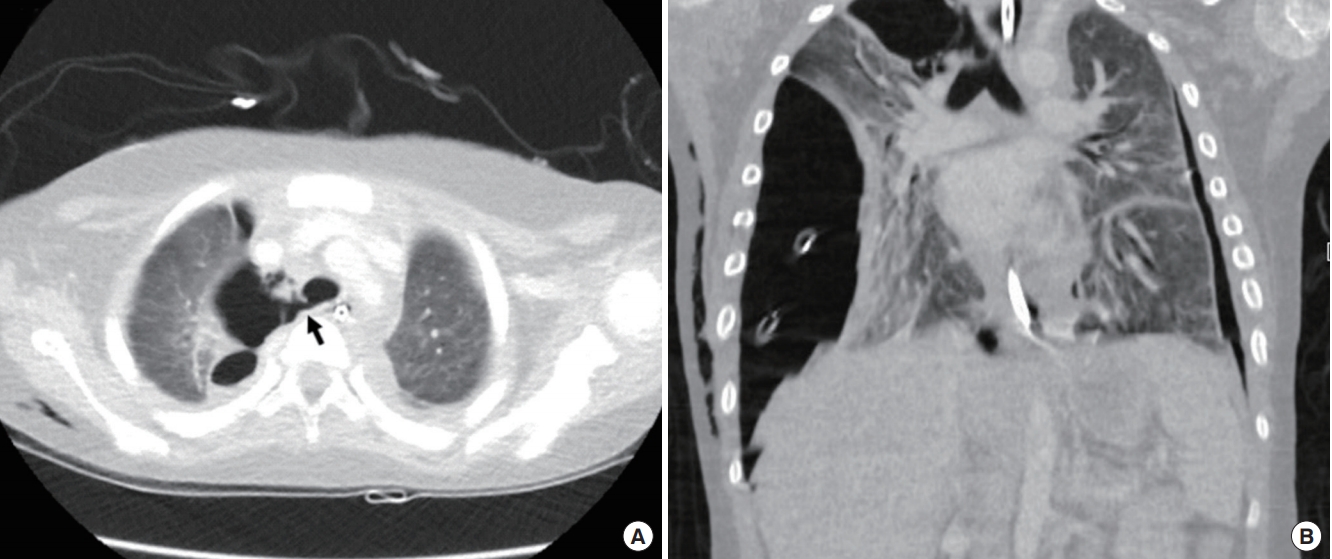
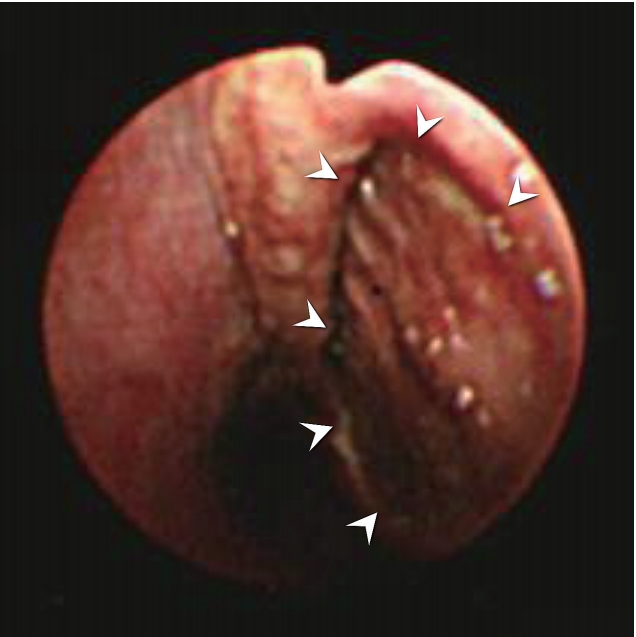
Pulmonary Pneumothorax caused by delayed tracheal rupture in a pediatric patient with acute respiratory distress syndrome -
Minyoung Jung1,2
 , Jong Ho Cho3, Ah Young Choi2, Minji Kim4, Joongbum Cho2
, Jong Ho Cho3, Ah Young Choi2, Minji Kim4, Joongbum Cho2 -
Acute and Critical Care 2019;34(2):170-171.
DOI: https://doi.org/10.4266/acc.2018.00234
Published online: February 7, 2019
1Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
2Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
3Department of Thoracic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
4Department of Pediatrics, Hallym University Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwaseong, Korea
- Corresponding author Joongbum Cho Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea Tel: +82-2-3410-6399 Fax: +82-2-2148-7088 E-mail: joongbum.cho@gmail.com
Copyright © 2019 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,252 Views
- 92 Download
-
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: MJ, JHC, AYC, MK, JC. Data curation: MJ, JHC. Writing original draft: MJ, AYC. Writing-review & editing: MK, JHC, JC.
NOTES
- 1. Hofmann HS, Rettig G, Radke J, Neef H, Silber RE. Iatrogenic ruptures of the tracheobronchial tree. Eur J Cardiothorac Surg 2002;21:649-52.ArticlePubMedPDF
- 2. Schneider T, Storz K, Dienemann H, Hoffmann H. Management of iatrogenic tracheobronchial injuries: a retrospective analysis of 29 cases. Ann Thorac Surg 2007;83:1960-4.ArticlePubMed
- 3. Minambres E, Buron J, Ballesteros MA, Llorca J, Munoz P, Gonzalez-Castro A. Tracheal rupture after endotracheal intubation: a literature systematic review. Eur J Cardiothorac Surg 2009;35:1056-62.ArticlePubMedPDF
- 4. Jabre P, Avenel A, Combes X, Kulstad E, Mazariegos I, Bertrand L, et al. Morbidity related to emergency endotracheal intubation: a substudy of the KETAmine SEDation trial. Resuscitation 2011;82:517-22.ArticlePubMed
- 5. Lim H, Kim JH, Kim D, Lee J, Son JS, Kim DC, et al. Tracheal rupture after endotracheal intubation: a report of three cases. Korean J Anesthesiol 2012;62:277-80.ArticlePubMedPMC
 PubReader
PubReader ePub Link
ePub Link Cite
Cite