Articles
- Page Path
- HOME > Acute Crit Care > Volume 33(2); 2018 > Article
- Image in Critical Care Trauma-Induced Retroperitoneal Paraganglioma Rupture Which Was Misunderstood as a Massive Retroperitoneal Hemorrhage
-
Hongjin Shim1
 , Ji Young Jang1, Yeong Ju Kim2, Jung Soo Lim3, Keum Seok Bae1
, Ji Young Jang1, Yeong Ju Kim2, Jung Soo Lim3, Keum Seok Bae1 -
Acute and Critical Care 2018;33(2):114-116.
DOI: https://doi.org/10.4266/acc.2017.00234
Published online: April 26, 2018
1Department of Surgery, Yonsei University Wonju College of Medicine, Wonju, Korea
2Department of Radiology, Yonsei University Wonju College of Medicine, Wonju, Korea
3Department of Internal Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea
- Keum Seok Bae Department of Surgery, Yonsei University Wonju College of Medicine, 20 Ilsan-ro, Wonju 26426, Korea Tel: +82-33-741-0573 Fax: +82-33-741-0574 E-mail: bksgs@yonsei.ac.kr
• Received: April 1, 2017 • Revised: July 4, 2017 • Accepted: July 5, 2017
Copyright © 2018 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
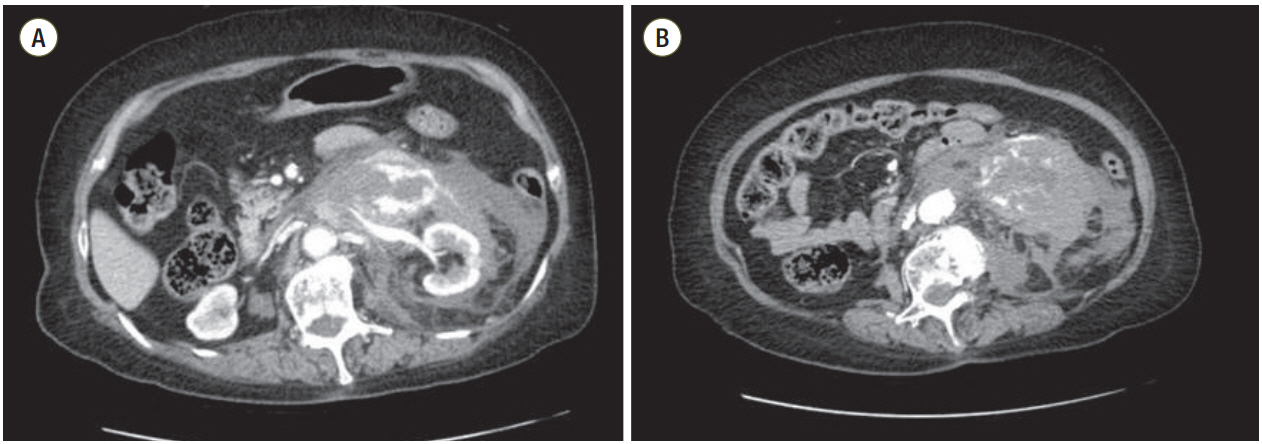
Figure 1.Precontrast views in the initial computed tomography. (A) Retroperitoneal hemorrhage was infiltrated in the left retroperitoneum. (B) A huge mass was not distinguished from the hematoma in the left retroperitoneum.
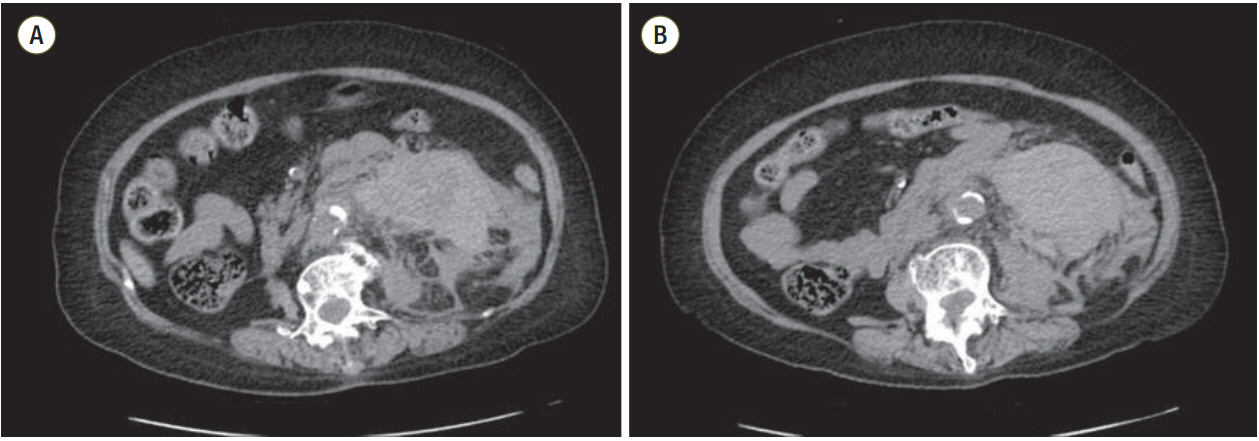
Figure 2.Postcontrast views in the initial abdominal computed tomography. (A) There were several extravasated lesions near the left kidney. (B) Some arteries were supplying to the paraganglioma.

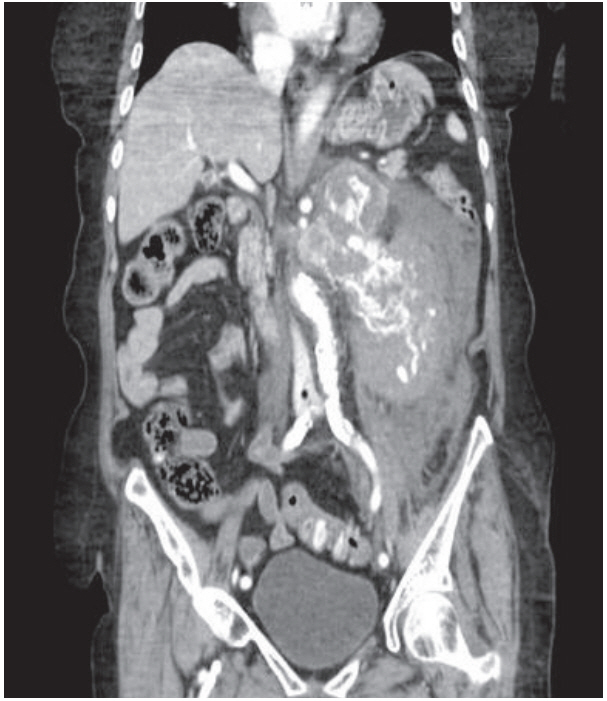
Figure 3.Postcontrast coronal view in the initial abdominal computed tomography: adjacent hemorrhage is masking the perirenal mass; therefore, it is difficult to distinguish from retroperitoneal hematoma.
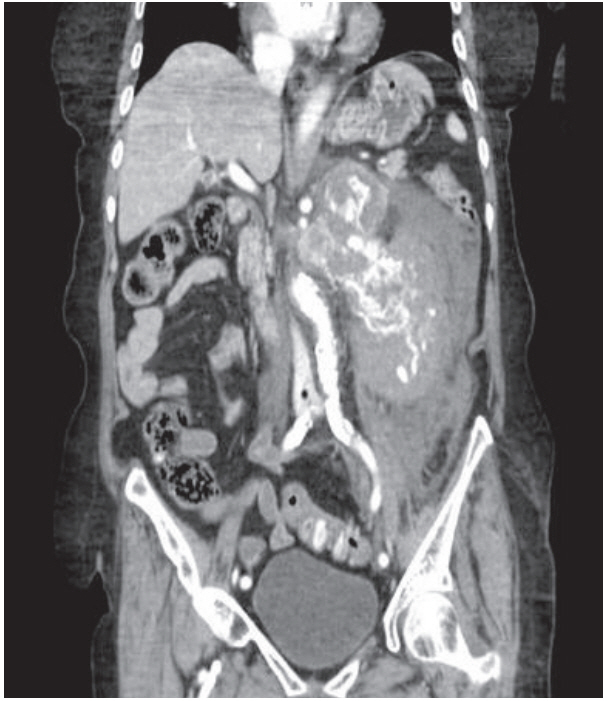
Figure 4.Gross finding of the paraganglioma. There is a lobulated brown solid mass with hemorrhage (arrow) in the soft tissue.

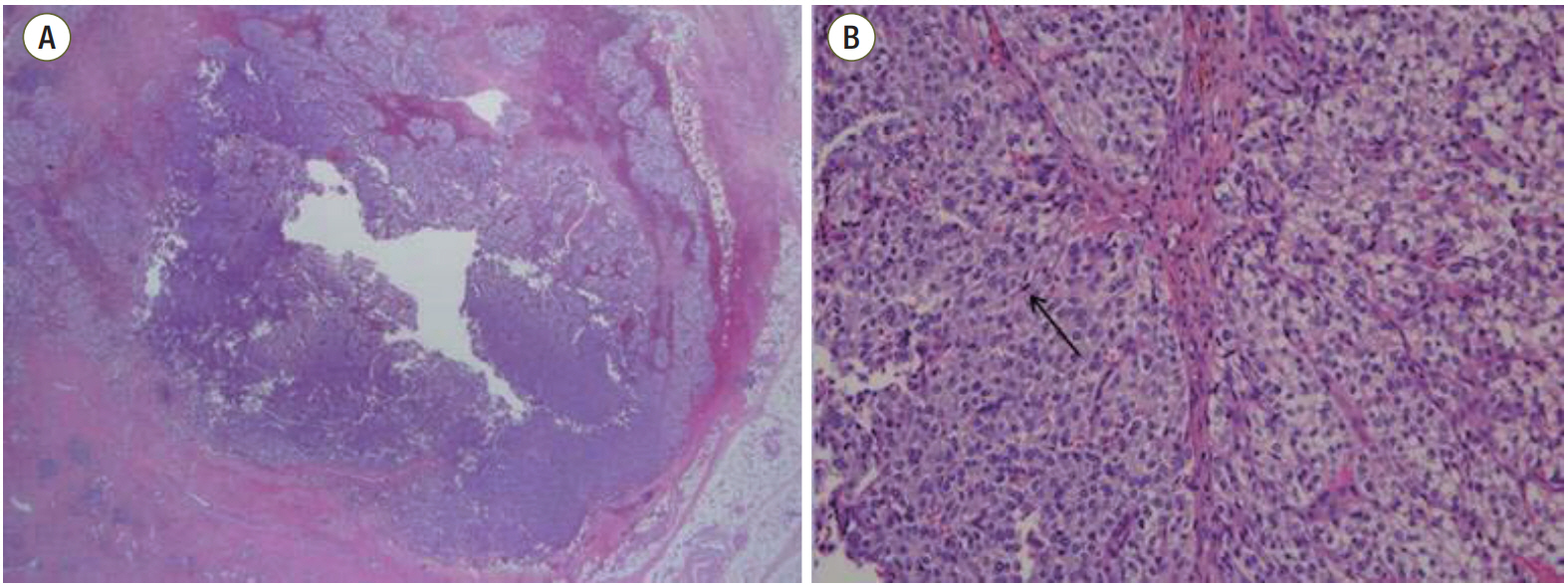
Figure 5.H&E stain. (A) There is a lobulated solid mass with hemorrhage in the soft tissue (×1.25). (B) Histology revealed an alveolar pattern with nest of neoplastic cells surrounded by vascularized connective-tissue septa (×200). Nests outlined by sustentacular cells (arrow). Cells have finely granular basophilic or amphophilic cytoplasm. There was no necrosis.
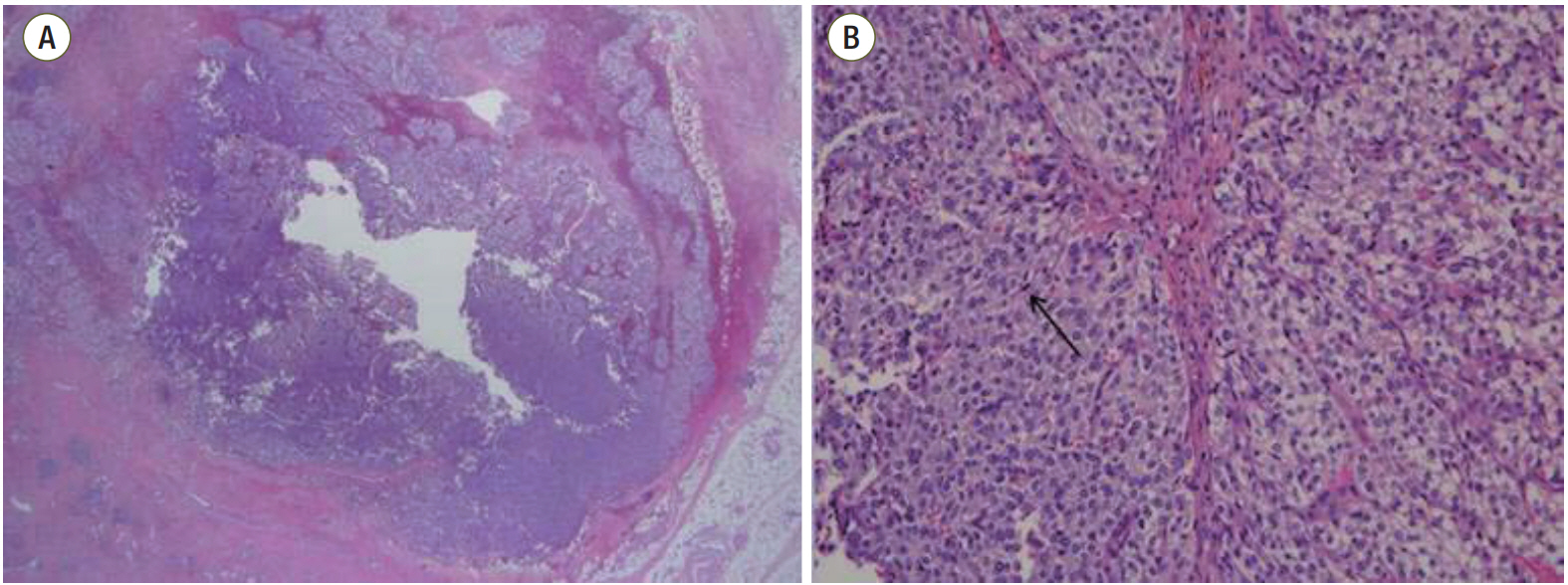
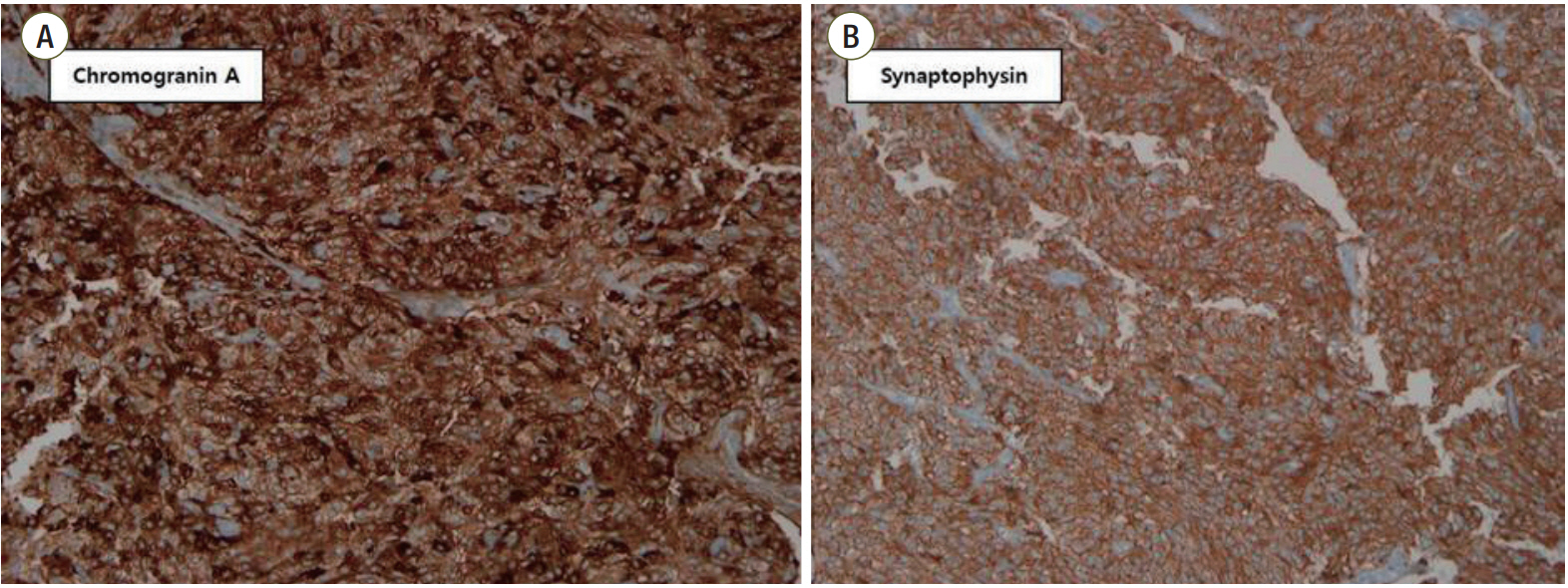
Figure 6.Immunohistochemical staining. Staining was positive for (A) chromogranin A (×200) and (B) synaptophysin (×200).
- 1. Pedroso C, Robalo R, Sereno P, Barros C, Marques C. A rare abdomino-pelvic tumor: paraganglioma. Acta Med Port 2015;28:114-6.ArticlePubMed
- 2. Pałasz P, Adamski Ł, Studniarek M. Paragangliomas: a propos of two cases. Diagnostics and treatment. Pol J Radiol 2015;80:411-6.ArticlePubMedPMC
- 3. Yau KK, Siu WT, Li MK. Unusual cause of acute abdomen: ruptured retroperitoneal paraganglioma. Asian J Surg 2008;31:32-5.ArticlePubMed
- 4. Mahmoudieh L, Saeedinia A, Ahmadpoor P, Temannaie Z, Parvin M, Torbati P, et al. Nephroquiz 8: perioperative management of paraganglioma. Iran J Kidney Dis 2015;9:259-62.PubMed
- 5. Sapienza P, Tedesco M, Graziano P, Moretti M, Mingazzini PL, Cavallaro A. An unusual case of spontaneous rupture of a clinically “silent” phaeochromocytoma. Anticancer Res 1997;17:717-20.PubMed
References
Figure & Data
References
Citations
Citations to this article as recorded by 
- Acute haemoperitoneum caused by ruptured extra‐adrenal paraganglioma
Jae Im Lee, Su Lim Lee, Kyung Jin Seo
ANZ Journal of Surgery.2021;[Epub] CrossRef - Laparoscopic resection of a ruptured retroperitoneal paraganglioma
Shogo Zuo, Toshio Sawai, Hiromichi Kanehiro, Yasuhiro Kuroda, Masayuki Sho
Journal of Pediatric Surgery Case Reports.2020; 59: 101522. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite